INTRODUCTION
Free or pedicled vascularized fibular grafts (VFG) are useful for the reconstruction of large skeletal defects, particularly in cases of scarred or avascular beds, or in patients with combined bone and soft tissue defects. Compared to non-VGF, VGF maintain their own viability, and serve as good osteoconductive and osteoinductive grafts because they contain living osteocytes and osteoblasts.
Due to its many structural and biological advantages, the free fibular osteo- or osteocutaneous graft is considered the most suitable autograft for the reconstruction of long bone defects in the extremities. The main surgical indication for a free VGF is the reconstruction of bone and soft tissue for a defect that is longer than 6 cm. Recently, the indications have been widely expanded to include not only the treatment of defects of the mid-tibia, humerus, forearm, distal femur, and proximal tibia;
but also arthrodesis of the shoulder and knee joints. Because
Updated Surgical Techniques and Expanded Indications of Free Vascularized Fibular Graft
Jong Woong Park
Department of Orthopedic Surgery, Division of Hand Surgery and Reconstructive Microsurgery, Korea University Anam Hospital, Seoul, Korea
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2015 by the Korean Society for Microsurgery. All Rights Reserved.
Received November 2, 2015 Accepted November 19, 2015
*Correspondence to: Jong Woong Park Department of Orthopedic Surgery, Division of Hand Surgery and Reconstructive Microsurgery, Korea University Anam Hospital, 73 Inchon-ro, Seongbuk-gu, Seoul 02841, Korea Tel: +82-2-920-5320
Fax: +82-2-920-5320 E-mail: [email protected] Financial support: None.
Conflict of interest: None.
Free or pedicled vascularized fibular grafts (VFG) are useful for the reconstruction of large skeletal defects, particularly in cases of scarred or avascular beds, or in patients with combined bone and soft tissue defects. Compared to non-VFG, VEG, which contains living osteocytes and osteoblasts, maintains its own viability and serves as good osteoconductive and osteoinductive graft. Due to its many structural and biological advantages, the free fibular osteo- or osteocutaneous graft is considered the most suitable autograft for the reconstruction of long bone defects in the injured extremity. The traditional indication of VFG is the long bone and soft tissue defect, which cannot be reconstructed using a conventional operative method. Recently, the indications have been widely expanded not only for defects of midtibia, humerus, forearm, distal femur, and proximal tibia, but also for the arthrodesis of shoulder and knee joints. Because of its potential to allow further bone growth, free fibular epiphyseal transfer can be used for the hip or for distal radius defects caused by the radical resection of a tumor. The basic anatomy and surgical techniques for harvesting the VFG are well known; however, the condition of the recipient site is different in each case. Therefore, careful preoperative surgical planning should be customized in every patient. In this review, recently expanded surgical indications of VFG and surgical tips based on the author’s experiences in the issues of fixation method, one or two staged reconstruction, size mismatching, overcoming the stress fracture, and arthrodesis of shoulder and knee joint using VFG are discussed with the review of literature.
Key Words: Bone defect, Soft tissue defect, Reconstruction, Free vascularized fibular graft
ARMS
Archieves of Reconstructive Microsurgery http://dx.doi.org/10.15596/ARMS.2015.24.2.41of its potential to allow further bone growth, free fibular epiphyseal transfer can be used for the hip, or for distal radius defects caused by the radical resection of a tumor. Furthermore, successful limb reconstructions were reported through joint arthrodesis using VFG. Shoulder or knee joint arthrodesis with VFG could be a good reconstruction strategy after infected arthroplasty or destruction of the joint, which cannot be effectively reconstructed with other surgical options.
The basic anatomy and surgical techniques for harvesting the VFG are well known; however, the condition of the recipient site is very different in each case. Therefore, careful preoperative surgical planning should be customized for every patient. In this review, the recently updated indications for VFG and surgical tips based on the author’s experiences in unusual cases are discussed with a review of the literature.
RECENT UPDATES IN FIXATION METHODS FOR VASCULARIZED FIBULAR GRAFTS
Traditionally, fixation of VFG was achieved with minimal
fixation with one or two K-wires or screws for the VFG docking sites. Additional stability was obtained with mono or ring type external fixators. Stabilization of the VFG by external fixation decreases the risk of recurrent infection and provides more space for the vascular anastomosis. However, the external fixator should be maintained until graft union is achieved, which usually takes several months. During that period, it is very inconvenient for the daily life of patients and carries a high risk of pin tract infection (Fig. 1).
