서론
만성폐쇄성폐질환(chronic obstructive pulmonary
dis-ease, COPD) 치료의 목표는 증상완화, 운동능력 향상, 삶의
질 향상과 급성악화 감소, 질병진행 예방 및 사망률 감소에
있다. 원인이 있는 경우 이를 제거하고 규칙적인 병원 방문
을 유도하여 위험인자, 병의 진행 정도, 약물효과 및 부작용,
급성악화, 동반 질환의 진행 정도를 평가하고 추적 관찰해야
한다. 또한 COPD 환자가 건강한 생활을 유지할 수 있도록 영
양, 육체적 활동, 재활요법, 급성악화 시의 대처법 등에 대한
조언과 교육을 해야 한다. 흡연은 COPD의 가장 중요한 위험
인자로 환자가 금연할 수 있도록 권하고 작업장에서의 분진,
유해가스에 노출되지 않도록 조언해야 한다. 최근 10여 년간
다양한 약제의 임상결과들이 발표되었고 국내에서도 많은 약
제들이 소개되었다. 적절한 약물 치료는 환자의 폐기능 증가,
증상완화, 운동능력, 삶의 질 향상과 급성악화의 감소에 도
움을 주지만 COPD 질환으로 인한 FEV
1의 연간 감소율 저하
와 사망률 개선에 도움이 된다는 증거는 아직까지 없다[1,2].
국내 COPD 진료지침 2018을 개정하였으며, 최근 COPD
치료에 변화와 발전을 가져온 주요 약물 중 국내에 유용한 약
제의 소개, 국내 보험기준과 국내 가이드라인을 소개하고자
한다[3].
만성폐쇄성폐질환의 약물요법
김 인 애1·박 용 범1,2·유 광 하3 | 한림대학교 의과대학 1강동성심병원 호흡기알레르기내과, 2폐연구소, 3건국대학교 의과대학 호흡기 알레르기내과Pharmacotherapy for chronic obstructive
pulmonary disease
In Ae Kim, MD1·Yong Bum Park, MD1,2·Kwang Ha Yoo, MD3
1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Kangdong Sacred Heart
Hospital, Hallym University College of Medicine, Seoul; 2Lung Research Institute, Hallym University College of Medicine, Chuncheon; 3Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea
Received: August 13, 2018 Accepted: August 20, 2018 Corresponding author: Yong Bum Park
E-mail: [email protected] © Korean Medical Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons. org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
The goals of management of stable chronic obstructive pulmonary disease (COPD) are to reduce both current symptoms and future risks with minimal side effects from treatment. Identification and reduction of exposure to risk factors are important in the treatment and prevention of COPD. Appropriate pharmacologic therapy can reduce symptoms and exacerbations, and improve health status and exercise tolerance. To date, none of the existing medications for COPD has been shown to modify disease progression or reduce mortality. The classes of medication are bronchodilators including beta2-agonist, anticholinergics and anti-inflammatory drug including inhaled corticosteroid and phosphodiesterase-4 inhibitor such as roflumilast. Each treatment regimen needs to be individualized as the relationship between severity of symptoms, airflow limitation and severity of exacerbation can differ between patients.
Key Words: Pulmonary disease, chronic obstructive; Beta2-agonist; Cholinergic antagonists; Inhaled corticosteroid; Phosphodiesterase 4 inhibitors
기관지 확장제
기관지 확장제는 COPD 치료의 중심이며 효과 및 부작용
등을 고려할 때, 흡입약제를 우선 사용하고 지속적인 증상이
있는 경우에는 속효성보다는 지속성 기관지확장제 사용을
권장한다. 작용시간에 따라 속효성과 지속성으로 구분하며,
증상 발생을 예방하거나 줄이기 위해 필요 시 혹은 규칙적
으로 사용한다. 흡입속효성기관지확장제의 효과는 대개 4-
6시간 지속된다. 흡입지속성베타-2작용제와 흡입지속성항
콜린제는 약제에 따라 12시간 또는 24시간 이상 약효가 지
속된다(Table 1). 흡입약물을 사용하는 경우 약물이 효과적
으로 폐와 기도에 전달되도록 사용방법에 대한 교육이 반
드시 필요하다[4,5]. 정량흡입기를 사용하기 힘든 경우에는
흡입보조기(스페이서, spacer)가 도움이 될 수 있다. 네불라
이저는 가격이 비싸고 적절한 유지관리가 필요하기 때문에
안정 시 치료에는 추천하지 않는다.
