Abstract
Implant overdenture is currently a reliable alternative treatment for complete denture in an edentulous jaw. When an edentulous patient has good bone quality and quantity, a minimum of four well-spaced implants are often recommended for an implant-supported overdenture. Several clinical reports have demonstrated successful results with a maxillary overdenture supported by four unsplinted implant attachments. Self-adjusting magnet attachments have convenient clinical procedures and maintenance care compared to other solitary type systems; moreover, they have the ability to compensate for gradual bone resorption. For the rehabilitation of an edentulous atrophic maxilla with four unsplinted self-adjusting magnet attachment of implants supporting an overdenture, it may be effective compared to that of other conventional treatments. Moreover, further controlled clinical studies are needed to evaluate the effects and complications.
Key Words: edentulous maxilla, implant removable prosthesis, implant supporting overdenture, magnet attachment, overdenture
4개의 임플란트와 연결고정하지 않은 Self-Adjusting 자성 어태치먼트를 이용한 상악 무치악 환자의 오버덴처 수복 증례
박수정, 이성복, 이석원, 안수진
경희대학교 치과대학 강동경희대학교치과병원 생체재료보철과
Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture
Soo Jeong Park, Richard Leesungbok, Suk Won Lee, Su Jin Ahn
Department of Biomaterial-Prosthodontics, Kyung Hee University Dental Hospital at Gangdong, School of Dentistry, Kyung Hee University, Seoul, Korea
ISSN 1229-5418 Implantology 2014; 18(1): 38~46
Reprint requests: Su Jin Ahn
Department of Biomaterial-Prosthodontics, Kyung Hee University Dental Hospital at Gangdong, School of Dentistry, Kyung Hee University, 892, Dongnam-ro, Gangdong-gu, Seoul 134-727, Korea
Tel: 82-2-440-7518, Fax: 82-2-440-7549 E-mail: [email protected]
Received for publication: March 15, 2014 Accepted for publication: March 17, 2014
교신저자: 안수진
(134-727) 서울시 강동구 동남로 892
경희대학교 치과대학 강동경희대학교치과병원 생체재료보철과 Tel: 82-2-440-7518, Fax: 82-2-440-7549
E-mail: [email protected] 원고접수일: 2014년 3월 15일 게재확정일: 2014년 3월 17일
Copyright © 2014. The Korean Academy of Oral & Maxillofacial Implantology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits
을 때 연결고정을 하거나 그렇지 않은 경우 결과에 유의 한 차이가 없음을 보고하고 있다7. 최근 개발된 자성 유 지장치인 Magfit SX (Aichi Steel Corp., Tokai, Japan)는 연조직이 흡수됨에 따라 발생할 수 있는 문제점을 보상 하기 위한 ‘self-adjusting’ 기능을 가져 임플란트 오버덴 처에 적합하며 좋은 결과를 보이고 있다.
본 증례는 상악 무치악 환자에서 양측 견치, 구치부에 4개의 임플란트를 식립하고 자성 유지장치를 이용한 오 버덴처를 장착한 후 3년간 추적관찰한 결과, 환자만족도, 골소실(bone loss), 기능, 유지관리 등 대부분의 측면에서 만족할 만한 결과를 보였기에 이를 보고하는 바이다.
II 증례보고
76세의 남자 환자가 십여 년 전부터 사용했던 상악 부 분의치가 맞지 않는다는 주소로 내원하였다. 몇 주 전 클 래스프로 유지되던 상악 우측 제1대구치가 상실되었으며 상악은 이중관으로 수복된 좌측 상악 견치가 2도의 동요 도를 보이며 잔존해 있었다(Fig. 1). 새 의치의 제작이 필 요했고 환자가 구개부 연장을 최소로 요구하는 점, 총의 치보다 유지력이 강한 보철을 원하는 점, 대합치가 모두 자연치 또는 임플란트 고정성 보철로 강한 교합력이 예 상되는 점 등을 고려하여 임플란트를 이용한 의치제작을 계획하였다. 가철성 의치의 장기간 장착으로 인한 골소 실 양이 크고 악간 거리가 좁기 때문에 고정성 임플란트 보철이 아닌 오버덴처를 진행하기로 하였다. 오버덴처의 acrylic base는 상실된 조직의 부피를 쉽게 보상해준다3.