The recently introduced locking plate systems can be a good substitution to overcome the disadvantages of external fixators.
As this is a biological internal fixator system, the locking plate does not compress the VFG, preserving the periosteal circulation. Furthermore, with its shorter lever arm from the graft compared to the external fixator, improved stability can be achieved, which permits earlier weight bearing. In our practice, the locking plate fixation with VFG not only provides convenience to the patients, but also achieves a good clinical result in treating infected nonunion or tumor resection of the long bone. In the case of osteomyelitis, active infection should
A B
C D
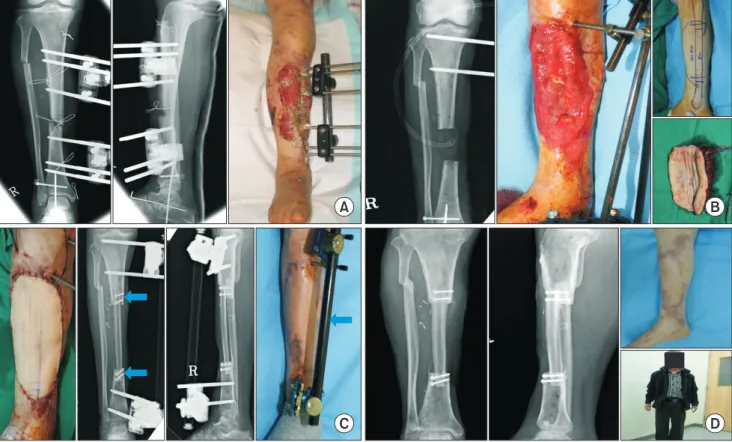
Fig. 1. Traditional free vascularized fibular graft (VFG) with minimal internal fixation. (A) Infected nonunion of tibia with soft tissue defect in 56-year- old man. (B) 18 cm VFG with 10×19 cm cutaneous flap is harvested. (C) Two screws (arrows) are fixed at proximal and distal graft sites and an external fixator is applied. (D) Two years later after operation. X-ray shows complete union and hypertrophy of VFG.
be eradicated through wide and repeated debridement with appropriate antibiotic treatment to minimize the possible recurrence of infection, prior to the application of locking plate (Fig. 2).
OVERCOMING STRESS FRACTURES
Stress fracture of the VFG after VFG union is the most
common complication in the literature, with reported rates ranging between 7.7% and 22.2%.1,2 In the majority of cases, this complication occurs within the first postoperative year.
Most stress fractures occur within the midshaft of the graft in lower extremity reconstruction cases due to the result of excessive loading. If the fracture site is well vascularized, proper immobilization induces sufficient callus formation and adequate union and hypertrophy can be obtained.
A B
C D
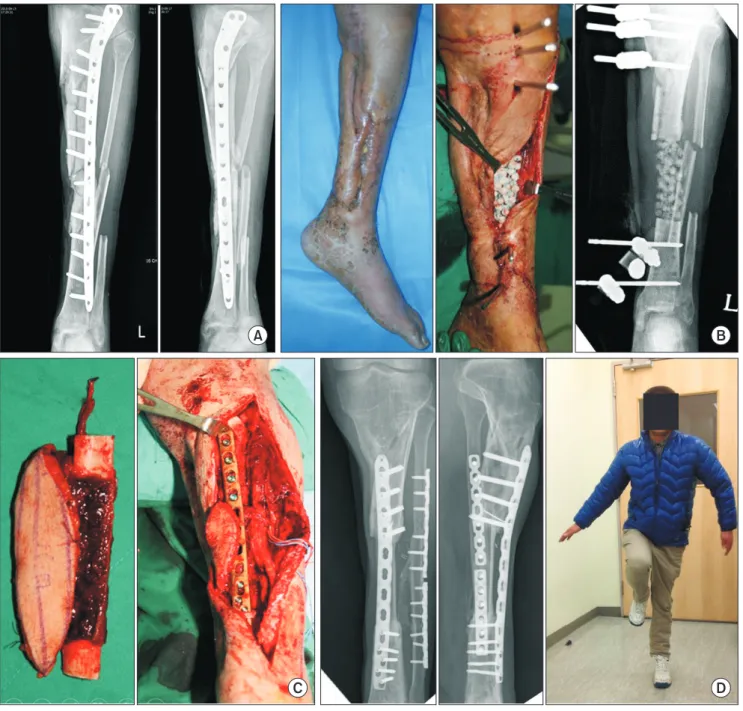
Fig. 2. Bridging locking plate fixation for vascularized fibular graft (VFG). (A) Chronic osteomyelitis of tibia with soft tissue defect in 38-year-old man.
