망막혈관종성증식에서 유리체강내 라니비주맙과 애플리버셉트 주입술 후 맥락막두께 변화의 비교
Comparison of the Changes in Subfoveal Choroidal Thickness after Intravitreal Ranibizumab and Aflibercept Injections in Retinal Angiomatous Proliferation
안소은, 양 헌, 전혜민, 김상원, 윤희성
Soh-Eun Ahn, Heon Yang, Hye Min Jeon, Sang Won Kim, Hee Seong Yoon
성모안과병원
Sungmo Eye Hospital, Busan, Korea
Purpose: To compare changes in choroidal thickness after intravitreal ranibizumab and aflibercept injections in patients with retinal an- giomatous proliferation (RAP).
Methods: This study involved 39 eyes (21 ranimizumab-treated eyes, 18 aflibercept-treated eyes) of 36 patients who received either intravitreal ranibizumab or aflibercept injection for the first time and followed up for more than 6 months. Subfoveal choroidal thickness was measured before intravitreal injection and at 3 and 6 months after intravitreal injection to determine any significant change in subfo- veal chorioidal thickness over time in each treatment group. The relevant changes at each time point were measured to compare differ- ences between the treatment groups. Central macular thickness and the best corrected visual acuity were measured and compared.
Results: Choroidal thickness at 3 and 6 months after injection was significantly lower than that before injection in both the ranibizumab and aflibercept groups (p < 0.001, in all). The changes in choroidal thickness were 17.7 ± 10.9 μm and 13.0 ± 11.0 μm at 3 and 6 months after ranibizumab injection, respectively, and 24.5 ± 12.5 μm and 18.3 ± 11.1 μm at 3 and 6 months after aflibercept injection, respectively. These results show that although no significant differences were observed according to injection type at 3 months, the aflibercept group ex- hibited a significantly greater decrease at 6 months (p = 0.094, 0.043). The best corrected visual acuity in the two groups was significantly improved for up to 6 months after the injection compared with before the injection, and the central macular thickness also significantly decreased. There was no significant difference in visual improvement and central macular thickness decrease between the two groups.
Conclusions: The results confirmed that both of these two drugs significantly decreased the subfoveal choroidal thickness in patients with RAP for up to 6 months after the injection, and the intravitreal injection of aflibercept tended to show a greater decrease in subfove- al choroidal thickness than the intravitreal injection of ranibizumab.
Keywords: Aflibercept; Optical coherence tomography; Ranibizumab; Retinal angiomatous proliferation; Subfoveal choroidal thickness
Address reprint requests to Hee Seong Yoon, MD
Sungmo Eye Hospital, #409-1 Haeun-daero, Haeundae-gu, Busan 48064, Korea Tel: 82-51-743-0775, Fax: 82-51-743-0776
E-mail: [email protected]
Received: 2016. 10. 7 Revised: 2016. 10. 18 Accepted: 2016. 10. 18
서론
망막혈관종성증식은 망막-망막 혹은 망막-맥락막 혈관의 문합 을 특징으로 하는 삼출성 나이관련황반변성의 한 형태로[1,2], 국내 나이관련황반변성 기초 역학조사에서는 약 6.2%를 차지 하는 것으로 나타났다[3]. 전형적인 삼출성 나이관련황반변성 과 비교하였을 때, 망막혈관종성증식으로 진단된 환자는 비교 적 나이가 많고 양안에서 발생하며[4,5], 드루젠이나 거짓드루 젠과 같은 망막의 연령관련 변성 소견이 더 높은 빈도로 보고 되고 있다[6,7].
빛간섭단층촬영(optical coherence tomography, OCT)의 발 전으로 깊이증강모드(enhanced depth imaging [EDI] mode)가 개발되면서 맥락막층을 더욱 정교하게 평가할 수 있게 되었고 [8,9], 이를 통해 망막혈관종성증식 환자에서 특징적으로 매우 얇은 맥락막두께가 보임을 확인하였다[6,10]. 일부 보고에서는 이처럼 얇은 맥락막에 의한 관류 장애가 망막혈관종성증식에서 망막내 신생혈관의 발생에 영향을 미칠 것으로 추측하였다[6].