무치악 환자에서, 총의치 장착자들이 호소하는 많은 불편감이 임플란트 식립을 통한 오버덴 처(overdenture) 또는 고정성 보철물에 의해 극복되고 있다. 충분치 못한 유지력, 저작 시 나타나는 통증 등 총의치에서 나타나는 문제점이 임플란트 오버덴 처에서는 훨씬 줄어든다. 또한 발치 후 계속적으로 흡수 되는 골은 임플란트 식립으로 방지되고 잔존 치조제에 가해지는 부담 역시 감소되기 때문에 임플란트 오버덴처 는 환자와 임상가 모두의 입장에서 매력적인 치료옵션으 로 선택되고 있다. 또한 임플란트 오버덴처가 무치악 환 자에서 중심교합을 좀 더 안정적으로 형성하게 하며, 총 의치와 비교하여 저작력을 25% 증가시켜준다는 보고들 이 있으며1, 의치환자의 최대저작력을 300% 증가시키고2 총의치와 비교하여 저작 시 하악 움직임을 현저히 빠르 게 한다는 연구결과가 있다3. 상악 무치악 환자에서, 고 정성 임플란트 보철에 비해 임플란트 오버덴처는 낮은 비용, 수술 시 식립 위치가 상대적으로 자유로운 점, 심 하게 흡수된 치조정에 대한 보철적 재건 등의 장점을 가 진다.
상악 무치악은 임플란트의 안정과 지지에 중요하다고 생각되는 피질골이 얇거나 소실되어 있으며, 해면골의 골밀도가 낮기 때문에4 하악에 비해 더 많은 수의 임플란 트 식립이 요구된다. 하지만 임플란트 식립 개수에 대해 특별한 기준은 제시되지 못하고 있는 상황이며5,6, 최소 4 개가 상악 임플란트 오버덴처를 위한 필요 개수라고 제 시되고 있다7. 많은 연구들은 상악 무치악 환자에게 4개 의 임플란트를 식립하고 다양한 각기 다른 어태치먼트 (attachment)를 사용하여 얻은 성공적인 결과를 보고하 고 있다8.
Case Report
4개의 임플란트를 식립하여 self-adjusting 자성 어태 치먼트인 Magfit SX를 이용하기로 계획하였다. 좌측 상 악 견치 발치 후 임시의치를 제작한 뒤, 투명한 아크릴릭 레진(acrylic resin)을 이용하여 이를 복제하고, 양측 견 치 부위에 임플란트 식립을 위한 구멍을 뚫어 스텐트 (stent)를 제작하였다(Fig. 2). 스텐트에 방사선 불투과성 을 가지는 gutta percha를 부착하여 방사선 사진과 컴퓨 터 단층촬영 이미지상에서 임플란트 식립 부위를 예상하 고 확인하였으며(Fig. 3), 수술 시 식립 위치 결정에 이용 하였다. 시술 부위를 결정하고 판막을 거상하여 시술 부
위를 노출시켜 제조사의 지시에 따라서 드릴링하여 상악 좌측 견치, 상악 양측 대구치 부위는 Straumann TE (Straumann AG, Bern, Switzerland) 직경 4.1 mm × 길 이 10 mm, 골 폭이 부족한 상악 우측 견치 부위에는 Straumann TE 직경 3.3 mm × 길이 10 mm를 식립하였 고, 양측 견치부에 Bio-Oss graft (Geistlich Pharma AG, Wolhusen, Switzerland)와 흡수성 membrane을 이 용한 골유도 재생술(guided bone regeneration)을 시행하 였다(Fig. 4).
