pISSN: 0378-6471 eISSN: 2092-9374 http://dx.doi.org/10.3341/jkos.2013.54.5.829
= 증례보고 =
후부판모양맥락망막염에서의 유리체강내 베바시주멥 선행 치료 후 임상경과
한세훈1⋅임지원1,2
한림대학교 의과대학 춘천성심병원 안과학교실1, 서울동부병원 안과2
목적: 잠복매독에 의한 후부판모양맥락망막염에서 유리체강내 bevacizumab 선행 치료 후 경과를 빛간섭단층촬영과 같이 보고하고자 한다.
증례요약: 43세 여자환자가 내원 3일 전부터 시작된 우안의 시력 저하를 주소로 내원하였다. 안저에서 우안 황반부에 판모양 맥락망막 염이 있었으며 전안부및 유리체에 염증반응은 없었다. 유리체강내 bevacizumab 주사를 시행하면서 전신검사를 시행하였다. 1주일 후 안저에서 황반부 병변은 소실되었으나 스펙트럼 영역 빛간섭단층촬영상 광수용체의 이상은 지속되었다. 혈청학적 검사에서 VDRL 과 FTA-ABS 양성 소견을 보였으며 내과 협진에서 잠복매독으로 최종 진단되어 penicillin 근주를 1주일 간격으로 3회를 시행하였다.
그 후 시력과 외망막층 이상은 점차 호전되었으며 6개월간 경과관찰기간 동안 재발은 없었다.
결론: 후부판모양맥락망막염에서 항생제 치료와 함께 유리체강내 bevacizumab 치료를 고려할 수 있으며 질환의 기전에 대해서는 추 가 연구가 필요하다.
<대한안과학회지 2013;54(5):829-833>
■ 접 수 일: 2012년 6월 15일 ■ 심사통과일: 2012년 10월 2일
■ 게재허가일: 2013년 2월 15일
■ 책 임 저 자: 임 지 원
서울특별시 동대문구 무학로 124 서울동부병원 안과
Tel: 02-920-9178, Fax: 02-920-9219 E-mail: [email protected]
매독은 treponema pallidum 감염에 의한 성적 접촉을 통 해 전염되는 만성 전신염증질환으로 치료를 하지 않을 경 우 전신의 여러 기관에서 다양한 합병증을 일으킬 수 있다.
안내매독은 질환의 시기나 정도에 상관없이 안구 및 안구 부속기 모든 곳에서 나타날 수 있기에 많은 안과 질환에서 중요한 가면성(great masquerade) 질환으로 불리고 있다.1 흔한 안내매독의 양상으로는 간질성각막염, 공막염, 망막혈 관염, 유리체염과 시신경염등이 있으나 포도막염이 가장 흔 한 것으로 알려졌다.2매독성 포도막염은 주로 2기에서 3기 에 많이 나타나며 전체포도막염의 1%를 차지한다.3,4포도막 염 중에서도 후극부를 침범하는 경우는 매독성 포도막염의 8% 정도이며 경도의 유리체염증과 동반되어 나타나는 1/2 에서 1시신경크기의 회색 망막병변이 전형적인 소견이다.5-7 저자들은 단안의 후부판모양맥락망막염이 유일한 양상 으로 나타난 잠복매독 1예에서 유리체강내 bevacizumab 치료 후 빠른 호전을 보인 증례를 경험하였기에 빛간섭단 층촬영 영상과 함께 경과를 보고하고자 한다.
증례보고
43세 여자환자가 내원 3일 전부터 갑작스럽게 시작된 우 안의 시력저하를 주소로 내원하였다. 특별한 기저질환이나 과거력은 없었다. 교정시력은 우안 0.4, 좌안 1.0 이었고 안 압과 동공반사는 정상이었으며 전안부 및 유리체에 염증소 견은 없었다. 안저검사에서 좌안에는 특이소견이 없었으나 우안에 황반부에 크림색의 판상모양의 병변이 발견되었고 작은 점상의 망막출혈이 동반해 있었다. 형광안저촬영에서 초기에는 약한 저형광을 보이다가 후기에 전반적으로 염색 되는 양상을 보였다(Fig. 1). 스펙트럼 영역 빛간섭단층촬 영에서 내망막층은 잘 배열되어 있었으나 외경계막선은 깨 져서 관찰되지 않았으며 광수용체 영역에 저반사층이 보이 고 있었고, 이 저반사층 가장자리 단면에 따라서 뷸규칙한 형태의 고반사물질이 부분부분 채워져 있었다. 맥락막를 관 찰하기 위한 enhanced-depth image (EDI) mode에서는 특히 내측 맥락막 영역에서 불규칙하게 고반사물질들이 채 워져 있는 모양을 보였다(Fig. 2A). 우선 황반부종을 감소 시키기 위하여 유리체강내 bevacizumab 주입술을 시행하 였으며 전신질환 유무를 찾기 위한 검사를 시행하였다.
