pISSN: 0378-6471⋅eISSN: 2092-9374
http://dx.doi.org/10.3341/jkos.2014.55.7.1093
Case Report
노른자모양황반변성 환자에서 유리체강내 베바시주맙 주입술을 시행한 환자 1예
A Case of Adult‐Onset Vitelliform Dystrophy Treated with Intravitreal Injection of Bevacizumab
문상우1,2⋅이호영3⋅윤일한1⋅임성협1,2
Sang Woo Moon, MD1,2, Ho Young Lee, MD3, Il Han Yun, MD, PhD1, Sung Hyup Lim, MD1,2
인제대학교 의과대학 부산백병원 안과학교실1, 안신생혈관질환 치료기술 개발센터2, 신세계 안과의원3 Department of Ophthalmology, Inje University Busan Paik Hospital, Inje University College of Medicine1, Busan, Korea
Therapeutics Center for Ocular Neovascular Disease2, Busan, Korea Shinsegae Eye Clinic3, Busan, Korea
Purpose: To report a patient diagnosed with adult-onset vitelliform dystrophy (AOVD) who received an intravitreal injection of bevacizumab in both eyes.
Case summary: A 47-year-old female presented with blurred vision and metamorphopsia in both eyes. On color fundus photo- graph, small, round, yellowish dots on the foveola and subreitnal fluid were observed. Optical coherence tomography (OCT) showed thick hyperreflective structures in the retinal pigment epithelium (RPE) layer with serous retinal detachment and sub- retinal fluid. Despite an intravitreal injection of bevacizumab on both eyes, anatomical improvement was not observed on fundus photography and OCT.
J Korean Ophthalmol Soc 2014;55(7):1093-1098 Key Words: Bevacizumab, Vitelliform macular dystrophy
■Received: 2013. 10. 26. ■ Revised: 2014. 1. 20.
■Accepted: 2014. 6. 9.
■Address reprint requests to Sung Hyup Lim, MD
Department of Ophthalmology, Inje University Busan Paik Hospital, #75 Bokji-ro, Busanjin-gu, Busan 614-735, Korea Tel: 82-51-890-6015, Fax: 82-51-890-6329
E-mail: [email protected]
* This study was presented as a poster at the 110th Annual Meeting of the Korean Ophthalmological Society 2013.
ⓒ2014 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
성인에서 발병한 노른자모양황반변성(Adult-onset vitelli- form macular dystrophy, AOVD)은 양측성으로 점진적인 시력저하를 초래하는 무늬 황반 변성(pattern macular dys- trophy)이다. 임상적으로 AOVD는 양측 황반부에 망막색소 상피층의 리포퓨신(lipofucin)에서 기인한 둥근 모양의 황색
침착물을 특징으로 한다.
이 질환의 첫 증상은 시력장애를 대게 초래하지 않으나 환자는 약간의 시야 흐림이나 변시증을 호소할 수도 있다. 병이 후기로 진행하여 병변이 분리되거나 조각날 경우 환 자는 시력저하를 호소할 수 있다. 조각 난 병변은 망막색소 상피의 지도모양위축 또는 맥락막 신생혈관 막으로 진행할 수도 있으며, 종종 연령관련황반변성에서 보이는 위축성 망막변화와 비슷하게 보일 수 있다.1
혈관내피세포성장 억제제 중 하나인 베바시주맙(Bevaci- zumab, AVASTIN®, Genentech Inc., San Francisco, CA, USA) 은 혈관내피성장인자의 인간단클론 항체로서 신생혈관 생 성을 억제하는 기능이 있으며, 황반부종의 치료에 유의한 효과가 있다고 알려졌다.2-6
아직 명확한 치료법이 밝혀지지 않은 AOVD 환자에서
Figure 1. Color fundus photograph of a 47-year-old female showing a small, round, yellowish dot at the site of the foveola or a tiny
honeycomb structure centrally (A, B). In fluorescence angiography reveals early blockage and late intense hyperfluorescent circles with hypofluorescent central zones (C, D).맥락막 신생혈관막이 동반된 경우 베바시주맙 주입을 통해 성공적인 시력회복을 보인 증례가 보고되고 있으며, Lee et al7은 맥락막 신생혈관이 동반되지 않은 AOVD환자에서 유 리체강 내 베바시주맙 주입술로 성공적으로 치료한 사례를 보고하였다. 병변의 황색 침착물은 점진적으로 감소하는 양상을 보이며, 광간섭단층촬영에서도 망막하액이 완전히 호전되는 양상을 보였다. 그러나 이러한 해부학적인 호전 에도 불구하고 환자는 여전히 시력저하를 호소하였다.7
위의 증례 보고에 따라 저자들은 본원에 내원하여 AOVD을 진단받은 환자에게 유리체강 내 베바시주맙 주입술을 시행을 한 후 광간섭단층촬영 및 안저 검사, 안구전위도 검사를 통해 황반부 병변의 변화 및 임상양상에 대해서 알아보았다.