1. 베타-2작용제
베타-2교감신경 수용체를 자극하여 cyclic AMP (cAMP)
를 증가시키고 기도평활근 수축을 억제한다. 흡입속효성베
타-2작용제는 1초간 강제호기량(forced expiratory volume
in one second, FEV
1)의 호전과 증상을 개선시킬 수 있어
증상조절을 위해 필요 시 사용할 수 있
다. Indacaterol은 효과가 24시간 이상
지속되어 하루 한번 사용하며, 국내에
서 유용한 흡입지속성베타-2작용제다.
Indacaterol 150 μg/day와 300 μg/day
는 formoterol, salmeterol보다 폐기능
을 더 호전시켰다[6,7]. 또한 위약에 비
해 호흡곤란 정도, 삶의 질, 운동능력
을 개선시키고 악화의 빈도를 줄였다
[8-10]. 국내 시판 후 감시보고에서 안
정성과 효능에 대해 보고하였다[11]. 보
험기준은 FEV
1정상예측치의 80% 미만
COPD에서 인정된다.
2. 항콜린제
항콜린제는 기도 평활근의 M3 무스카린성
수용체(mus-carinic receptor)에 대한 아세틸콜린의 기관지 수축 효과
를 차단한다. Tiotropium, aclidinium, glycopyrronium
bromide 및 umeclidinium과 같은 흡입지속성항콜린제는
M3 무스카린성 수용체에 대한 결합 연장 및 M2 무스카린
성 수용체와의 빠른 해리를 통해 기관지 확장제의 효과 지
속시간을 연장시킨다. 국내에 유용한 흡입지속성항콜린제
중 tiotropium과 umeclidinium은 하루에 1회 투여하고,
aclidinium은 하루에 2회 투여한다. 흡입지속성항콜린제 요
법은 증상, 삶의 질과 호흡재활 효과를 향상시키고, 급성악
화 및 급성악화 관련 입원을 줄여준다[12-14]. 임상시험 결
과 흡입지속성항콜린제(tiotropium) 요법이 흡입지속성베
타-2작용제 요법에 비해 급성악화를 감소시킨다[15]. 보험
기준은 FEV
1정상예측치의 80% 미만 COPD에서 인정된다.
3. 기관지확장제 병합요법
서로 다른 작용기전을 가진 기관지확장제를 병용하면, 단
일 기관지확장제의 용량을 증가시켜 사용하는 것보다 부작
용의 위험은 줄이면서 기관지 확장 효과는 상승시킬 수 있
다.흡입지속성베타-2작용제와 흡입지속성항콜린제가 하나
의 흡입기로 개발되어 여러 약제가 사용되고 있다. 흡입지속
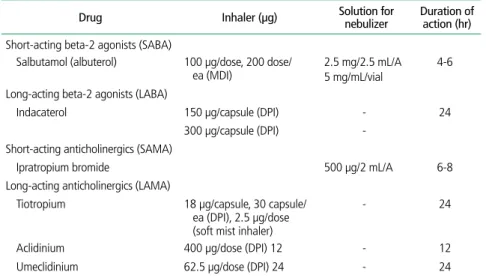
Table 1. Available inhaled bronchodilators in Korea (2018)
Drug Inhaler (μg) Solution for nebulizer Duration of action (hr) Short-acting beta-2 agonists (SABA)
Salbutamol (albuterol) 100 μg/dose, 200 dose/
ea (MDI) 2.5 mg/2.5 mL/A 5 mg/mL/vial 4-6 Long-acting beta-2 agonists (LABA)
Indacaterol 150 μg/capsule (DPI) - 24 300 μg/capsule (DPI)
-Short-acting anticholinergics (SAMA)
Ipratropium bromide 500 μg/2 mL/A 6-8 Long-acting anticholinergics (LAMA)
Tiotropium 18 μg/capsule, 30 capsule/ ea (DPI), 2.5 μg/dose
(soft mist inhaler)
- 24
Aclidinium 400 μg/dose (DPI) 12 - 12 Umeclidinium 62.5 μg/dose (DPI) 24 - 24 SABA, short acting bronchodilator; LABA, long acting bronchodilator; SAMA, short acting muscarinic antagonist; LAMA, long acting muscarinic antagonist; MDI, metered dose inhaler; DPI, dry powder inhaler.