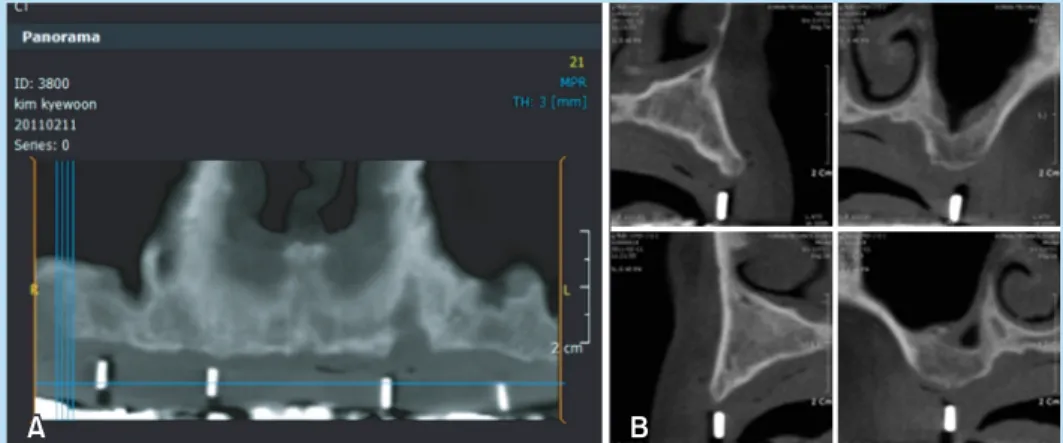
통상적인 상악 오버덴처를 위한 제작과정(예비인상, Fig. 1. Panoramic view before treatment (A) and after implant insertion (B). Four implants distributed on maxilla.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Fig. 2. Diagnostic stent (A) and surgical stent (B) for implant insertion.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture. Implantology 2014
Fig. 4. (A) Intraoral view of maxilla before implant placement. (B) Four implants placed on #13, #16, #23, and #26 area with guided bone regeneration. (C) Healing stage of bone and soft tissue.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Fig. 5. Bite registration (A) using framework of maxilla (B).
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Case Report
개인트레이, border molding, framework 제작[Fig. 5A], 중심위[centric relation]에서의 악간관계 채득[Fig. 5B], 왁스덴처 시적 및 수정, 레진중합)을 거쳐, 식립 후 6개 월 뒤 최종보철의 장착을 위해 각 임플란트에 Magfit SX 를 연결하였다. Magfit SX는 자석이 polyoxymethylene (POM) housing 안에 들어가 있어 0.4 mm의 유격을 갖
고, 8도의 뒤틀림을 허용하여 의치 장착 후 잇몸이 흡수 되거나 저작 시 자석이 떨어져서 흡착력이 감소하는 현 상을 방지한다(Fig. 6). 의치 장착 시에는 housing과 자 석 사이에 레진이 들어가는 것을 방지하면서 장착하는 것이 중요하다. 사전에 완성한 상악 의치에서 Magfit SX 를 부착할 부위의 유격을 확인한 후 Magfit 전용 지대주 를 체결한 후(Fig. 7A)에 러버댐을 사용하여 언더컷 하방 으로 자가중합 레진이 흘러 들어가는 것을 방지하였다 (Fig. 7B). 자성체를 위치시키고 floss silk를 사용하여 0.4 mm의 공간을 확보하고 의치를 passive하게 환자 구 강 내에 위치시킨 뒤, 레진 중합이 끝난 후 내면의 과잉 레진을 다듬어 환자에게 장착하였다(Fig. 8). 상악 양측 모두 제2대구치까지 배열하여 하악의 모든 자연치가 교 합이 되도록 하였다. 최후방 구개부 연장은 임플란트 오 버덴처의 장점을 살려 총의치에 비해 현저히 감소시켰 다. 하지만 치조제에서도 충분한 지지를 얻기 위하여 구 개측 치조제 사면을 의치가 피개하여 충분한 지지를 얻 으면서 임플란트에 무리한 힘이 가해지지 않도록 하였다 (Fig. 5). 오버덴처의 구개측 피개를 제거하는 것은 다른
Fig. 7. (A) Magnet attachments were connected with implant fixture. (B) Rubber dam blocked-out the acrylic resin that connected magnet abutment and mandibular prosthesis.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Fig. 6. Picture and diagram of Magfit SX (Aichi Steel Corp.). POM: polyoxymethylene.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
있으며 생물학적, 보철적 합병증 없이 만족할 만한 결과 를 보이고 있다(Figs. 9~11).