유리체강내 주사 1주일 후 환자의 우안 시력은 0.7로 호 전되었으며 빛간섭단층촬영상 저반사층은 모두 사라졌지만 외경계막과 광수용체의 내절/외절 경계선은 제대로 배열되 어 있지 않았다(Fig. 2B). 혈액검사에서 백혈구 및 적혈구,
A B
Figure 1. (A) Initial fundus photography of right eye. It showed yellow-white placoid lesion with a retinal hemorrhage in the macula
(B) Late-phase of fluorescein angiography. It revealed a lesion of with well-defined borders and late-staining hyperfluorescence.간기능, 신기능 수치와 톡소플라즈마, herpes simplex vi- rus, varicella zoster virus, cytomegalovirus 및 자가면역 검사(rheumatoid factor, antinuclear antibody), 흉부 X-ray는 정상소견을 보였다. 하지만 erythrocyte sed- imentation rate이 13 mm/h으로 경미하게 증가되어 있었 고, Vernereal Disease Research Laboratory이 1:128로 증 가해 있으면서 Fluorescent treponemal antibody absorbed 가 IgG와 IgM 모두 양성소견을 보였다. 이에 안내매독을 의심하고 감염내과 협진을 의뢰하였다.
내과에서 시행한 추가검사에서 뇌척수액은 매독 음성소 견을 나타내었다. Human immunodeficiency virus도 음성 이었으며 다른 면역이상이나 피부이상, 림프절비대 같은 전 신이상을 발견할 수 없었다. 추가 문진에서 배우자가 피부 과에서 매독 양성으로 페니실린 치료를 초진 2주일 전 받기 시작한 것이 확인되었다.
잠복매독으로 최종 진단되었고 benzathine penicillin G 240만 단위 근육주사 치료를 1주일 간격으로 3회 시행하였 다. 마지막 페니실린 주사 치료를 받던 날 환자는 우안 시 력이 0.7이었으며 스펙트럼 영역 빛간섭단층촬영에서 외경 계막과 광수용체부위의 경계면이 관찰되기 시작하였다. EDI 모드에서도 맥락막의 과반사침착이 호전되었다(Fig. 2C).
경과관찰 6개월 후 시력은 0.9로 좀더 호전되었으며 안저 에서 재발이나 악화의 소견은 발견되지 않았고 다른 염증 의 증후도 관찰되지 않았다.
고 찰
매독은 결막과 공막, 각막, 수정체, 시신경, 망막, 뇌신경 등 안구와 안구부속기 어디에나 발병할 수 있으며 안내매
독 특유의 양상은 정의된 바가 없기에 모든 양상의 안구내 염증에서 배제해야 하는 질환이다. 이중 주로 황반부의 망 막색소상피층에 국한된 큰 판상모양의 병변을 매독성 급성 후부판모양맥락망막염으로 Gass et al3이 명명하였으며 2 기 매독의 비교적 특징적인 양상이라고 하였지만 매우 드 물게 보고되어 있다. 매독은 크게 4기로 나누어지는데 감염 된 후 3개월의 잠복기를 거쳐서 경성하감이 나타나는 시기 를 1기로 보며 경성하감이 사라진 후 혈액을 타고 전신으로 전파되어 손과 발의 구진홍반성 발진, 열, 림프절비대 등이 나타나는 시기를 2기로 본다. 2기에서는 10%에서 안구내 징후가 나타나게 된다. 다음 잠복기를 거쳐서 3기로 진행되 면 생명에도 지장을 줄 수 있는 심혈관질환이나 신경학적 증상이 합병될 수 있으며 잠복매독은 특별한 증상이 없는 시기로 수개월에서 수십 년까지 기간이 매우 다양하다. 특 이하게도 본 증례는 잠복매독으로 최종 진단되었지만 하지 만 각 시기별 증상이 겹쳐지면서 나타날 수 있다는 점을 고 려할 때 안내매독의 진단에 매독의 시기는 주요하지 않은 것으로 보인다.1,2
매독성 급성후부판모양맥락망막염의 병태생리는 아직 명확하지 않다. 유리체강내 스테로이드 주입술 후 발생한 증례와 스테로이드 감량 후 호전된 매독성 후부판모양맥락 망막염의 보고를 미루어서 스테로이드가 면역체계의 조절 에 이상을 일으켜서 질환이 발생하는 것으로 생각되어 스 테로이드는 치료에 금기라고 하였으나 전신 스테로이드 치 료 후의 오히려 질환의 호전도 보고된 바 있기에 이는 결론 지을 수 없다.8-12최근에는 주로 자가면역질환과 관련있는 anti-cardiolipin antibody가 증가된 증례를 토대로 자가면 역반응과의 연관성이 제기된 바 있으며 Brito et al12은 이 항체가 맥락막의 treponema와 결합하여 맥락막 혈전을 일