증례보고
47세 여성 환자가 양안 시야 흐림 및 변시증을 주소로 외
래로 내원하였다. 최대 교정시력은 우안 20/20, 좌안 20/25 였으며 안압은 양안 모두 14 mmHg이며 전안부 검사에는 특별한 이상소견은 보이지 않았다. 안저검사에서 양안에서 작고 둥근 노란색 반점이 망막중심속오목 근처에서 보이며 황반부 하액이 축적된 양상을 보였다. 형광안저혈관조영술 에서 초기 형광차단이 보며 후기에 저형광을 가진 중심부 위를 가진 과형광고리를 보였다(Fig. 1).
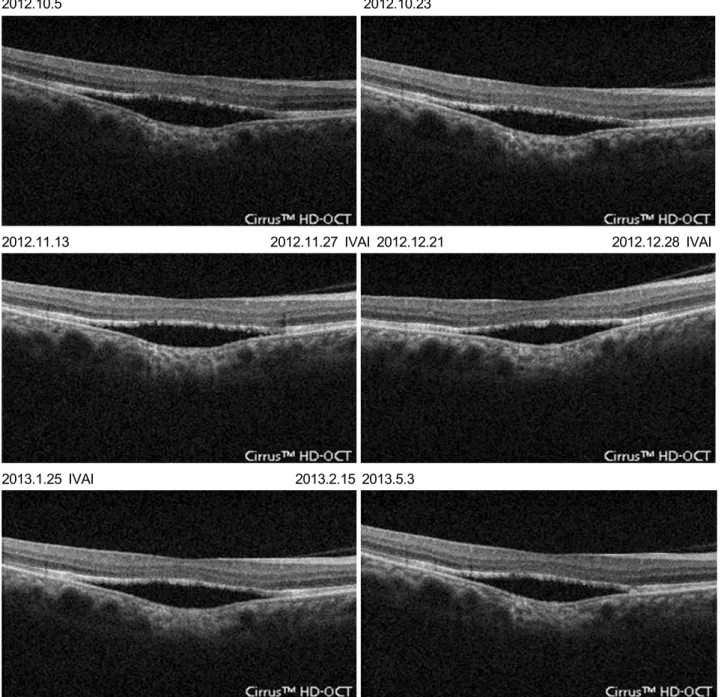
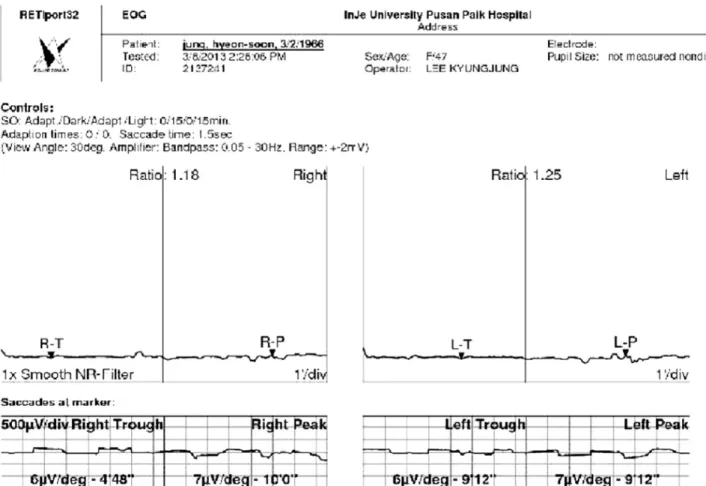
광간섭단층촬영에서 망막색소상피를 따라 두꺼운 과반향 병변(hyperreflective lesion)이 보이며 이와 함께 신경 망막 박리가 동반되었다(Fig. 2, 3). 망막전위도 검사는 정상 소견 을 보였다. 눈전위도 검사에서 양안에서 아르덴비(Arden ra- tio)가 우안 1.18, 좌안 1.25로 감소를 보였다(Fig. 4).