임플란트-지지 오버덴처는 전형적인 총의치와 비교해
Fig. 8. Magnet attachment in denture base. Overfilled connecting resin was removed.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Fig. 9. Frontal view after maxilla and mandible final prosthesis installation.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Fig. 10. (A) Concave facial profile before treatment. (B) Adequate facial profile after final prosthesis insertion.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-Adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
Case Report
많은 문제점과 불편감을 감소시키는 치료법으로, 환자들 의 만족도는 매우 높다1-3. 상악 임플란트 오버덴처는 임 플란트와 치조점막 모두에서 지지를 얻으므로 임플란트 고정성 보철에 비해 적은 수의 임플란트 식립이 가능하 고, 발음이나 saliva control에 문제되는 일이 더 적으며, 협측 flange를 통해 안면조직을 더 적절하게 지지한다.
또한 구강위생을 위한 접근이 쉽고, 악간 관계에 있어서 도 치아를 좀 더 이상적인 위치에 놓을 수 있으며 전악 고정성 임플란트 보철에 비해 기공오차(misfit)가 적다는 장점이 있다6.
상악 오버덴처의 성공률이 고정성 임플란트 보철의 성 공률보다 낮다고 보고되는데, 이러한 보고에서의 실패 원인을 분석한 또 다른 연구들은 골의 양과 질이 좋지 못 한 환자들이 고정성 임플란트 보철의 대상이 아닌 오버덴 처의 대상이 되기 때문에 상대적으로 낮은 생존율이 보고 될 수 밖에 없다고 언급하고 있다10. 또한 골의 양과 질이 동일한 경우 임플란트 고정성 보철과 오버덴처는 동일한 성공률을 가진다는 연구결과들이 보고되고 있다11.
최근 다양한 부착장치가 임플란트 오버덴처에 사용되 고 있다. 이러한 시스템에는 telescopic crown, bar, locator, magnet 등이 있으며, 임상가는 그들의 경험과 선호도에 따라 이러한 부착장치를 선택하게 된다. Bar를
통해 임플란트를 연결고정하는 것은 치조정이 심하게 흡 수된 환자에서 충분한 지지와 유지를 부여하는 장점을 가지고 있으며12, 전상악골에 집중해서 임플란트를 식립 하고 bar로 연결고정하는 것은 상악 임플란트 오버덴처 에서 우선적인 치료옵션으로 여겨져 왔다. 하지만 안면 고경이 낮은 환자에게는 bar structure가 들어갈 공간이 확보되지 않는 점, 혀의 불편감을 호소하는 경우가 많은 점, 구강위생 관리가 상대적으로 어려운 점, 기공과정이 복잡하며 각 단계의 정밀성이 요구되는 점 등 환자의 내 원 횟수와 임상가의 편의성, 유지관리 측면에 있어 적응 증 선택에 주의가 요구된다. 따라서 최근에는 상악골의 양과 질이 좋으며 치조제에서도 충분한 지지를 동반할 수 있는 경우, 연결하지 않은 독립적인 어태치먼트를 이 용한 오버덴처 치료법이 많이 이용되고 있다7-9. 연결고 정하지 않은 분리된 어태치먼트가 골의 상실을 가중시킨 다고 여겨왔지만, bar를 통해 연결고정을 한 경우나 연 결고정하지 않은 상부구조 사이의 임플란트 성공률과 생 존율에는 유의한 차이가 없다고 보고되고 있다13.
