Korean Circulation Journal
Introduction
Hypertension (HT) is a major global public health burden,
1)and it is an important risk factor for cardiovascular disease (CVD) and
cerebrovascular accident.
2)Prehypertensive subjects are at risk of progression to HT, and prehypertension is associated with excessive morbidity and mortality due to CVD.
3)Echocardiography is an important non-invasive diagnostic tool for investigation of left ventricular function. Left ventricular diastolic dysfunction due to various myocardial diseases occurs frequently in hypertension, and it is a common cause of heart failure in patients with hypertension.
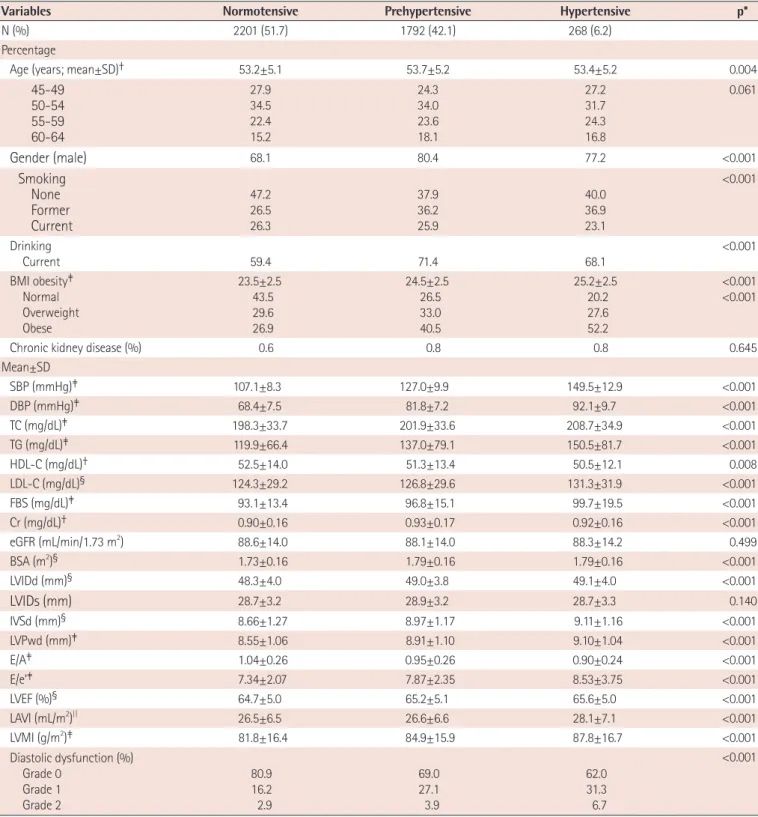
4)However, few studies have shown an association between diastolic dysfunction grade and blood pressure classification, especially mild hypertension or prehypertension (preHT). We sought to investigate the association between diastolic dysfunction and preHT in apparently healthy middle-aged adults.
Subjects and Methods
Study population and protocol
The present study included 4261 Koreans (male:female ratio 7:3),
Print ISSN 1738-5520 • On-line ISSN 1738-5555
Prehypertension and Left Ventricular Diastolic Dysfunction in Middle-Aged Koreans
Shin Yi Jang, PhD 1 , Sujin Kim, BSN 1 , Chang Kwan Lee, PhD 2 , Eun Jeong Cho, MD 3 , Soo Jin Cho, MD 4 , and Sang-Chol Lee, MD 1
1