(B) Complete debridement and antibiotics-mixed cement beads are filled in the defect. (C) VFG is applied with a bridging locking plate fixation. (D) Two years later after operation. X-ray shows complete union of VFG. Fractured ipsilateral fibular is also fixed and united.
To limit the incidence of stress fracture in VFG, excessive loading and movement at the graft site should be prevented.
For this purpose, the bridging locking plate fixator is a sufficient
internal protection device. The strong fixation not only protects the VFG from stress fractures, but also permits early weight bearing after union of the graft. However, there is rising concern
A B
C D
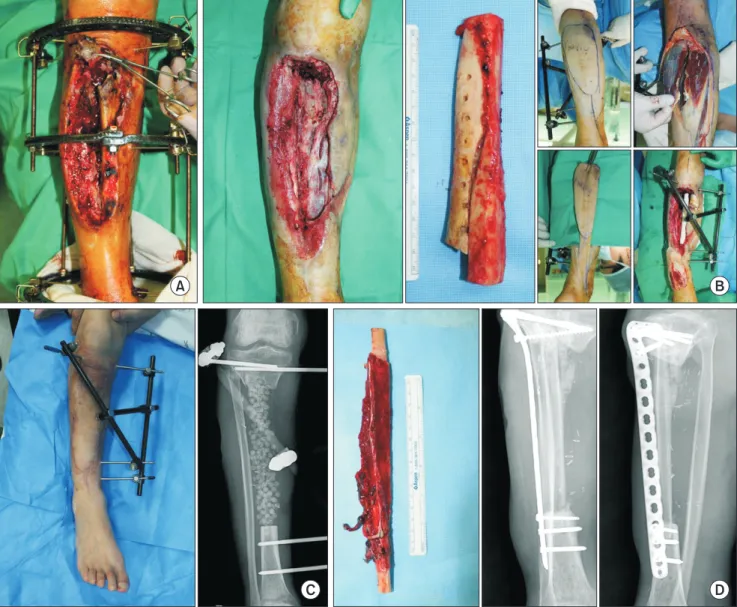
Fig. 3. Cancellous bone graft augmentation with vascularized fibular graft (VFG). (A) Chronic osteomyelitis of tibia with pathologic fracture in 55-year-old man. (B) Wide excision of sequestrum and antibiotics-mixed cement beads are filled in the defect. (C) VFG is applied with a bridging locking plate and large amount of autoiliac cancellous bone graft is added besides the VFG. (D) Three years later after operation. X-ray shows complete union of VFG and the grafted cancellous bone is completely united with VFG like a hypertrophied VFG.
about the stress shielding effect of the plate, which restricts natural graft hypertrophy and remodeling because of the limited mechanical loading. The benefits of early weight bearing must be weighed up against the need for protection of the graft from excessive loads.
Along with the VFG with the bridging locking plate fixation, the author has attempted augmentation cancellous bone grafts.
In this procedure, autogenous cancellous bone is obtained from the iliac crest and transferred to the proximal or distal junction of the VFG, where the VFG and recipient bone size mismatching is significant. Additionally, cancellous bone is grafted beside the shaft of the VFG in onlay graft fashion. After
union of the cancellous grafts with the VFG, the cross sectional load bearing area of the VFG is increased. The results of several of our cases were satisfactory, without graft absorption or stress fracture (Fig. 3). However, in the consideration of the risks of recurrent infection, pure autogenous cancellous bone graft is recommended without combination with an allograft.
When the VFG is transferred combined with its cutaneous flap, vascular perforators for the cutaneous flap should be protected from the cancellous bone mass.
