대한화상학회지 제 21 권 제 1 호
50
Journal of Korean Burn SocietyVol. 21, No. 1, 50-53, 2018
CASE REPORT
화상 반흔 구축 치료를 위한 부분층 피부 및 무세포 진피 이식: 증례 보고
고성훈ㆍ나웅규ㆍ임효섭ㆍ민수기
1한림대학교 의과대학 한림대학교성심병원 성형외과학교실, 1병리학교실
Acellular Dermal Matrix and Split-Thickness Skin Graft Stabilized by Negative Pressure Wound Therapy for Postburn Scar Contracture: A Case Report
Sung Hoon Koh, M.D., Ph.D., Woong Gyu Na, M.D., Hyoseob Lim, M.D., Ph.D. and Soo Kee Min, M.D., Ph.D.
1 Departments of Plastic and Reconstructive Surgery and 1Pathology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, KoreaPostburn scar contracture for ankle is commonly treated with contracture release procedure and skin graft but contracture re- currence rate is high. Contracture in grafted skin is inversely related to the graft thickness but full-thickness skin graft is limited in large defect coverage. Using ADM for ankle joint defect which was following ankle postburn scar contracture release proce- dure with grafting split-thickness skin may be an alternative reconstructive option. We present a 63-year-old man with post- burn scar contracture and Marjolin ulcer on his left ankle. He originally had limited ankle movement function but surgical re- section of skin malignancy and surrounding scar tissue released the ankle. Coverage using ADM and STSG was performed and NPWT was used for graft fixation. Ankle range of motion was satisfactory at postoperative follow-up. The ADM and STSG with NPWT could be considered an alternative reconstruction option after contracture release for ankle. (J Korean Burn Soc
2018;21:50 -53)
Key Words: Cicatrix, Skin transplantation, Acellular dermis
Received: 2018. 4. 2, Revised: 2018. 5. 16, Accepted: 2018. 5. 25 Corresponding author: Hyoseob Lim, Department of Plastic
and Reconstructive Surgery, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, 22 Gwanpyeong-ro, 170 beon-gil, Dongan-gu, Anyang 14068, Korea
Tel: 82-31-380-3781, Fax: 82-31-380-5980 E-mail: [email protected]
INTRODUCTION
Postburn scar contracture of ankle joints is caused by full-thickness or deep partial-thickness burns
1). Common reconstruction method following contracture release for ankle joint is split-thickness skin graft (STSG) rather than regional or free flap but recurrence rate is high
1). We pres- ent 63-year-old male patient who had successful ankle joint function restoration using acellular dermal matrix (ADM). He was referred with Marjolin ulcers on left an- kle which was occurred on postburn contracure site.
Postburn scar contracture limited range of motion (ROM) initially but wide excision of Marjolin ulcer and adjacent scar tissue released the ankle. Consequent defect was cov- ered by STSG and ADM and nearly full ROM was shown after postoperative several months.
CASE REPORT
A 63-year-old man with hypertension, diabetes mellitus and history of old pulmonary tuberculosis was referred to our department because of a chronic ulceration on his left ankle. He had limited ROM on his left ankle because of scar contracture that had been caused by a burn injury more than 30 years previously. Cicatricial tissue covered his ankle from dorsal surface to lateral malleolar area.
The ulceration located on the anterior ankle area and the
lateral malleolar area developed 6 months before
presentation. Both lesions had irregular pattern of gran-
ulation tissue overgrowth with serous clot (Fig. 1).