이 환자는 전 노른자 모양 단계의 AOVD로 진단을 내렸 으며, 환자에게 아바스틴의 잠재적 위험과 장점을 설명한 후 Lee et al7의 보고에 따라 양안 유리체강 내 베바시주맙 주입술을 시행하였다. 먼저 좌안에 시행하였으며 각각 1개
A B
C D
2012.10.5 2012.10.23
2012.11.13 2012.11.27 IVAI 2012.12.21 2012.12.28 IVAI
2013.1.25 IVAI 2013.2.15 2013.5.3
Figure 2. Right eye optical coherence tomography (OCT) represents thick hyperreflective structures in the retinal pigment epi-
thelium (RPE) layer and serous retinal detachment and subretinal fluid. OCT after the intravitreal bevacizumab showing no differ- ence of subretinal fluid volume or extent of serous retinal detachment and hyperreflective lesions. IVAI = intravitreal avastin injection.월, 2개월 뒤 두 번의 추가적인 주사를 시행하였으며, 좌안 의 해부학적 호전은 없었으나 시력 향상을 느끼며 우안의 유리체강 내 베바시주맙 주입술을 원하여 한 달 간격으로 3번의 주사를 시행하였다.
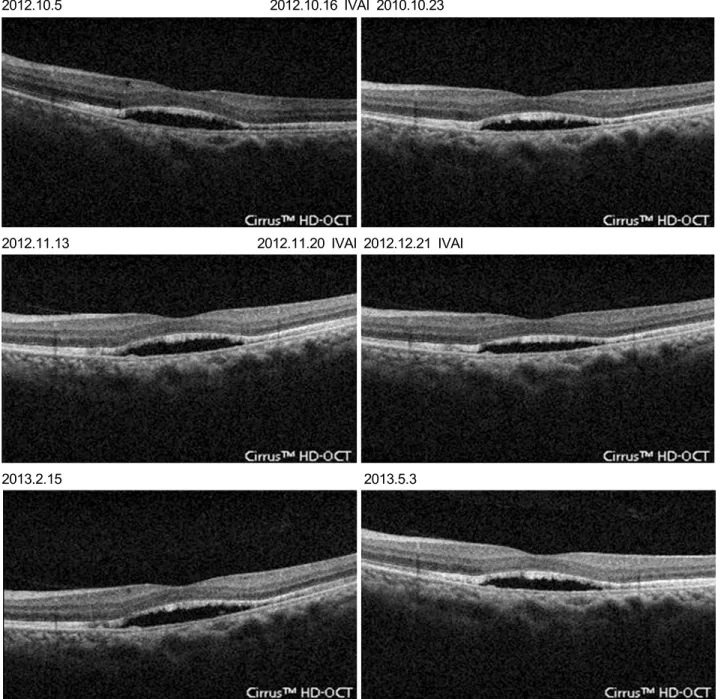
각각 광간섭단층촬영과 최대교정시력을 통해 경과관찰을 한 결과 3차례 아바스틴 시행한 양안 모두 망막하액의 감소 는 보이지 않았으며 망막색소상피를 따라 있는 과반향 병변 도 변화가 없었으며, 최대교정시력도 변화 없었다(Fig. 2, 3).
안저 검사에서도 처음 내원 당시와 치료 후 차이를 발견하 지 못했다. 하지만 환자가 주관적으로 호소하는 시야 흐림 및 변시증은 호전을 보였다.
고 찰
노른자모양환반변성은 상염색체 우성으로 유전하는 드 문 질환이다. 이 질환은 어느 나이에서나 발병이 가능하지
2012.10.5 2012.10.16 IVAI 2010.10.23
2012.11.13 2012.11.20 IVAI 2012.12.21 IVAI
2013.2.15 2013.5.3
Figure 3. Left eye optical coherence tomography (OCT) also represents abnormal findings as described above on the right eye. OCT
was performed after the intravitreal bevacizumab, there were also no difference of subretinal fluid volume or extent of serous retinal detachment and hyperreflective lesions. IVAI = intravitreal avastin injection.만 3-15세 사이에 젊은 나이게 유병된 경우 베스트 노른자 모양 황반변성(Best vitelliform macular dystrophy)으로 명 명되며, 30-50세 사이에 유병된 경우 AOVD로 진단되어 서 로 임상적인 차이를 보이게 된다. 그러나 최근에는 두 질환 모두 Best1 유전자 이상에 의해 나타나며, 주된 원인으로 망막색소상피의 가쪽바닥막에 위치한 Ca2+통로인 베스트로 핀(bestropin)의 기능 이상이라고 알려졌다.8-12
노른자모양황반변성에서 전형적인 안저 소견은 양측 황 반부에 노른자 모양의 둥근 병변이 발견되는 것이다. 망막
에서 침착물의 정확한 위치는 명확히 알려져 있지 않지만 spectral domain 광간섭단층촬영에 근거하여 신경 망막 아 래에 위치하며 이로 인해 광수용체의 안쪽 및 바깥 분절의 변화를 초래하는 것으로 알려졌다. 노른자 모양의 물질 침착 의 정확한 이유는 알려져 있지 않지만 포식되지 않은 광수용 체 바깥 분절의 축적에 의한 것으로 생각한다. 이렇게 망막 하 공간에 축적된 물질은 리포푸신(lipofucin) 전구체 형성을 증가하려는 경향을 보이게 되고 이는 산화 손상(oxidative damage)에 취약하게 만든다.13-16
Figure 4. Electrooculography (EOG) showed decrease in the Arden ratio (light-dark ratio), 1.16 in the right eye and 1.25 in the left eye.