한편, 삼출성 나이관련황반변성의 치료약제로 사용되는 항혈 관내피성장인자(anti-vascular endothelial growth factor, anti- VEGF)는 유리체강내 주사시 맥락막 층까지 침투하여 혈관수 축 효과를 나타내고 그 결과 신생혈관의 활성도를 낮추는 것으 로 알려져 있다[11-13]. 망막혈관종성증식에서도 베바시주맙, 라 니비주맙을 비롯하여 최근 애플리버셉트에 이르기까지 약제별 로 유리체강내 주입술 후 병변의 축소 및 장기적인 시력호전과 중심망막두께의 감소를 보인 연구결과들을 확인할 수 있다[14- 18]. 하지만 망막혈관종성증식 환자를 대상으로 두 종류 이상 의 약제 효과를 비교한 논문은 많지 않으며[18], 특히 맥락막두 께 변화에 미치는 영향을 비교분석한 연구는 부족한 실정이다.
이에 저자들은 처음 진단된 망막혈관종성증식 환자에서 유 리체강내 라니비주맙과 애플리버셉트 주입술 후 중심하 맥락막 두께의 변화를 비교하고, 최대교정시력 및 중심망막두께의 변 화도 함께 확인하고자 하였다.
대상과 방법
본 연구는 헬싱키 선언에 입각한 성모안과병원 의학연구윤리심 의위원회의 승인 아래 진행되었다(승인번호: 2016-BM-002-01).
2013년 6월부터 2016년 2월까지 본원을 내원한 망막혈관종성 증식 환자 중에서 치료 기왕력이 없는 환자만을 후향적 차트 분석을 통해 선택하였다. 망막혈관종성증식의 진단은 안저소 견, 형광안저혈관조영 및 인도시아닌그린혈관조영 소견을 종합 적으로 판단하여 이루어졌으며 특징적인 망막-망막 혹은 망 막-맥락막 혈관문합이 발견되는 경우에 진단하였다. 그중에서 유리체강내 라니비주맙 0.5 mg/0.05 mL (Lucentis®, Genentech
Inc., South San Francisco, CA, USA) 또는 애플리버셉트 2.0 mg/0.05 mL (Eylea®, Regeneron, New York, NY, USA and Bayer HealthCare, Berlin, Germany) 주입술을 시행 받고 6개월 이상 경과관찰이 가능했던 36명 39안을 대상으로 하였다. 주사 약제의 선택은 시술의사의 재량에 의해 이루어졌으며, 진단 후 1개월 간격으로 3회의 주사를 시행하고 이후에는 병변이 잔존 또는 재발하는 경우 추가 치료를 하였다. 첫 3회 주사 후 안저 검사나 빛간섭단층촬영에서 망막하액이 남아있거나 재발한 경 우, 새로 생긴 황반출혈, 망막색소상피박리의 크기 증가와 같은 병변의 활성 소견이 보일 경우 추가 주사를 시행하였다. 심한 매 체혼탁을 동반한 경우와 6디옵터 이상의 고도근시 환자, 시력에 영향을 줄 수 있는 다른 질환이나 병태를 동반한 경우 본 연구 에서 제외하였다. 맥락막두께에 영향을 줄 수 있는 레이저 시술 이나 유리체망막 수술을 시행 받은 경우 또한 연구에서 제외하 였다. 일반적으로 망막혈관종성증식이 아닌 전형적 삼출성 나 이관련황반변성이 진행하는 경우에도 망막-맥락막 문합이 나 타날 수 있는 것으로 알려져 있다[19]. 이를 배제하기 위해 황 반중심에 지도모양 위축이나 원반형 반흔이 관찰되는 경우 또 는 증상 발생 후 6개월 이상 경과한 경우 연구에서 제외하였다.