성기관지확장제 병합요법은 위약보다 폐기능을 증가시키며,
단일 흡입지속성기관지확장제 사용과 비교에서 우월한 폐
기능 상승효과를 나타낸다[16-18]. 흡입지속성기관지확장
제 병합요법은 위약이나 단일 흡입지속성기관지확장제보다
호흡곤란 개선, 삶의 질 개선과 급성악화의 빈도를 감소시켰
다[19-21]. 급성악화의 과거력이 있는 환자들을 대상으로
한 연구에서 흡입지속성기관지확장제 병합요법은 흡입스테
로이드와 흡입지속성베타2-작용제 복합요법에 비해 급성악
화를 감소시켰다[21]. 보험기준은 FEV
1정상예측치의 80%
미만 COPD에서 인정된다.
흡입스테로이드와 지속기관지확장제의
병합요법
COPD의 국소 혹은 전신 염증에 대한 흡입스테로이드 단
독사용의 효과에 대해서는 증거가 부족한 실정이며 폐렴의
발생을 증가시켜 흡입스테로이드 단독치료는 권고하지 않는
다. 흡입스테로이드와 흡입지속성베타-2작용제 병합요법은
대규모 전향적 연구에서 사망률을 의미 있게 감소시키지는
못했다[22,23]. 최근 연구에서 흡입스테로이드, 흡입지속성
베타-2작용제, 흡입지속성항콜린제 삼제 병합요법이 흡입
항콜린제 단독요법, 흡입스테로이드와 흡입지속성베타-2작
용제 병합요법, 흡입지속성베타-2작용
제와 흡입지속성항콜린제 병합요법보다
폐기능과 삶의 질을 향상키시고, 급성악
화를 감소시켰다[24-28]. 흡입스테로이
드를 포함한 병합요법은 천식을 동반한
중복 증후군, 혈중 호산구 증가증과 잦
은 악화 환자 등 특수한 임상상황에 한정
되어야 한다. 국내 보험기준은 부분 조
절 이상 단계의 천식과 FEV
1정상예측
치의 60% 미만 COPD에 보험이 적용된
다(Table 2).
Phosphodiesterase-4억제제
Phosphodiesterase-4억제제는 cAMP의 대사를 방해하여
세포내 cAMP 농도를 높이는데 이는 항염증효과를 나타내고
또한 호중구의 이동과 화학 주성을 억제하는 효과도 있다.
Roflumilast는 처음으로 COPD 치료제로 허가 받은 약물로
하루 한번 복용하는 경구용 약제로 기관지 확장제가 아니지
만 FEV
1과 삶의 질 향상효과가 있다[29-31]. 가장 흔한 부
작용은 설사와 구역 증상이고 대부분 약물치료의 초기에 발
생한다[32]. 체중감소는 평균 2 kg 정도이고 비만 환자(체질
량지수 >30)에서 체중감소를 더 많이 볼 수 있으며 체중변
화는 초기 6개월 이내에 발생한다. 대부분 약물 중단 3개월
이내에 체중이 회복된다. 국내 보험기준은 급성악화 병력이
있고 만성기관지염을 수반한 중증의 COPD (FEV
1정상 예
측치의 50% 미만의 경우 또는 흡입지속성베타-2작용제나
흡입지속성항콜린제 등의 지속 투여에도 연 2회 이상 급성
악화가 발생한 경우)에는 투여소견서를 참조하여 인정한다.
기타 약물적 치료
1. 예방접종
모든 COPD 환자에게 인플루엔자 백신 접종을 권장한다.
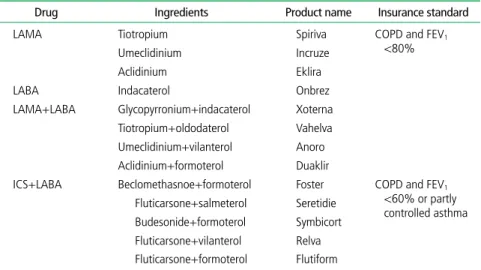
Table 2. Insurance standard of inhaled bronchodilators and inhaled steroids in Korea
Drug Ingredients Product name Insurance standard LAMA Tiotropium Spiriva COPD and FEV1
<80% Umeclidinium Incruze
Aclidinium Eklira LABA Indacaterol Onbrez LAMA+LABA Glycopyrronium+indacaterol Xoterna
Tiotropium+oldodaterol Vahelva Umeclidinium+vilanterol Anoro Aclidinium+formoterol Duaklir
ICS+LABA Beclomethasnoe+formoterol Foster COPD and FEV1
<60% or partly controlled asthma Fluticarsone+salmeterol Seretidie Budesonide+formoterol Symbicort Fluticarsone+vilanterol Relva Fluticarsone+formoterol Flutiform
LAMA, long acting muscarinic antagonist; LABA, long acting bronchodilator; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in one second.