Additional strategy to prevent the stress fracture of the VFG is to obtain union of the ipsilateral fibular fracture. When the fibular is fractured in the injured leg, obtaining union through
A B
C D
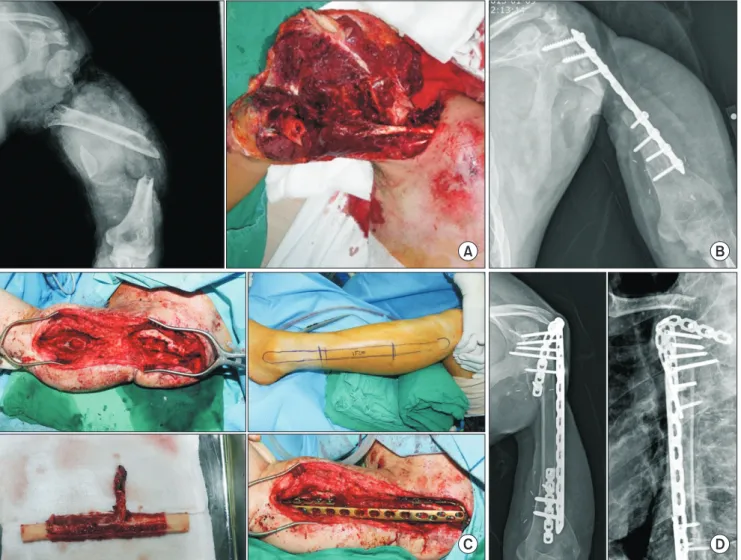
Fig. 4. Staged reconstruction for huge bone and soft tissue defect. (A) Huge soft tissue and bone defect which can’t be reconstructed by the one- stage free vascularized osteocutaneous flap in 54-year-old man. (B) Wide excision of dead bone and antibiotics-mixed cement beads are filled with an external fixation. The soft tissue defect is reconstructed with a medial gastrocnemius muscle flap and 17×9cm-sized reverse sural artery island flap. (C) Soft tissue defect is well healed. (D) A vascularized fibular graft is applied with a bridging locking plate as a second stage operation.
the open reduction and internal fixation for the ipsilateral fibular fracture can provide additional stability combined with the VFG.
STAGED RECONSTRUCTION VS.
SINGLE STAGE RECONSTRUCTION
One of the most important advantages of free VFG is that single stage reconstruction is possible with the composite osteocutaneous flap. If the recipient bed is free from active infection, bone and soft tissue defects can be reconstructed in a single stage operation. The VFG can be harvested with its cutaneous flap as large as 10×20 cm. However, in some cases, the soft tissue defect is larger than the permissible size of the fibular osteocutaneous flap, or the condition of the recipient site requires a more vascularized skin flap.
In the staged operation, a free flap or pedicled flap covers the soft tissue defect in the first stage, and the bone defect is reconstructed later. For the free flap donor site, the latissimus dorsi muscle or myocutaneous flap, or the anterolateral thigh flap can be used. However, in cases with a heavily scarred bed due to recurrent infection or failed previous free flap surgery, preserved recipient vessels are very limited, and it can be difficult to find healthy recipient vessels. In this situation, the first stage operation can be performed with various kinds of pedicled grafts around the open wound. Usually, soft tissue reconstruction with an appropriate pedicled muscle flap or an island fasciocutaneous flap can cover large soft tissue defects which cannot be covered with a fibular osteocutaneous flap.
The combination of one or two gastrocnemius muscle flaps with a saphenous neurocutaneous island flap or sural artery flap provides sufficient size for whole anteromedial and anterolateral defects of the leg. After the completion and eradication of residual infection, the bone defect is reconstructed with VFG as a second stage operation (Fig. 4).
SIZE MISMATCHING OF VASCULARIZED FIBULAR GRAFTS WITH DISTAL FEMUR
OR PROXIMAL TIBIA
Usually, VFG grafting is performed with a single strut, and 26 to 28 cm in length can be harvested. However, when the
recipient site of this graft is in the lower extremity, especially the distal femur or proximal tibia, there can be concerns in size mismatch and strength of the graft. With the single strut VFG graft, the risk of stress fracture and nonunion is markedly increased. In this situation, a double-barrel VFG or double- strut VFG graft is indicated. Through this technique, the free vascularized graft increases the volume of bone by two-fold, whilst maintaining its advantages as a living bone graft. Double- strut, free VGF can withstand a higher torque and more mechanical stress than a conventional single-strut VGF.
When the length of the defect is shorter than 13 cm, because the maximum length of a single VFG is 26 cm, the free fibular graft can be cut at its center and folded as a double barrel, maintaining its vascular pedicle. If the length of the defect is longer than this, a single VFG no longer connects the defect. In this situation, the ipsilateral VFG is transferred with its vascular pedicles and the contralateral free VFG is anastomosed with the ipsilateral VFG. With this double-strut hybrid anastomosis, the problems related to longer defects and size mismatch can be successfully resolved.
In distal femoral defects, both ends of a double-strut VFG can be impacted into the medullary canal of the femur, and a long anatomical distal femur locking plate is applied as a bridging plate technique. In the proximal tibial defect, the proximal ends of a double-strut VFG can be impacted into the fresh cancellous bed in the metaphysis of tibia; however, at the distal ends, the medullary canal of the tibia is not large enough to take both ends of the VFGs. The author’s recommendation is that one VFG is impacted into the medullary canal of the distal tibia and the other VFG is connected at the side of the tibia after performing a step-cut osteotomy at the end of the VFG.