상악 무치악에 4개의 임플란트를 식립한 뒤 bar로 연 결고정한 경우와 연결고정하지 않고 각기 다른 독립적 어태치먼트를 사용한 환자들의 전향적 연구에서, 시간의 경과에 따른 임플란트 주위조직의 건강도, probing depth, 주위골 손실(marginal bone loss) 등에는 유의차 가 없다는 결과가 보고되었다7. 구강 기능이나 환자만족 도 역시 유의차가 없었으며, 3년간의 추적관찰 시 bar로 연결고정한 경우와 그렇지 않은 경우 성공률과 생존율 각 케이스 모두 100%였다. 이러한 보고는 4개의 임플란 트를 상악 무치악 환자에게 식립하였을 경우 성공률이 어태치먼트 종류에 영향을 받지 않는다는 것을 의미한 다. 위 연구에서 bar를 사용한 경우는 보철적 유지관리 와 합병증의 해결을 위해 내원해야 하는 횟수가 유의하 게 높았으며, 치은의 병적 증식(gingival hyperplasia)이 발생하는 경향이 있다고 보고하였다. 연결고정하지 않은 Fig. 11. Panoramic view at 3 year follow-up check.
Soo Jeong Park et al. : Rehabilitation of an Edentulous Atrophic Maxilla with Four Unsplinted Self-adjusting Magnet Attachment of Implants Supporting an Overdenture.
Implantology 2014
각도와 위치의 중요성에 대해 언급하고 있다. 임플란트 를 정확하게 위치시키는 것은 어태치먼트 시스템의 유지 에 영향을 미친다7.
또한 임플란트를 전상악골에 집중하지 않고 구치부에 분산시킬 경우 전상악 부위에 임플란트가 집중된 경우와 tuberosity까지 후방 분포된 경우를 비교한 유한요소 분 석 결과, 후자가 골에 응력이 덜 가해지는 것으로 나타났 다14. 이는 ap spread가 증가하여 골에 가해지는 응력이 감소된 결과로 여겨진다.
자성 유지장치는 지금까지 널리 사용되어 온 유지장치 의 한 종류이지만 자성체와 키퍼의 거리에 따라서 유지 력의 변화가 발생하기 때문에 임플란트 식립 이후 연조 직이 변화할 수밖에 없는 조건에서는 그 사용이 제한될 수밖에 없었다. Magfit SX는 이러한 단점을 보완하여 점 막의 움직임에 대하여 보상이 가능하도록 POM housing 을 포함한 구조를 가지고 있어(Fig. 8), 술 후에 연조직이 변하더라도 유지력 소실 없이 사용할 수 있고, 임플란트 간의 식립 각도가 완전히 평행하지 않은 경우에도 사용 할 수 있다. 자성 유지장치는 다른 solitary type 유지장 치에 비해 구강 내 작업이 편리하며 연령이 높은 환자가 착탈하기에 적합한 유지력을 갖는다. 또한 사용기간이 길어져도 자성에 의한 유지력이 소실되지 않는다는 장점 이 있다.
임플란트 상악 오버덴처는 전통적인 총의치와 비교하 여 전반적인 환자 만족도가 높으며, 저작 능력의 향상을 가져온다3,7. 여러 저자들은 상악 무치악 환자에서 4개의 임플란트와 연결고정하지 않은 어태치먼트를 이용한 이 러한 치료방법이 우수한 예후를 보여준다고 언급하고 있 다13.
지하였고 연결고정하지 않은 독립적인 어태치먼트가 가 지는 장점을 활용하였다. 지속적인 관찰결과 구강위생 관리가 용이하고 비용에 비해 환자만족도가 높으며, 주 기적인 방사선 사진 평가에서도 골소실에 있어서 만족할 만한 결과를 보이고 있다. 따라서 이는 상악 골질이 좋고 치조제의 지지를 기대할 수 있는, 비슷한 구강 내 상황을 가지는 환자에게 적용할 수 있는 좋은 술식이라고 여겨 진다. 오버덴처의 장착 이후에도 임플란트 주위 조직, 어 태치먼트를 포함한 상부구조, 보철물 자체 등의 유지관 리를 위한 내원은 매우 중요하며, 이는 하악 잔존치아가 남아있을 때 bacterial flora에 의해 감염의 위험이 있기 때문에 더욱 그렇다15.