Sung Hoon Koh, et al:Acellular Dermal Matrix for Postburn Contracture
51
Fig. 3. Intraoperative photograph showing coverage with ADM
and STSG.Fig. 1. (A) Preoperative photograph showing anterior surface of
left ankle. (B) Preoperative photograph showing lateral malleolar area of left ankle.Fig. 2. Intraoperative photograph of the cicatricial tissue
resection with tumor wide excision.Fig. 4. (A) Postoperative 7 months photograph with full
dorsiflexion. (B) Postoperative 7 months photograph with full planarflexion.Incisional biopsies were performed suspecting skin malignancy. We harvested sufficient tissue and pathologic examination revealed SCC in both lesions. Wide excision with a 1-cm safety margin was performed under general anesthesia. Bony or ligamentous structures were not exposed. After frozen biopsy confirmed negative re- section margin for tumor cell, additional contracture re- lease was also performed (Fig. 2). Adjacent scar tissue was resected as much as possible resulting in improve- ments in joint ROM. After 1 week of vaseline gauze dressing, the entire defect was covered with healthy gran- ulation tissue and reconstruction with an ADM and STSG was planned. Regional flap or free tissue transfer was not considered due to burden of long operation time and the
need for early ambulation considering his age and under- lying disease. Full-thickness skin graft was not appro- priate for coverage as well due to large defect size.
Postoperative joint motion would hinder graft fixation and full-thickness skin would be more difficult to survive.
Under general anesthesia, split-thickness (9/1000-inch
thickness) skin was taken on his left thigh and was ex-
panded with mesh (1:1.5). A 17-cm×6-cm CGDerm
(CGBio, Seong-Nam si, Republic of Korea) was placed on
the anterior surface of ankle where joint motion actively
took place. Expanded split-thickness skin was laid over
the CGDerm spanning the whole defect (Fig. 3). Negative
pressure wound therapy (CuraVAC, CGBio) was used for
52
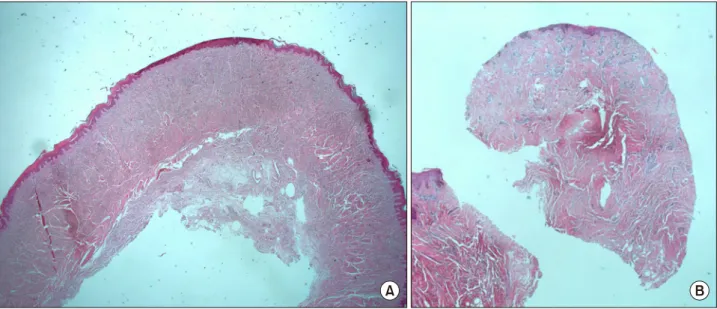
대한화상학회지 Vol. 21, No. 1, 2018Fig. 5. (A) Intraoperative pathologic photograph showing 2.8 mm thickness dermis. (B) Postoperative 10 months pathologic photograph
showing 4 mm thickness dermis.graft fixation with a short-leg splint and was changed ev- ery 3 days. At 1 week postoperatively, NPWT and the splint were removed and ambulation was gradually started. The graft took well, with minimal skin loss at the joint area. The patient was educated about repetitive an- kle movement with full extension and full flexion and tubular elastic garment which was designed to compress the wound and to minimize scar tissue formation.
Postoperative joint ROM was wider than preoperative joint ROM. Postoperative 7 months photograph shows nearly normal ROM from full flexion to full extension with satisfactory skin pliability (Fig. 4). Serial pathologic examinations revealed that skin sampled at postoperative 10 months had thicker dermis (4 mm) with looser colla- gen layer than the cutaneous tissue which was harvested with wide excision (2.8 mm) (Fig. 5).
DISCUSSION
Postburn scar contracture for ankle could be accom- panied with foot and leg deformity and is commonly treated with contracture release procedure and skin graft
1). However, its rest position induces graft tissue con- traction and contracture recurrence is frequent
1). Contracture of autologous grafted skin is known to occur during sec- ondary contraction of the scar that appears between the wound bed and the grafted skin
2). Secondary contraction
is inversely related to the grafted skin thickness, but full-thickness skin grafting is not always possible when the defect is too large
2,3). ADM is a dermal allograft de- rived from several sources including porcine intestinal submucosa, bovine tendon and human collagen
4). Immun- ogenic components are removed and chance for in- flammatory response is low
4). Since commercially released in 1994, ADM has made good results with STSG in con- tracture treatment or prevention
3,5,6). It functions as a scaf- fold for cellular migration and proliferation providing sufficient skin thickness when used with split-thickness skin
4). Hur reported favorable outcomes of the defect area covered by the artificial dermis and split-thickness auto- graft
2). The grafted skin was measured during post- operative follow-up examinations, and minimized con- tracture with artificial dermis was observed
2). In our case, the patient had limited joint function with postburn scar contracture. Removal of cicatricial tissue released the contracture. Coverage with split-thickness skin and CGDerm which is a kind of ADM successfully prevent contracture recurrence and restore the joint ROM.