A
B
C
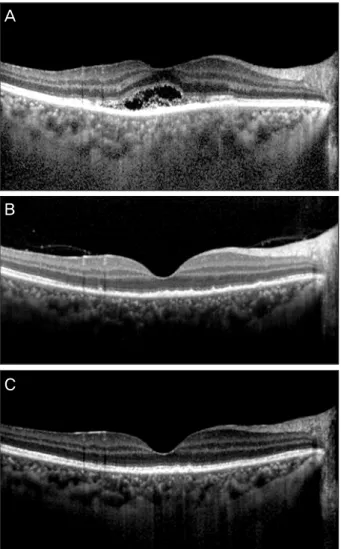
Figure 2. Horizontal section of spectral-domain optical coher-
ence tomography images (A) Image at initial visit using en- hanced-depth image mode. An ill-defined photoreceptor in- ner/outer segment junction and absent external limiting mem- brane were shown. There was hypodensity area arounding an irregular hyperdensity infiltration on outer retina. Choroidal detail revealed irregular, diffuse infiltration of the inner cho- roidal vasculature. (B) Image at 1 week after intravitreal bevacizumab. The hypodensity area was disappeared and pho- toreceptor disarrangement was remained. (C) Image after 1 month after intravitreal bevacizumab injection using en- hanced-depth image mode. Restored stratification of the outer retinal layers and well-defined numerous choroidal vascular space were shown.으키고 망막색소상피의 대사에 장애를 유발함으로서 빛간 섭단층촬영에서 보이는 광수용체 이상을 초래한 것이라고 하였다. 본 증례에서는 anti-cardiolipin antibody를 측정하 지 않았으나 항생제 치료가 완료된 후에도 시력과 특히 맥 락막 영상의 호전은 서서히 일어나는 점은 비슷하였다. 또 한 과거에는 인체면역결핍바이러스 양성 같은 면역저하자 에서만 발생한다고 생각하였으나 본 증례에서처럼 정상면
역을 가진 환자에서의 보고도 있어서 면역억제상태와는 관 련이 없는 것으로 생각되고 있다.13
과거 시간 영역 빛간섭단층촬영 보고에서는 단순한 황반 두께증가나 망막색소상피층의 반사도 증가, 간혹 동반되는 삼출망막박리 소견만이 보고되었는데 본 증례에서는 스펙 트럼 영역 빛간섭단층촬영을 시행하여 망막층을 좀더 자세 히 분석할 수 있었다.14 내망막의 층화현상은 잘 보존되어 있었으며 이상소견은 외망막층의 맥락막/망막색소상피세포 영역에 국한되어 있었다. 외경계막 및 광수용체내절/외절 경계면이 무너져서 관찰되지 않았으며 특히 광수용체가 분 리되면서 저반사층이 나타났고 저반사층 주위에 불규칙한 형태의 고반사물질들의 침착이 관찰되었다. 이 저반사층은 기존 매독성 급성후부판모양맥락망막염에서는 보고되지 않 았던 소견인 점이 흥미롭다. 이 고반사물질들이 광수용체의 분절들인지 염증성 물질의 침착인지는 불명확하여 추가 연 구가 필요할 것으로 생각된다. 또한 EDI mode로 얻은 맥락 막영상에서는 특히 내측 맥락막혈관부위에서 고반사물질의 침착을 관찰할 수 있었다. 매독성 급성후부판모양맥락망막 염에서의 인도시아닌안저촬영 연구에서 병변부위는 저형광 으로 나타나며 안저에서 병변이 사라진 후에도 인도시아닌 촬영에서의 저형광은 지속되었던 점이 특징이었다.15,16 이 소견은 흰반점증후군 같은 안내염증에서 나타나는 소견으 로 이와 유사하게 맥락막내 염증성 물질의 침착과 허혈변 화가 합병되어 나타난 것으로 추측한다. 따라서 anti-car- diolipin antibody 관련 보고와 흰반점증후군과의 유사점을 종합하면 자가면역반응의 일종이 질환의 발생에 관여하였 을 것으로 생각한다.