모든 환자는 내원 당시 최대교정시력, 안압측정, 굴절검사, 안저검사, 형광안저혈관조영, 인도시아닌그린혈관조영 및 빛 간섭단층촬영을 시행하였다. 빛간섭단층촬영은 SD-OCT (CirrusTM HD-OCT 4000, Carl Zeiss Meditec, Dublin, CA, USA)를 사용하였고, 7 이상의 신호 강도를 보이는 영상만을 분석하였다. 중심하 맥락막두께는 깊이증강영상(EDI) 기법으 로 촬영된 고해상도 라스터 스캔 영상에서 Cirrus 소프트웨어 에서 제공하는 직선측정도구(linear measurement tool)를 이용 하여, 중심와 바로 아래 지점에서 망막색소상피의 외측경계에 서부터 공막의 내측경계까지 수직선을 그어 측정하였다(Fig. 1) [8,20,21]. 두 명의 저자(ASE, YH)가 독립적으로 측정하여 도 출한 맥락막두께의 평균값을 분석에 사용하였다. 주사 전 초기 중심하 맥락막두께, 주사 후 3개월, 6개월째 중심하 맥락막두 께를 측정하였고, 각각의 시기별 중심하 맥락막두께의 측정자 간 일치도를 분석한 결과, 급내상관계수(intra-class correlation coefficient)는 주사 전 0.984 (95% confidence interval [CI]:
0.978–0.988, p<0.001), 주사 후 3개월째 0.983 (95% CI:
0.979–0.990, p<0.001), 6개월째 0.987 (95% CI: 0.982–0.991, p<0.001)로 높은 신뢰도를 보였다. 최대교정시력은 Snellen 시 력표를 사용하여 측정한 뒤 logMAR로 변환하였다. 중심망막 두께는 cube scan data로부터 계산된 Early Treatment Diabetic Retinopathy Study 영역 중에서 중심 1 mm 영역의 평균망막두 께로 정의하였다.
약제 종류에 따라 라니비주맙군과 애플리버셉트군으로 나누 고 약제그룹별로 주사 전과 비교하여 주사 후 3개월, 6개월째 중심하 맥락막두께가 의미 있는 변화를 보이는지 확인하였다.
또한 시기별로 주사 전과 주사 후 중심하 맥락막두께의 차이를 계산한 변화량이 두 약제 간에 차이를 보이는지 확인하였다. 주 사 전 맥락막두께가 두꺼울수록 큰 변화량을 보일 수 있다는 가능성을 염두에 두고 초기 맥락막두께를 기준으로 한 변화율 을 도출한 후 두 약제 간의 차이를 분석하였다(맥락막두께 변 화율[%] = 맥락막두께 변화량[μm] / 주사 전 맥락막두께[μm]
× 100). 최대교정시력과 중심망막두께도 약제그룹별로 주사 전 과 비교하여 주사 후 3개월, 6개월째 의미있는 변화를 보이는지 확인하고, 두 약제 간에 변화량의 차이를 보이는지 비교하였다.
통계분석은 SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA)을 사용하였다. 각각의 약제그룹 내에서 주사 전과 주 사 후 3개월, 6개월째 중심하 맥락막두께, 최대교정시력, 중심망 막두께의 변화는 repeated measures analysis of variance를 이용
하여 유의성을 확인하였고, 약제 종류에 따른 두 그룹별 비교는 연속형 변수의 경우 Mann-Whitney U test, 범주형 변수의 경우 카이제곱 검정 또는 Fisher’s exact test를 이용하였다. p-value가 0.05보다 작은 경우를 통계적으로 유의한 것으로 간주하였다.
결과
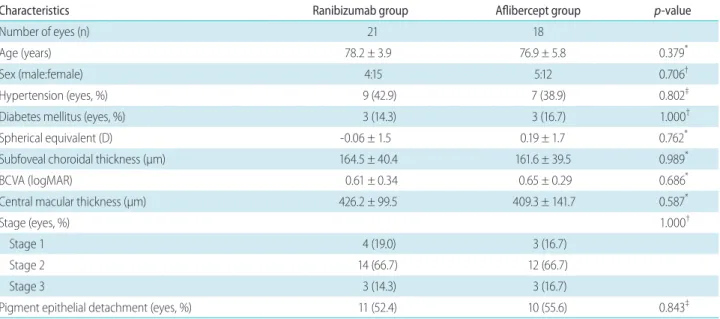
전체 대상군은 총 36명 39안으로 라니비주맙군이 21안, 애플 리버셉트군이 18안이었다. 주사약제별로 연령, 성별, 진단 당시 굴절력, 최대교정시력, 중심망막두께 및 중심하 맥락막두께를 Table 1에 제시하였으며 초기 중심하 맥락막두께를 포함한 주사 전 특성에서 두 군 간에 유의한 차이는 보이지 않았다.
A B C D
Figure 1. Representative images of retinal angiomatous proliferation. (A) Color fundus photography shows retinal hemorrhage, neovascular membrane, and multiple soft drusen. (B) Fluorescein angiography shows retinal-retinal anastomosis (RRA) (arrow). (C) Indocyanine green angiog- raphy reveals RRA (arrow). (D) Enhanced depth imaging optical coherence tomography shows subretinal neovascularization membrane above pigment epithelial detachment. Subfoveal choroidal thickness (double-head arrow) was defined as the vertical distance drawn from the outer border of the retinal pigment epithelium to the inner border of the sclera (arrowheads) beneath the very center of the fovea.