COPD 환자에서 인플루엔자 백신은 입원이 필요한 하기도
감염과 사망을 감소시키며 고령의 환자에서 더 효과적이다
[33-35]. 65세 이상의 모든 COPD 환자에게 폐렴구균 백
신 접종을 권장한다. 23가 폐렴구균 다당질백신(PPSV23)
은 FEV
140% 미만 혹은 동반질환(특히 심장질환)들을 지닌
65세 미만 COPD 환자들의 지역사회획득 폐렴 발생을 감소
시킨다. 폐렴구균 단백결합 백신(PCV 13)은 접종 후 2년까
지 PPSV23보다 동등하거나 우월한 면역성을 보인다. 한 연
구에서 PCV 13은 65세 이상의 성인에서 백신형 지역사회획
득 폐렴과 침습성 폐렴구균질환의 예방
에 유의한 효과가 있었으며, 이 효과는
최소 4년 이상 지속되었다[36].
2. 항생제
1년 동안 azithromycin (250 mg/day
혹은 500 mg 주 3회) 혹은 erythromycin
(500 mg 1일 2회)을 COPD 급성악화의
경향을 보이는 환자에게 투여했을 때 급
성악화의 위험을 줄였다[37-39]. 그러
나 azithromycin 투여는 항생제 내성
과 청력이상 빈도를 증가시킨다. 현재
COPD 급성악화를 예방하기 위한 항생
제 지속투여의 효과 혹은 안정성에 대한
1년 이상의 연구결과는 없기 때문에 안
정 시 COPD 환자에게 예방적 항생제 처
방을 권장하지 않는다.
3. 점액용해제와 항산화제
점액용해제인 N-acetylcysteine이나
carbocysteine과 같은 약제는 항산화 효과
를 가지며, 흡입 스테로이드제제를 사용
하지 않는 환자에서 급성 악화를 감소시
키고 건강상태를 조금 호전시켰다[40].
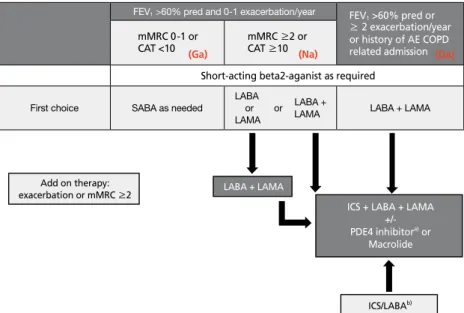
국내 각 군 환자별 약물치료
국내 COPD 종합적 평가 (Figure 1)와 각 군 환자별 약물치
료는 다음과 같다. (Figure 2)
1. 가군 환자
FEV
1이 정상예측치의 60% 이상이고, 지난 1년 동안 급
성악화가 1회 이하이면서 modified Medical Research
Council (mMRC) 0-1단계 사이의 호흡곤란이나 COPD
Assessment Test (CAT) 10점 미만의 경미한 증상이 있는
(Da) (Ga) (Na) FEV1 < 60% Exacerbation frequency ≥2/year or one hospitalization due to exacerbation Exacerbation frequency of 0-1/year FEV1 ≥60% mMRC 0-1 CAT <10
Symptoms (mMRC or CAT score)
mMRC ≥2 CAT ≥10
Figure 1. Classification of patients with chronic obstructive pulmonary disease. FEV1, forced expiratory
vol-ume in 1 second; mMRC, modified Medical Research Council dyspnea score; CAT, COPD Assessment Test score.
FEV1 >60% pred or
≥ 2 exacerbation/year or history of AE COPD related admission (Da)
mMRC 0-1 or
CAT <10 (Ga) mMRC ≥2 or CAT ≥10 (Na)
Short-acting beta2-aganist as required
First choice SABA as needed
LABA LABA + or or LAMA LAMA
LABA + LAMA
Figure 2. Pharmacologic treatment algorithms. FEV1, forced expiratory volume in one second; mMRC,
mod-ified Medical Research Council dyspnea score; CAT, COPD Assessment Test score; AE COPD, acute exacerba-tion of chronic obstructive pulmonary disease; SABA, short acting bronchodilator; LABA, long acting broncho-dilator; LAMA, long acting muscarinic antagonist; ICS, inhaled corticosteroid; PDE4, phosphodiesterase-4. a)
Postbronchodilator FEV1 <50%, symptoms of chronic bronchitis, and a history of exacerbations. b)Asthma
overlap or high blood eosinophil.