R-T = right trough; R-P = right peak; L-T = left trough; L-P = left peak.
베바시주맙은 혈관내피성장인자(Vascular Endothelial Growth Factor, VEGF)와 강하게 결합할 수 있는 단일클론항체로 혈 액-망막장벽을 강화하며 혈관투과성을 개선하고, 또한 혈관 내피성장인자로 인한 혈관내피세포증식과 신생혈관 생성 을 줄일 수 있다고 알려졌다.5-6
위 이론에 근거하여 베바시주맙이 망막하액의 정도를 감 소시킴으로써 망막색소상피에 의한 포식작용를 촉진하는 데 중요한 역할을 하는 것으로 생각하고 Lee et al7은 노른 자모양황반변성 환자에게 유리체강 내 베바시주압 주입술 을 시행한 것으로 생각한다.
위 이론 및 증례보고에 근거하여 효과를 기대하고 본원 에 내원한 환자에게 유리체강 내 베바시주맙 주입술을 시 행하였다. 하지만 Lee et al7이 보고한 증례와는 달리 위 환 자에서는 안저 소견의 변화는 보이지 않았으며, 광간섭단 층촬영에서도 망막하액 및 망막색소상피와 광수용체층 사 이에 존재하는 과반향를 보이는 병변의 호전을 확인하지 못하였다.
잠재 맥락막 신생혈관막이 동반된 AOVD 환자에서 유리 체강 내 베바시주맙 주입술이 시력회복에 성공적인 결과를
얻었다고 증례가 보고된 경우도 있었다.17,18 그 외에 레이저 광응고요법, 코르티코스테로이드, 비타민 A, E, 광역학치료 등 여러 시도가 이뤄졌으나 모두 AOVD에서 의미 있는 효 과는 없는 것으로 알려졌으며,17 아직까지 AOVD에 확립된 특별한 치료법은 없으며, 1년에 한두 번씩 안과검진을 받도 록 권장하고 있다.
노른자모양황반변성에서 유리체강 내 베바시주맙 주입 술이 효과가 있었다는 보고가 있긴 하지만, 우리는 맥락막 신생혈관을 동반한 노른자모양황반변성에서만 베바시주맙 의 약리적 효과가 발생할 것이라고 추정한다. 최근 국내에 서 몇몇의 연구자들이 노른자모양황반변성의 치료에 유리 체강 내 베바시주맙 주입술을 시도하는 것으로 보이며, 임 상 연구자들이나 환자들에게 정확한 정보를 제공할 수 있 도록 여러 기관에서의 시술 사례를 모아서 분석해 보는 것 이 의미가 있을 것이다.
마지막으로 AOVD의 경우 예후는 대부분 좋은 것으로 알려졌으며, 시력저하는 비교적 느리게 진행하며, 대부분의 환자는 질병의 후기가 되어서도 적어도 한 눈에서는 적절 한 시력을 유지한다고 알려졌다. 하지만 시력저하 및 상실
= 국문초록 =
노른자모양황반변성 환자에서 유리체강내 베바시주맙 주입술을 시행한 환자 1예
목적: 성인에서 발병한 노른자모양황반변성(Adult-onset vitelliform macular dystrophy, AOVD)을 진단받은 환자에게 유리체강 내 베 바시주맙 주입술을 시행을 한 1예를 보고하고자 한다.