Table 1. Comparisons of baseline characteristics of 39 eyes (36 patients) with retinal angiomatous proliferation
Characteristics Ranibizumab group Aflibercept group p-value
Number of eyes (n) 21 18
Age (years) 78.2 ± 3.9 76.9 ± 5.8 0.379*
Sex (male:female) 4:15 5:12 0.706†
Hypertension (eyes, %) 9 (42.9) 7 (38.9) 0.802‡
Diabetes mellitus (eyes, %) 3 (14.3) 3 (16.7) 1.000†
Spherical equivalent (D) -0.06 ± 1.5 0.19 ± 1.7 0.762*
Subfoveal choroidal thickness (μm) 164.5 ± 40.4 161.6 ± 39.5 0.989*
BCVA (logMAR) 0.61 ± 0.34 0.65 ± 0.29 0.686*
Central macular thickness (μm) 426.2 ± 99.5 409.3 ± 141.7 0.587*
Stage (eyes, %) 1.000†
Stage 1 4 (19.0) 3 (16.7)
Stage 2 14 (66.7) 12 (66.7)
Stage 3 3 (14.3) 3 (16.7)
Pigment epithelial detachment (eyes, %) 11 (52.4) 10 (55.6) 0.843‡
Values are presented as mean ± SD or n (%).
BCVA = best corrected visual acuity; logMAR = logarithm of the minimum angle of resolution.
*p-value by Mann-Whitney U-test; †p-value by Fisher’s exact test; ‡p-value by χ2 test.
라니비주맙군의 경우, 주사 전 중심하 맥락막두께 164.5 ± 40.4 μm에서 주사 후 3개월째 146.8 ± 38.9 μm, 6개월째 151.5
± 39.4 μm로 주사 전과 비교하여 주사 후 유의한 맥락막두께 의 감소를 보였다(p<0.001, in both). 애플리버셉트군에서도 주 사 전 맥락막두께 161.6 ± 39.5 μm에서 주사 후 3개월째 137.1
± 37.6 μm, 6개월째 143.6 ± 36.2 μm로 유의한 맥락막두께의 감소를 보였다(p<0.001, in both) (Fig. 2). 두 약제 모두 평균적으 로 첫 주사 후 3개월째에 비해 6개월째 중심하맥락막두께가 두 꺼워지는 양상을 보였다(Fig. 2, 3).
중심하 맥락막두께의 변화량 및 변화율은 주사 전과 비교하 여 주사 후 3개월째, 라니비주맙군에서 17.7 ± 10.9 μm, 11.0 ± 6.2%가 감소하고, 애플리버셉트군에서 24.5 ± 12.5 μm, 15.4 ± 8.0%가 감소하였으며 애플리버셉트군에서 보다 큰 감소를 보였 으나 두 군 간의 통계학적으로 유의한 차이는 없었다(p=0.094, 0.083, respectively). 주사 후 6개월째는 라니비주맙군에서 13.0
± 11.0 μm, 8.0 ± 6.1%가 감소하고, 애플리버셉트군에서 18.3
± 11.1 μm, 11.2 ± 6.0%가 감소하였으며 애플리버셉트군이 라니비주맙군에 비해 유의하게 큰 감소를 보였다(p=0.043, in both) (Table 2). 3개월째 누적주사횟수는 3번으로 두 군에서 동일하였고, 6개월째 누적주사횟수는 라니비주맙군이 3.24 ± 0.44회, 애플리버셉트군이 3.11 ± 0.32회로 두 군 간의 유의한 차이는 없었다(p=0.512). 첫 3회 치료 후 추가 주사가 필요했 던 경우를 비교하였을 때도 라니비주맙군이 5안(23.8%), 애플 리버셉트군이 2안(11.1%)으로 두 군 간의 유의한 차이는 없었 다(p=0.418) (Table 3).