LABA + LAMA
ICS + LABA + LAMA +/- PDE4 inhibitora) or Macrolide Add on therapy: exacerbation or mMRC ≥2 ICS/LABAb)
환자를 말한다. 흡입속효성기관지확장제의 경우 폐기능을
호전시키고 호흡곤란을 감소시키는 효과가 있어 일차 치료
로 권장한다. 약물치료에도 불구하고 mMRC 2단계 이상의
증상이 발생하거나 급성악화가 발생하는 경우 흡입지속성기
관지확장제를 사용할 수 있다.
2. 나군 환자
FEV
1이 정상예측치의 60% 이상이고 지난 1년 동안 급성
악화가 1회 이하이면서 mMRC 2단계 이상의 호흡곤란이나
CAT 10점 이상의 증상이 있는 환자를 말한다. 흡입지속성
베타-2작용제 혹은 흡입지속성항콜린제를 일차 약제로 사
용할 수 있으며 두 약물 간 우열은 없고 진료의사 및 환자의
선호에 따라 선택할 수 있다. 진단 당시 증상이 심한 경우 처
음부터 흡입지속성베타-2작용제와 흡입지속성항콜린제를
병합하여 사용할 수 있다.
3. 다군 환자
mMRC 혹은 CAT 점수와 상관없이 FEV
1이 정상 예측치
의 60% 미만이거나 지난 1년 동안 2회 이상 급성악화가 있
었거나 입원할 정도로 심한 악화가 있었던 환자를 말한다.
흡입지속성베타-2작용제와 흡입지속성항콜린제 복합제의
사용을 일차치료로 권장한다. 다만 천식과 중복되어 있거
나 혈중 호산구가 높은 환자에서는 inhaled corticosteroid/
long acting muscarinic antagonist (LABA) 복합제를 일차
약제로 고려해 볼 수 있다.
다군 환자에서 흡입지속성베타-2작용제와 흡입지속성항
콜린제 복합제 또는 ICS/LABA 복합제의 사용에도 불구하
고 mMRC 2단계 이상의 증상이 지속되거나 급성악화가 발
생하는 경우 세가지 약제 성분을 모두 병합하여 사용하도
록 한다.
Phosphodiesterase-4 억제제는 급성악화 병력이 있고 만
성기관지염을 수반한 중증의 COPD 즉 FEV
1값이 정상 예측
치의 50% 미만의 경우 또는 흡입지속성베타-2작용제나 흡
입지속성항콜린제 등의 지속 투여에도 연 2회 이상 급성악화
가 발생한 경우에 사용할 수 있다. Macrolide 추가 요법은 악
화를 유의하게 감소시키는 효과를 보였다. 장기 사용 시 내성
균 발현, 청력저하 등의 부작용 우려가 있으므로 사용 시 신
중을 기해야 한다.
결론
최근 다양한 COPD 약제가 개발되어 많은 임상결과에 따
른 치료 가이드라인이 변화가 있다. COPD의 조기 발견과
적절한 약물치료를 통해 증상완화, 운동능력 향상, 삶의 질
향상과 급성악화 감소, 질병진행을 예방할 수 있다. 또한
COPD 환자의 적절한 평가와 각 군에 따른 가이드라인의 권
고 약제를 사용하는 것이 중요하다.
찾아보기말:
만성폐쇄성폐질환; 베타-2작용제; 항콜린제; 흡입스테로이드; PDE4 억제제ORCID
In Ae Kim, https://orcid.org/0000-0002-8994-2891 Yong Bum Park, https://orcid.org/0000-0002-5814-6104 Kwang Ha Yoo, https://orcid.org/0000-0001-9969-2657REFERENCES
1. Burge PS, Calverley PM, Jones PW, Spencer S, Anderson JA, Maslen TK. Randomised, double blind, placebo controlled study of fluticasone propionate in patients with moderate to severe chronic obstructive pulmonary disease: the ISOLDE trial. BMJ 2000;320:1297-1303.