If a locking plate of suitable length is available, the proximal and distal tibial ends are stabilized with one plate in a bridging plate fashion. If it is not, two separate plates are fixed at both the proximal and distal docking sites. In this situation, patients should be carefully monitored for stress fracture between the two plate ends.
KNEE JOINT ARTHRODESIS WITH VASCULARIZED
FIBULAR GRAFTS
The patient’s quality of life after limb-salvage surgery
is much better than with amputation for the treatment of osteosarcoma of the distal end of the femur or proximal tibia.
Various reconstructive techniques have been described for reconstruction after the resection of malignant tumors around the knee.3-5 The options for limb-salvage operations after malignant tumor resection depend upon the patient’s general condition and the characteristics of the tumor. Although customized knee joint arthroplasty or allograft could provide a mobile joint, unexpected complications such as deep wound infection, wound dehiscence, or osteomyelitis sometimes occur.
Knee joint arthrodesis can be a good surgical option, providing stable and predictable results after tumor resection or failed conventional reconstruction procedures. Knee joint arthrodesis can usually be performed with an autogenous
bone graft, but there is a high rate of nonunion, stress fracture, and failure of fixation,6 especially if it is performed after tumor resection because of the nonvascular bed around the graft.
Accumulated evidence shows that knee joint arthrodesis using a VFG after wide excision of a malignant tumor around the knee is a very reliable surgical option.6
The technical problems associated with VFG for knee joint arthrodesis are selecting the appropriate fixation method, including the plate positioning; whether to preserve the patella or not; gaining sufficient strength and length of the graft; and overcoming difficult vascular anastomoses. After malignant tumor resection, relatively large bone and soft tissue defects remain. Due to the limitation of thickness of the thin fibula, sufficient stability cannot be obtained with one piece of fibular
A B
C D
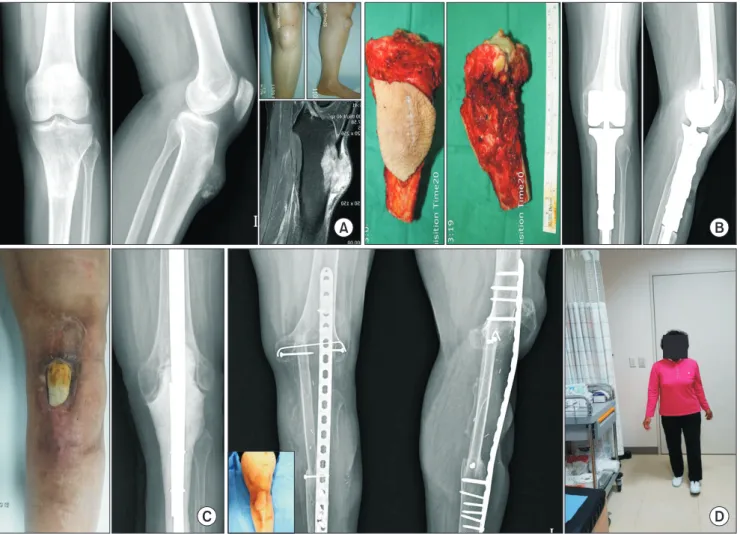
Fig. 5. Knee joint arthrodesis using a double-strut vascularized fibular graft (VFG). (A) Osteosarcoma in proximal tibia in 60-year-old woman. (B) Radical excision of tumor and the defect is reconstructed with a tumor prosthesis. (C) Two years later, the arthroplasty is infected with the soft tissue defect. The implant is removed and replaced with the cement. The soft tissue defect is covered with a sural artery island flap. (D) 18 cm bone defect is reconstructed with the ipsilateral pedicled fibular transfer and the contralateral free VFG (Double strut VFG). A year later, complete knee joint arthrodesis is obtained.
graft. To overcome this problem, a double-barrel VFG is usually needed. When the length of one VFG is not sufficient, double struts of VFG reconstruction from the ipsilateral and contralateral legs provide long and strong grafts. The free VFG obtained from the contralateral side is anastomosed with the ends of the vascular pedicles of the ipsilateral VFG.
For the fixation of VFG, a long locking plate across the joint as a bridging plate is recommended. In consideration of bone contours, positioning the plate on the anterior surface of the joint after resection of the patella is an easy way to fix the VFG.