라니비주맙군의 경우, 최대교정시력(logMAR)은 주사 전, 주 사 후 3개월, 6개월째 각각 0.61 ± 0.34, 0.41 ± 0.26, 0.40 ± 0.21이었으며, 같은 시기에 측정된 중심망막두께는 각각 426.2
± 99.5 μm, 214.1 ± 34.1 μm, 215.2 ± 28.9 μm였다. 주사 후 3개월, 6개월째 최대교정시력은 주사 전과 비교하여 유의 하게 호전되었으며, 중심망막두께 역시 유의하게 감소한 결과 를 보였다(p<0.001, in all). 애플리버셉트군의 경우, 최대교정시 력(logMAR)은 주사 전, 주사 후 3개월, 6개월째 각각 0.65 ± 0.29, 0.43 ± 0.16, 0.43 ± 0.17이었으며, 같은 시기에 측정된 중 심망막두께는 각각 409.3 ± 141.7 μm, 197.4 ± 23.7 μm, 199.8
± 21.6 μm였다. 주사 후 3개월, 6개월째 최대교정시력은 주사 전과 비교하여 유의하게 호전되었으며, 중심망막두께 역시 유 A
B
C
Figure 2. Six-months changes in subfoveal choroidal thickness, best corrected visual acuity, and central macular thickness in eyes with retinal angiomatous proliferation that were treated with ran- ibizumab (closed blue diamond, blue line) or aflibercept (closed red square, red line), according to the follow-up period. (A) Subfoveal choroidal thickness after injection was significantly lower than that before injection in both the ranibizumab and aflibercept groups.
(B) Best corrected visual acuity in the two groups was significantly improved after the injection compared with before the injection, and (C) central macular thickness also significantly decreased. *p <
0.05 by repeated measures analysis of variance (ANOVA).
Table 2. Comparison of subfoveal choroidal thickness changes between patients treated with ranibizumab and those treated with aflibercept
Ranibizumab group Aflibercept group p-value*
△† 3 months (μm) 17.7 ± 10.9 24.5 ± 12.5 0.094
△‡ 3 months (%) 11.0 ± 6.2 15.4 ± 8.0 0.083
△† 6 months (μm) 13.0 ± 11.0 18.3 ± 11.1 0.043
△‡ 6 months (%) 8.0 ± 6.1 11.2 ± 6.0 0.043 Values are presented as mean ± SD unless otherwise indicated.
*p-value by Mann-Whitney U-test; †Amount of change from baseline value at each follow-up time; ‡Percentage of change from baseline val- ue at each follow-up time.
A D
B E
C F
Figure 3. Representative cases of retinal angiomatous proliferation treated with ranibizumab (left column) or aflibercept (right column). (A) A 77-year-old male patient was treated with ranibizumab. Subfoveal choroidal thickness (SFCT) (double-head arrow) at baseline was 176 μm. (B) After three monthly injections, SFCT (double-head arrow) was decreased to 133 μm. (C) He had no recurrence during the 6-months follow-up period. SFCT (double-head arrow) was rethickened to 161 μm. (D) A 74-year-old female patient was treated with aflibercept. SFCT (double-head arrow) at baseline was 174 μm. (E) After three monthly injections, SFCT (double-head arrow) was decreased to 125 μm. (F) He had no recurrence during the 6-months follow-up period. SFCT (double-head arrow) was measured to 137 μm.
Table 3. Six-months results for treatment of retinal angiomatous proliferation using either ranibizumab or aflibercept
Ranibizumab group Aflibercept group p-value* logMAR change from baseline
3 months -0.21 ± 0.26 -0.23 ± 0.17 0.626*
6 months -0.22 ± 0.23 -0.22 ± 0.19 0.770*
CMT changes from baseline (μm)
3 months 212.0 ± 88.0 211.9 ± 126.5 0.945*
6 months 211.0 ± 90.2 209.5 ± 124.5 0.945*
Number of anti-VEGF injections 3.24 ± 0.44 3.11 ± 0.32 0.512*
Number of eyes required 4th injection (%) 5 (23.8) 2 (11.1) 0.418†
Values are presented as mean ± SD unless otherwise indicated.
logMAR = logarithm of the minimum angle of resolution; CMT = central macular thickness; anti-VEGF = anti-vascular endothelial growth factor.
*p-value by Mann-Whitney U-test; †p-value by Fisher’s exact test.
의하게 감소한 결과를 보였다(p<0.001, in all) (Fig. 2). 두 약제 군을 서로 비교하였을 때, 주사 후 3개월, 6개월째 최대교정시 력의 변화 정도 및 중심망막두께의 감소 정도는 유의한 차이를 보이지 않았다(Table 3).