IV 결 론
상악 무치악 환자에서 전후방 4개의 임플란트를 식립 하고 self-adjusting 기능이 있는 Magfit SX 어태치먼트 를 이용한 오버덴처의 제작은, 전신질환이 없고 골질과 양이 좋은 환자에서 상악 총의치를 대체할 수 있는 예지 성 높은 치료 방법들 중의 하나라고 할 수 있다.
References
1. Bakke M, Holm B, Gotfredsen K. Masticatory function and patient satisfaction with implant-supported mandibular overdentures: a
Case Report
prospective 5-year study. Int J Prosthodont. 2002; 15: 575-581.
2. Sposetti VJ, Gibbs CH, Alderson TH, et al. Bite force and muscle activity in overdenture wearers before and after attachment placement. J Prosthet Dent. 1986; 55: 265-273.
3. Chan MF, Närhi TO, de Baat C, et al. Treatment of the atrophic edentulous maxilla with implant-supported overdentures: a review of the literature. Int J Prosthodont. 1998; 11: 7-15.
4. Laurito D, Lamazza L, Spink MJ, et al. Tissue-supported dental implant prosthesis (overdenture): the search for the ideal protocol. A literature review. Ann Stomatol (Roma). 2012; 3: 2-10.
5. Kronström M, Widbom C, Soderfeldt B. Patient evaluation after treatment with maxillary implant-supported overdentures. Clin Implant Dent Relat Res. 2006; 8: 39-43.
6. Ekfeldt A, Christiansson U, Eriksson T, et al. A retrospective analysis of factors associated with multiple implant failures in maxillae. Clin Oral Implants Res. 2001; 12: 462-467.
7. Zou D, Wu Y, Huang W, et al. A 3-year prospective clinical study of telescopic crown, bar, and locator attachments for removable four implant-supported maxillary overdentures. Int J Prosthodont. 2013; 26:
566-573.
8. Kiener P, Oetterli M, Mericske E, et al. Effectiveness of maxillary overdentures supported by implants: maintenance and prosthetic complications. Int J Prosthodont. 2001; 14: 133-140.
9. Smedberg JI, Lothigius E, Bodin I, et al. A clinical and radiological two- year follow-up study of maxillary overdentures on osseointegrated implants. Clin Oral Implants Res. 1993; 4: 39-46.
10. Jemt T. Implant treatment in resorbed edentulous upper jaws: a three year follow up study on 70 patients. Clin Oral Implants Res. 1993; 4:
187-194.
11. Jemt T, Lekholm U. Implant treatment in edentulous maxillae: a 5-year follow-up report on patients with different degrees of jaw resorption. Int J Oral Maxillofac Implants. 1995; 10: 303-311.
12. Gotfredsen K, Holm B. Implant-supported mandibular overdentures retained with ball or bar attachments: a randomized prospective 5-year study. Int J Prosthodont. 2000; 13: 125-130.
13. Watson RM, Jemt T, Chai J, et al. Prosthodontic treatment, patient response, and the need for maintenance of complete implant-supported overdentures: an appraisal of 5 years of prospective study. Int J Prosthodont. 1997; 10: 345-354.
14. El-Sheikh AM, Shihabuddin OF, Ghoraba SM. A prospective study of early loaded single implant-retained mandibular overdentures:
preliminary one-year results. Int J Dent. 2012; 2012: 236409.
15. Chan MF, Howell RA, Cawood JI. Prosthetic rehabilitation of the atrophic maxilla using pre-implant surgery and endosseous implants. Br Dent J. 1996; 181: 51-58.