2. Anthonisen NR, Connett JE, Kiley JP, Altose MD, Bailey WC, Buist AS, Conway WA Jr, Enright PL, Kanner RE, O’Hara P, Owens GR, Scanlon PD, Tashkin DP, Wise RA, Altose MD, Connors AF, Redline S, Deitz C, Rakos RF, Conway WA Jr, DeHorn A, Ward JC, Hoppe-Ryan CS, Jentons RL, Reddick JA, Sawicki C, Wise RA, Permutt S, Rand CS, Scanlon PD, Davis LJ, Hurt RD, Miller RD, Williams DE, Caron GM, Lauger GG, Toogood SM, Buist AS, Bjornson WM, Johnson LR, Bailey WC, Brooks CM, Dolce JJ, Higgins DM, Johnson MA, Lorish CD, Martin BA, Tashkin DP, Coulson AH, Gong H, Harber PI, Li VC, Roth M, Nides MA, Simmons MS, Zuniga I, Anthonisen NR, Manfreda J, Murray RP, Rempel-Rossum SC, Stoyko JM, Connett JE, Kjelsberg MO, Cowles MK, Durkin DA, Enright PL, Kurnow KJ, Lee WW, Lindgren PG, Mongin SJ, O’Hara P, Voelker HT, Waller LA, Owens
GR, Rogers RM, Johnston JJ, Pope FP, Vitale FM, Kanner RE, Rigdon MA, Benton KC, Grant PM, Becklake M, Burrows B, Cleary P, Kimbel P, Nett L, Ockene JK, Senior RM, Snider GL, Spitzer W, Williams OD, Hurd SS, Kiley JP, Wu MC, Ayres SM, Hyatt RE, Mason BA. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1: the Lung Health Study. JAMA 1994;272:1497-1505.
3. Park YB, Rhee CK, Yoon HK, Oh YM, Lim SY, Lee JH, Yoo KH, Ahn JH; Committee of the Korean COPD Guideline 2018. Revised (2018) COPD Clinical Practice Guideline of the Korean Academy of tuberculosis and respiratory disease: a summary. Tuberc Respir Dis (Seoul) 2018 Jun 19 [Epub]. https://doi.org/10.4046/trd.2018.0029.
4. Bosnic-Anticevich SZ. Continued innovation in respiratory care: the importance of inhaler devices. Tuberc Respir Dis (Seoul) 2018;81:91-98.
5. Yoo KH, Chung WY, Park JH, Hwang SC, Kim TE, Oh MJ, Kang DR, Rhee CK, Yoon HK, Kim TH, Kim DK, Park YB, Kim SH, Yum HK. Short-term evaluation of a comprehensive education program including inhaler training and disease management on chronic obstructive pulmonary disease. Tuberc Respir Dis (Seoul) 2017;80:377-384.
6. Korn S, Kerwin E, Atis S, Amos C, Owen R, Lassen C; INSIST study group. Indacaterol once-daily provides superior efficacy to salmeterol twice-daily in COPD: a 12-week study. Respir Med 2011;105:719-726.
7. Donohue JF, Betts KA, Du EX, Altman P, Goyal P, Keininger DL, Gruenberger JB, Signorovitch JE. Comparative efficacy of long-acting β2-agonists as monotherapy for chronic obstruc-tive pulmonary disease: a network meta-analysis. Int J Chron Obstruct Pulmon Dis 2017;12:367-381.
8. Beeh KM, Wagner F, Khindri S, Drollmann AF. Effect of indacaterol on dynamic lung hyperinflation and breathless-ness in hyperinflated patients with COPD. COPD 2011;8:340-345.
9. O’Donnell DE, Casaburi R, Vincken W, Puente-Maestu L, Swales J, Lawrence D, Kramer B; INABLE 1 study group. Effect of indacaterol on exercise endurance and lung hyper-inflation in COPD. Respir Med 2011;105:1030-1036. 10. Wang J, Nie B, Xiong W, Xu Y. Effect of long-acting
beta-agonists on the frequency of COPD exacerbations: a meta-analysis. J Clin Pharm Ther 2012;37:204-211.
11. Yum HK, Kim HR, Chang YS, Shin KC, Kim S, Oh YM. Safety and effectiveness of indacaterol in chronic obstructive pulmonary disease patients in South Korea. Tuberc Respir Dis (Seoul) 2017;80:52-59.