Both ends of the VFG are fixed to the distal femur and proximal tibia with one or two screws for optimal positioning and maintaining their position. The cancellous bone chips taken from the resected patella can be grafted at the docking sites of
the grafts (Fig. 5).
SHOULDER JOINT ARTHRODESIS WITH
VASCULARIZED FIBULAR GRAFTS
Resection of malignant tumors of the proximal humerus or repeated wide debridement due to comminuted fracture, osteomyelitis, or infection following shoulder arthroplasty, often results in a large bone defect at the proximal humerus.
If the shoulder joint is destroyed with loss of the glenoid and humeral head, the ideal method for shoulder reconstruction is very limited. Shoulder arthrodesis is an appropriate salvage procedure but is associated with a high rate of complications
A B
C D
Fig. 6. Shoulder joint arthrodesis using a vascularized fibular graft (VFG). (A) Near total amputation of arm and shoulder in 42-year-old man. (B) Infected nonunion of humerus with destruction of the shoulder joint. (C) VFG is fixed with a double plating in orthogonal configuration. (D) Complete shoulder joint arthrodesis is obtained after 1 year and 9 months.
such as fixation failure, nonunion, or recurrent infection.
Shoulder arthrodesis with VFG can provide sufficient stability, and a well-vascularized graft provides strong resistance against unfavorable conditions.7 To obtain stable fixation until union, double plate fixation with orthogonal configuration is recommended for the side of the shoulder joint.8 The locking reconstruction plate is contoured to fit the scapula and the proximal VFG. The plate is applied with sufficient length from the scapular spine to the VFG. A second plate is positioned to bridge from the anterior aspect of the glenoid or acromion, to the VFG in the orthogonal position, to the first plate.8 The preferred shoulder position is 30o of abduction, 30o of flexion, and 30o to 50o of internal rotation. For distal fixation, the VFG is impacted into the medullary canal of the humerus. Reaming of the medullary canal of the humerus facilitates insertion of the fibular graft. A small locking plate can be added at the distal docking site. Vascular anastomosis is performed with the brachial artery (end-to-side) and the venae comitantes (end-to- end) with the fibular graft in a retrograde orientation to allow easier access to the vessels in the distal aspect of the arm (Fig. 6).9
CONCLUSION
In this review, the expanded indications of VFG and surgical tips based on the author’s experiences and accumulated evidences in the literature are summarized. The successful reconstruction of long bone and soft tissue defects is a very challenging mission to the orthopedic surgeon. Although various reconstruction strategies have been introduced such as bone transport with plates or external fixation, VFG still has very distinguishable and unique advantages superior to the
other surgical options.
REFERENCES
1. Ihara K, Doi K, Yamamoto M, Kawai S. Free vascularized fibular grafts for large bone defects in the extremities after tumor excision. J Reconstr Microsurg 1998;14:371-6.
2. Amr SM, El-Mofty AO, Amin SN, Morsy AM, El-Malt OM, Abdel-Aal HA. Reconstruction after resection of tumors around the knee: role of the free vascularized fibular graft. Microsurgery 2000;20:233-51.
3. Campanacci L, Alì N, Casanova JM, Kreshak J, Manfrini M.
Resurfaced allograft-prosthetic composite for proximal tibial reconstruction in children: intermediate-term results of an original technique. J Bone Joint Surg Am 2015;97:241-50.
4. Li WX, Ye ZM, Yang DS, Tao HM, Lin N, Yang ZM.
Endoprosthetic reconstruction after wide resection of primary bone tumor around the knee. Zhonghua Wai Ke Za Zhi 2007;45:
665-8.
5. Mankin HJ, Doppelt SH, Sullivan TR, Tomford WW.
Osteoarticular and intercalary allograft transplantation in the management of malignant tumors of bone. Cancer 1982;50:613- 30.
6. Enneking WF, Shirley PD. Resection-arthrodesis for malignant and potentially malignant lesions about the knee using an intramedullary rod and local bone grafts. J Bone Joint Surg Am 1977;59:223-36.
7. Scalise JJ, Iannotti JP. Glenohumeral arthrodesis after failed prosthetic shoulder arthroplasty. J Bone Joint Surg Am 2008;90:
70-7.
8. Bilgin SS. Reconstruction of proximal humeral defects with shoulder arthrodesis using free vascularized fibular graft. J Bone Joint Surg Am 2012;94:e94.
9. Wood MB. Free vascularized fibular grafting-25 years' experience: tips, techniques, and pearls. Orthop Clin North Am 2007;38:1-12, v.