매독의 치료는 240만 단위 Benzathine penicillin G의 단 독 근주가 1, 2차 및 초기 잠복 매독의 치료로 추천되고 있 으며, 후기 잠복 매독과 3차 매독의 치료로는 1주 간격으로 240만 단위 Benzathine penicillin G를 3회 근주하는 것이 추천된다.본 증례에서는 매독이 진단되기 전 황반부 부종 을 감소시키기 위하여 유리체강내 bevacizumab 주입술을 선행하였으며 다른 치료 없이도 1주일 후 시력 향상과 망막 내 저반사층의 소실을 관찰할 수 있었다. 하지만 광수용체 의 재배열과 맥락막의 고반사도는 1달에 걸쳐서 서서히 호 전되었으며 이는 시력의 상대적으로 더딘 회복과 관련이 있었다고 생각한다. 질환의 근본 원인인 매독균의 근절이 치료에 필수적이므로 페니실린 치료를 추가로 시행하였으 며 그 후 재발은 없었다. Bevacizumab 같은 Anti-vascular endothelial growth factor (VEGF) 유리체강내 주사는 맥 락막신생혈관뿐만 아니라 당뇨망막병증이나 망막혈관폐쇄 증과 같은 다양한 황반질환에 쓰이는 치료법이다. 포도막염 에서는 염증에 의한 혈액안구장벽의 파괴로 여러 매개물질
이 증가하면서 황반부종을 일으키는데 포도막염으로 인한 황반부종 환자의 전방수에서 VEGF의 발현의 증가가 보고 되었기에 VEGF가 하나의 치료 목표가 될 수 있다고 하였
다.17,18이에 여러 종류의 포도막염으로 인한 황반부종에서
유리체강내 anti-VEGF 치료는 효과적이라고 보고되어 있
다.19-21 저자들은 환자의 빠른 회복을 목표로 유리체강내
bevacizumab 주사를 선행치료로 사용하여 다른 치료 없이 1주일 후 호전됨을 관찰하였으나 매독과 VEGF 발현에 관 련된 보고는 아직까지 없으며 매독성 급성후부판모양맥락 망막염의 불명확한 병태생리를 생각하면 유리체강내 bev- acizumab의 효과와 기전에 대해서는 더 많은 환자 수를 통 한 추가연구가 필요하다. 또한 유리체강내 bevacizumab의 효과는 단기간 황반부종의 호전에 국한될 것이며 매독의 근본적인 치료는 매독균을 없애는 페니실린 항생제 치료임 은 반드시 주지하여야 한다.
요약하면 후부판모양맥락망막염만이 유일한 임상양상으 로 나타난 잠복매독 1예를 경험하였으며 유리체강내 bev- acizumab 주입술을 선행치료로 시행하여 빠른 시력 호전을 이룰 수 있었다. 이에 스펙트럼 영역 빛간섭단층촬영 결과 와 함께 보고하는 바이다.
참고문헌
1) Aldave AJ, King JA, Cunningham ET Jr. Ocular syphilis. Curr Opin Ophthalmol 2001;12:433-41.
2) Kiss S, Damico FM, Young LH. Ocular manifestations and treat- ment of syphilis. Semin Ophthalmol 2005;20:161-7.
3) Gass JD, Braunstein RA, Chenoweth RG. Acute syphilitic posteri- or placoid chorioretinitis. Ophthalmology 1990;97:1288-97.
4) Tamesis RR, Foster CS. Ocular syphilis. Ophthalmology 1990;
97:1281-7.
5) Villanueva AV, Sahouri MJ, Ormerod LD, et al. Posterior uveitis in patients with positive serology for syphilis. Clin Infect Dis 2000;
30:479-85.
6) Barile GR, Flynn TE. Syphilis exposure in patients with uveitis.
Ophthalmology 1997;104:1605-9.
7) Durnian JM, Naylor G, Saeed AM. Ocular syphilis: the return of an old acquaintance. Eye (Lond) 2004;18:440-2.
8) Zamani M, Garfinkel RA. Corticosteroid-induced modulation of acute syphilitic posterior placoid chorioretinitis. Am J Ophthalmol 2003;135:891-4.