12. Karner C, Chong J, Poole P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2014;(7):CD009285.
13. Casaburi R, Kukafka D, Cooper CB, Witek TJ Jr, Kesten S. Improvement in exercise tolerance with the combination of tiotropium and pulmonary rehabilitation in patients with COPD. Chest 2005;127:809-817.
14. Kesten S, Casaburi R, Kukafka D, Cooper CB. Improvement
in self-reported exercise participation with the combination of tiotropium and rehabilitative exercise training in COPD patients. Int J Chron Obstruct Pulmon Dis 2008;3:127-136. 15. Decramer ML, Chapman KR, Dahl R, Frith P, Devouassoux
G, Fritscher C, Cameron R, Shoaib M, Lawrence D, Young D, McBryan D; INVIGORATE investigators. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomised, blinded, parallel-group study. Lancet Respir Med 2013;1:524-533.
16. Cazzola M, Molimard M. The scientific rationale for combin-ing long-actcombin-ing beta2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther 2010;23:257-267.
17. Farne HA, Cates CJ. Long-acting beta2-agonist in addition to tiotropium versus either tiotropium or long-acting beta2-agonist alone for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2015;(10):CD008989.
18. Oba Y, Sarva ST, Dias S. Efficacy and safety of long-acting β-agonist/long-acting muscarinic antagonist combinations in COPD: a network meta-analysis. Thorax 2016;71:15-25. 19. Miravitlles M, Baek S, Vithlani V, Lad R. Optimal
bronchodi-lation for COPD patients: are all long-acting β₂-agonist/long-acting muscarinic antagonists the same? Tuberc Respir Dis (Seoul) 2018;81:198-215.
20. Wedzicha JA, Decramer M, Ficker JH, Niewoehner DE, Sandström T, Taylor AF, D’Andrea P, Arrasate C, Chen H, Banerji D. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med 2013;1:199-209.
21. Wedzicha JA, Banerji D, Chapman KR, Vestbo J, Roche N, Ayers RT, Thach C, Fogel R, Patalano F, Vogelmeier CF; FLAME Investigators. Indacaterol-glycopyrronium versus salmeterol-fluticasone for COPD. N Engl J Med 2016;374: 2222-2234.
22. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, Yates JC, Vestbo J; TORCH investigators. Sal-meterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007;356:775-789.
23. Vestbo J, Anderson JA, Brook RD, Calverley PM, Celli BR, Crim C, Martinez F, Yates J, Newby DE; SUMMIT Investi-gators. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened car-diovascular risk (SUMMIT): a double-blind randomised con-trolled trial. Lancet 2016;387:1817-1826.
24. Vestbo J, Papi A, Corradi M, Blazhko V, Montagna I, Fran-cisco C, Cohuet G, Vezzoli S, Scuri M, Singh D. Single inhaler extrafine triple therapy versus long-acting muscarinic anta-gonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised con-trolled trial. Lancet 2017;389:1919-1929.
25. Singh D, Papi A, Corradi M, Pavlisova I, Montagna I, Francisco C, Cohuet G, Vezzoli S, Scuri M, Vestbo J. Single inhaler triple therapy versus inhaled corticosteroid plus
long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, random-ised controlled trial. Lancet 2016;388:963-973.
26. Lipson DA, Barnacle H, Birk R, Brealey N, Locantore N, Lomas DA, Ludwig-Sengpiel A, Mohindra R, Tabberer M, Zhu CQ, Pascoe SJ. FULFIL trial: once-daily triple therapy for patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2017;196:438-446.
27. Papi A, Vestbo J, Fabbri L, Corradi M, Prunier H, Cohuet G, Guasconi A, Montagna I, Vezzoli S, Petruzzelli S, Scuri M, Roche N, Singh D. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary dis-ease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet 2018;391:1076-1084.
28. Lipson DA, Barnhart F, Brealey N, Brooks J, Criner GJ, Day NC, Dransfield MT, Halpin DMG, Han MK, Jones CE, Kilbride S, Lange P, Lomas DA, Martinez FJ, Singh D, Tabberer M, Wise RA, Pascoe SJ; IMPACT Investigators. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med 2018;378:1671-1680.
29. Calverley PM, Rabe KF, Goehring UM, Kristiansen S, Fabbri LM, Martinez FJ; M2-124 and M2-125 study groups. Roflumilast in symptomatic chronic obstructive pulmonary disease: two randomised clinical trials. Lancet 2009;374:685-694.