Additionally, NPWT could be effectively used with
STSG and ADM. CGDerm produced by freeze-drying is
derived from cadaveric human skin
7). Using the natural
human dermis framework, effective ingrowth of dermal
cells may be expected. However, in the literature, a longer
period was required for graft stabilization when the ADM
Sung Hoon Koh, et al:Acellular Dermal Matrix for Postburn Contracture
53
was applied with skin grafts
8). This could be attributed to the increased distance between the grafted skin and nutrients and oxygen diffusion
8). To solve this problem, we used NPWT for the wound. NPWT aids imbibition, inosculation, and neovascularization and prevents sero- mas and hematomas, thereby assisting in graft take
8). NPWT could also improve the graft quality
9). Bioemen et al reported superior scar quality when a split-thickness autograft and dermal substitute (Matriderm) were co-ap- plied with NPWT
9). In our case, grafted skin took well and early ambulation was possible at postoperative 1 week with splint removal. Bed rest status increases risk of deep vein thrombosis, bedsores, pneumonia
10). Early ambulation with reliable graft take using NPWT is benefi- cial for him considering his old age.
In conclusion, combining an ADM and STSG with NPWT to cover the defects caused by ankle postburn scar contracture release resulted in satisfactory postoperative ROM compared with the preoperative status. NPWT helps the graft take and makes early ambulation possible.
The ADM and STSG with NPWT could be considered an alternative reconstruction option with ankle postburn scar contracture release.
REFERENCES
1) Grishkevich VM, Ankle dorsiflexion postburn scar contr- actures: anatomy and reconstructive techniques. Burns. 2012;
38:882-8.
2) Hur GY, Seo DK, Lee JW. Contracture of skin graft in human burns: effect of artificial dermis. Burns. 2014;40:1497-503.
3) Corps BV. The effect of graft thickness, donor site, and graft bed on graft thickness in the hooded rat. Br J Plast Surg.
1969;22:125–133.
4) Hughes OB, Rakosi A, Macquhae F, Herskovitz I, Fox JD, Kirsner RS. A Review of Cellular and Acellular Matrix Products: Indications, Techniques, and Outcomes. Plast Reconstr Surg. 2016;138:138S-47S.
5) Ryssel H, Germann G, Kloeters O, Gazyakan E, Radu CA.
Dermal substitution with Matriderm(Ⓡ) in burns on the dorsum of the hand. Burns. 2010;36:1248-53.
6) Haslik W, Kamolz LP, Manna F, Hladik M, Rath T, Frey M.
Management of full-thickness skin defects in the hand and wrist region: first long-term experiences with the dermal matrix Matriderm. J Plast Reconstr Aesthet Surg. 2010;63:
360-4.
7) Park JY, Lee TG, Kim JY, Lee MC, Chung YK, Lee WJ.
Acellular Dermal Matrix to Treat Full Thickness Skin Defects:
Follow-Up Subjective and Objective Skin Quality Assessments.
Arch Craniofac Surg. 2014;15:14-21.
8) Lee YJ, Park MC, Park DH, Hahn HM, Kim SM, Lee IJ.
Effectiveness of Acellular Dermal Matrix on Autologous Split-Thickness Skin Graft in Treatment of Deep Tissue Defect:
Esthetic Subjective and Objective Evaluation. Aesthetic Plast Surg. 2017;41:1049-1057.
9) Bloemen MC, van der Wal MB, Verhaegen PD, Nieuwenhuis MK, van Baar ME, van Zuijlen PP, et al. Clinical effectiveness of dermal substitution in burns by topical negative pressure:
a multicenter randomized controlled trial. Wound Repair Regen. 2012;20:797-805.
10) Allen C, Glasziou P, Del Mar C., Bed rest: a potentially harmful treatment needing more careful evaluation Lancet.
1999;9:1229-33.