9) Tran TH, Cassoux N, Bodaghi B, et al. Syphilitic uveitis in patients infected with human immunodeficiency virus. Graefes Arch Clin Exp Ophthalmol 2005;243:863-9.
10) Erol N, Topbas S. Acute syphilitic posterior placoid chorioretinitis after an intravitreal triamcinolone acetonide injection. Acta Ophthalmol Scand 2006;84:435.
11) Yoo C, Kim SK, Huh K, Oh J. Atypical acute syphilitic posterior placoid chorioretinitis. Korean J Ophthalmol 2009;23:108-11.
12) Brito P, Penas S, Carneiro A, et al. Spectral-domain optical coher- ence tomography features of acute syphilitic posterior placoid cho- rioretinitis: the role of autoimmune response in pathogenesis. Case Report Ophthalmol 2011;25:39-44.
13) Joseph A, Rogers S, Browning A, et al. Syphilitic acute posterior placoid chorioretinitis in nonimmuno-compromised patients. Eye (Lond) 2007;21:1114-9.
14) Chen J, Lee L. Posterior placoid chorioretinitis: An unusual ocular manifestation of syphilis. Clin Ophthalmol 2008;2:669-73.
15) Baglivo E, Kapetanios A, Safran AB. Fluorescein and indocyanine green angiographic features in acute syphilitic macular placoid chorioretinitis. Can J Ophthalmol 2003;38:401-5.
16) Meira-Freitas D, Farah ME, Höfling-Lima AL, Aggio FB. Optical coherence tomography and indocyanine green angiography find- ings in acute syphilitic posterior placoid choroidopathy: case report. Arq Bras Oftalmol 2009;72:832-5.
17) Campochiaro PA. Targeted pharmacotherapy of retinal diseases with ranibizumab. Drugs Today (Barc) 2007;43:529-37.
18) Cordero Coma M, Sobrin L, Onal S, et al. Intravitreal bevacizumab for treatment of uveitic macular edema. Ophthalmology 2007;
114:1574-9.
19) Ossewaarde-van Norel A, Rothova A. Clinical review: Update on treatment of inflammatory macular edema. Ocul Immunol Inflamm 2011;19:75-83.
20) Gulati N, Forooghian F, Lieberman R, Jabs DA. Vascular endothe- lial growth factor inhibition in uveitis: a systematic review. Br J Ophthalmol 2011;95:162-5.
21) Modorati G, Miserocchi E. Intravitreal injection therapy in the treatment of noninfectious uveitis. Dev Ophthalmol 2012;51:110-21.
=ABSTRACT=
Clinical Course Following Intravitreal Bevacizumab Injection in Posterior Placoid Chorioretinitis
Se Hoon Han, MD1, Ji Won Lim, MD, PhD1,2
Department of Ophthalmology, Hallym University Chuncheon Sacred Heart Hospital, Hallym University College of Medicine1, Chuncheon, Korea Department of Ophthalmology, Seoul Metropolitan Dongbu Hospital2, Seoul, Korea
Purpose: To report the clinical course with optical coherence tomography findings following intravitreal bevacizumab in- jection in patients with posterior placoid chorioretinitis due to latent syphilis.
Case summary: A 43-year-old woman presented with visual dimness in the right eye 3 days in duration. Fundus examination showed yellow, placoid lesions in the right eye and there was no cell reaction in the anterior chamber and vitreous. An intravitreal bevacizumab injection was given and systemic work-up performed. After 1 week, the macular lesion disappeared. However, photoreceptor disarrangement was present on spectral-domain optical coherence tomography image. On serologic test, the Venereal Disease Research Laboratory test, and fluorescent treponemal antigen absorption test were positive. She was referred to a division of infectious diseases and confirmed as latent syphilis. The patient received intramuscular pen- icillin 3 times weekly. Visual acuity and outer retinal abnormality further improved and there was no recurrence during the 6-month follow-up.
Conclusions: Intravitreal bevacizumab injection added to antibiotic treatment may be considered for treating patients with posterior placoid chorioretinitis. Further studies are necessary to evaluate precise disease mechanisms and treatment.
J Korean Ophthalmol Soc 2013;54(5):829-833
Key Words: Chorioretinitis, Posterior placoid chorioretinitis, Spectral-domain optical coherence tomography, Syphilis
Address reprint requests to Ji Won Lim, MD, PhD
Department of Ophthalmology, Seoul Metropolitan Dongbu Hospital
#124 Muhak-ro, Dongdaemun-gu, Seoul 130-707, Korea
Tel: 82-2-920-9178, Fax: 82-2-920-9219, E-mail: [email protected]