30. Calverley PM, Sanchez-Toril F, McIvor A, Teichmann P, Bredenbroeker D, Fabbri LM. Effect of 1-year treatment with roflumilast in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2007;176:154-161.
31. Fabbri LM, Calverley PM, Izquierdo-Alonso JL, Bundschuh DS, Brose M, Martinez FJ, Rabe KF; M2-127 and M2-128 study groups. Roflumilast in moderate-to-severe chronic ob- structive pulmonary disease treated with longacting broncho-dilators: two randomised clinical trials. Lancet 2009;374:695-703.
32. Joo H, Han D, Lee JH, Rhee CK. Incidence of adverse effects and discontinuation rate between patients receiving 250 micrograms and 500 micrograms of roflumilast: a com-parative study. Tuberc Respir Dis (Seoul) 2018 Jun 19 [Epub]. https://doi.org/10.4046/trd.2018.0015.
33. Restrepo MI, Sibila O, Anzueto A. Pneumonia in patients with chronic obstructive pulmonary disease. Tuberc Respir Dis (Seoul) 2018;81:187-197.
34. Poole PJ, Chacko E, Wood-Baker RW, Cates CJ. Influenza vaccine for patients with chronic obstructive pulmonary dis-ease. Cochrane Database Syst Rev 2006;(1):CD002733. 35. Hak E, van Essen GA, Buskens E, Stalman W, de Melker RA.
Is immunising all patients with chronic lung disease in the community against influenza cost effective? Evidence from a general practice based clinical prospective cohort study in
Utrecht, The Netherlands. J Epidemiol Community Health 1998;52:120-125.
36. Bonten MJ, Huijts SM, Bolkenbaas M, Webber C, Patterson S, Gault S, van Werkhoven CH, van Deursen AM, Sanders EA, Verheij TJ, Patton M, McDonough A, Moradoghli-Haftvani A, Smith H, Mellelieu T, Pride MW, Crowther G, Schmoele-Thoma B, Scott DA, Jansen KU, Lobatto R, Oosterman B, Visser N, Caspers E, Smorenburg A, Emini EA, Gruber WC, Grobbee DE. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med 2015;372: 1114-1125.
37. Seemungal TA, Wilkinson TM, Hurst JR, Perera WR, Saps-ford RJ, Wedzicha JA. Long-term erythromycin therapy is associated with decreased chronic obstructive pulmonary disease exacerbations. Am J Respir Crit Care Med 2008;178: 1139-1147.
38. Albert RK, Connett J, Bailey WC, Casaburi R, Cooper JA Jr, Criner GJ, Curtis JL, Dransfield MT, Han MK, Lazarus SC, Make B, Marchetti N, Martinez FJ, Madinger NE, McEvoy C, Niewoehner DE, Porsasz J, Price CS, Reilly J, Scanlon PD, Sciurba FC, Scharf SM, Washko GR, Woodruff PG, Anthonisen NR; COPD Clinical Research Network. Azithro-mycin for prevention of exacerbations of COPD. N Engl J Med 2011;365:689-698.
39. Uzun S, Djamin RS, Kluytmans JA, Mulder PG, van’t Veer NE, Ermens AA, Pelle AJ, Hoogsteden HC, Aerts JG, van der Eerden MM. Azithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): a randomised, double-blind, placebo-controlled trial. Lancet Respir Med 2014;2:361-368.
40. Poole P, Chong J, Cates CJ. Mucolytic agents versus placebo for chronic bronchitis or chronic obstructive pulmonary dis-ease. Cochrane Database Syst Rev 2015;(7):CD001287.
Peer Reviewers’ Commentary
이 논문은 2018년에 개정된 만성폐쇄성폐질환(COPD) 진료지침 을 바탕으로, 국내에서 유용한 치료 약물에 대한 내용을 소개하 고 있다. 실제 임상에서 적용할 수 있는 약제들의 기전, 효과 및 부작용과 각 약제들의 국내 보험 기준에 대한 내용을 체계적으 로 설명해 주고 있다. 우리나라 자체의 가이드라인에서 제시하 고 있는 COPD 환자들의 종합 평가에 따른 환자별 약물 치료에 대하여 체계적으로 설명하고 있어, 우리나라 CP{D 환자의 적절 한 평가 및 약제의 사용을 위한 좋은 지침이 될 것으로 판단된다. [정리: 편집위원회]