증례요약: 47세 여성 환자가 양안 시야 흐림 및 변시증을 주소로 외래로 내원하였다. 안저 검사에서 양안에서 작고 둥근 노란색 반점이 망막중심속오목 근처에서 보이며 황반부 하액이 축적된 양상을 보였다. 광간섭단층촬영에서 망막색소상피를 따라 두꺼운 과반향 병 변(hyperreflective lesion)이 보이며 이와 함께 신경 망막박리가 동반되었다. 양안에 각각 3차례 유리체강 내 베바시주맙 주입술을 시행 후 광간섭단층촬영 및 안저 검사에서 병변의 호전을 보이지 않았다.
<대한안과학회지 2014;55(7):1093-1098>
의 가능성이 있음을 환자에게 설명하고, 삶의 질을 위해 저 시력과 관련된 재활치료에 대한 정보를 제공할 필요가 있 을 것으로 생각한다.
REFERENCES
1) Do P, Ferrucci S. Adult-onset foveomacular vitelliform dystrophy.
Optometry 2006;77:156-66.
2) Funk M, Kriechbaum K, Prager F, et al. Intraocular concentrations of growth factors and cytokines in retinal vein occlusion and the ef- fect of therapy with bevacizumab. Invest Ophthalmol Vis Sci 2009;
50:1025-32.
3) Wu L, Martínez-Castellanos MA, Quiroz-Mercado H, et al. Twelve- month safety of intravitreal injections of bevacizumab (Avastin):
results of the Pan-American Collaborative Retina Study Group (PACORES). Graefes Arch Clin Exp Ophthalmol 2008; 246:81-7.
4) Kreutzer TC, Alge CS, Wolf AH, et al. Intravitreal bevacizumab for the treatment of macular oedema secondary to branch retinal vein occlusion. Br J Ophthalmol 2008;92:351-5.
5) Rabena MD, Pieramici DJ, Castellarin AA, et al. Intravitreal bev- acizumab (Avastin) in the treatment of macular edema secondary to branch retinal vein occlusion. Retina 2007;27:419-25.
6) Matsumoto Y, Freund KB, Peiretti E, et al. Rebound macular ede- ma following bevacizumab (Avastin) therapy for retinal venous oc- clusive disease. Retina 2007;27:426-31.
7) Lee JY, Lim J, Chung H, et al. Spectral domain optical coherence tomography in a patient with adult-onset vitelliform dystrophy treated with intravitreal bevacizumab. Ophthalmic Surg Lasers Imaging 2009;40:319-21.
8) Petrukhin K, Koisti MJ, Bakall B, et al. Identification of the gene
responsible for Best macular dystrophy. Nat Genet 1998;19:241-7.
9) Marmorstein AD, Marmorstein LY, Rayborn M, et al. Bestrophin, the product of the Best vitelliform macular dystrophy gene (VMD2), localizes to the basolateral plasma membrane of the reti- nal pigment epithelium. Proc Natl Acad Sci U S A 2000;97:12758-63.
10) Sun H, Tsunenari T, Yau KW, Nathans J. The vitelliform macular dystrophy protein defines a new family of chloride channels. Proc Natl Acad Sci U S A 2002;99:4008-13.
11) Boon CJ, Klevering BJ, Leroy BP, et al. The spectrum of ocular phenotypes caused by mutation in the BEST1 gene. Prog Retin Eye Res 2009;28:187-205.
12) Booij JC, Boon CJ, van SChooneveld MJ, et al. Course of visual decline in relation to the BEST1 genotype in vitelliform macular dystrophy. Ophthalmology 2010;117:1415-22.
13) Jarc-Vidmar M, Kraut A, Hawlina M. Fundus autofluorescence imaging in Best’s vitelliform dystrophy. Klin Monatsbl Augenheilkd 2003;220:861-7.
14) Gass JDM. Stereoscopic atlas of macular diseases: diagnosis and treatment, 4th ed. St. Louis: Mosby, 1997;304-11.
15) Deutman AF, Hoyng CB. Macular dystrophies. In: Ryan SJ, Ogden TE, Hinton DR, et al, eds. Retina, 3rd. Vol. 2. St. Louis: Mosby, 2001;1210-57.
16) Spaide RF, Noble K, Morgan A, Freund KB. Vitelliform macular dystrophy. Ophthalmology 2006;113:1392-400.
17) Montero JA, Ruiz-Moreno JM, De La Vega C. Intravitreal bev- acizumab for adult-onset vitelliform dystrophy: a case report. Eur J Ophthalmol 2007;17:983-6.
18) Abengoechea-Hernandez S, Elizalde-Montagut J, Fideliz de la Paz-Dalisay M. Photodynamic therapy in adult-onset foveo- macular vitelliform dystrophy. Arch Soc Esp Oftalmol 2007;82:
117-20.