고찰
망막혈관종성증식은 다른 유형의 삼출성 나이관련황반변성에 비해 보다 얇은 맥락막두께를 보이며, 맥락막 위축의 발생률이 높은 질환이다[6,22,23]. 망막혈관종성증식을 유리체강내 항혈 관내피성장인자 단일요법으로 치료한 최근 연구 결과들은 시 력 및 해부학적인 호전이 장기간 유지될 수 있음을 보여주었으 나[14-18], Grunwald et al. [24,25]의 연구 결과에 따르면 맥락막 위축의 발생을 촉진시킬 수 있는 것으로 알려져 있다. Mrejen et al. [26]은 이러한 맥락막 위축의 발생이 망막혈관종성증식에서 지속적인 치료에도 불구하고 시력 악화가 발생하는 이유일 것 으로 추측하였다. 한편 Kim et al. [27]은 망막혈관종성증식에서 치료 후 경과관찰 중에 맥락막두께가 증가되는 현상이 관찰되 며 이는 재발과 관련된 소견임을 보고하였다. 이처럼 망막혈관 종성증식 환자의 진단 및 치료에 있어서 맥락막두께를 확인하고 변화를 관찰하는 것은 중요한 부분임을 알 수 있다.
유리체강내 anti-VEGF 주사가 맥락막두께에 미치는 영향에 관하여서는 다양한 연구결과가 있어왔다. 특히 OCT의 발전으 로 EDI mode가 개발되면서 맥락막층을 더욱 정교하게 평가할 수 있게 되어 관련 연구들이 활발하게 진행되었다[13,28-30]. 망 막혈관종성증식 환자를 대상으로 한 맥락막두께 관련 연구로 Kim et al. [27]의 연구를 꼽을 수 있는데, 중심하 맥락막두께와 망막혈관종성증식 병변 아래 맥락막두께가 주사 후 3개월까지 는 유의하게 감소하지만 1년까지는 그 상태가 유지되지 못함을 보고하였다. 저자들은 초기 3회 주사 후 as-needed 방식에 준한 치료를 시행한 것이 이러한 맥락막두께의 재증가 현상에 영향 을 미쳤을 것으로 보고, 망막혈관종성증식도 다른 유형의 삼출 성 나이관련황반변성과 마찬가지로 맥락막 조직이 anti-VEGF 치료에 민감하게 반응함을 시사하였다[28,29]. 본 연구에서도 두 가지 약제 모두 주사 후 3개월까지는 주사 전과 비교하여 유 의하게 중심하 맥락막두께를 감소시킴을 확인하였다. 주사 후 6 개월째는 3개월째에 비해서는 두께가 증가하는 양상을 보였으 나 여전히 주사 전과 비교하여서는 유의한 감소를 보였다. 추가 적으로 6개월 이후에 중심하 맥락막두께가 어떻게 변화하는지 확인하는 것도 중요할 것으로 보이며, 6개월째 중심하 맥락막 두께의 증가를 보인 군과 감소를 보인 군을 비교하여 이후 재발 이나 맥락막 위축 발생과의 연관성을 알아보는 것도 의미가 있 을 것으로 생각된다.
망막혈관종성증식에서 중심하 맥락막두께 관련하여 두 약제
를 비교한 결과는 Kim et al. [31]의 연구에서 찾아볼 수 있었다.
전체 삼출성 나이관련황반변성 환자를 대상으로 라니비주맙과 애플리버셉트 주사 후 3개월째 중심하 맥락막두께에 대한 효과 를 비교하고 하위유형을 분류하여 망막혈관종성증식에서의 결 과도 보고하였다. 라니비주맙은 8.8 ± 8.1 μm, 애플리버셉트는 13.6 ± 13.1 μm의 맥락막두께 감소를 보였으며, 애플리버셉트 군에서 보다 큰 감소 경향을 보이나 통계적으로 유의한 차이는 아니었다. 비교적 적은 안수가 이러한 결과에 영향을 미쳤을 것 으로 저자들은 판단하고 있다. 본 연구에서도 주사 후 3개월째 애플리버셉트군에서 보다 큰 맥락막두께 감소 경향을 보이나 통 계적으로 유의한 차이는 보이지 않았다. 주사 후 6개월째는 이 러한 경향이 보다 두드러지게 나타나며 통계적으로 유의한 차 이를 보였다. 이는 애플리버셉트가 라니비주맙에 비해 맥락막 두께를 더 많이 감소시키며[31], 애플리버셉트의 효과가 라니비 주맙에 비해 보다 오래 지속된다는 이전 연구결과들과 비슷한 맥락에서 이해할 수 있을 것으로 보인다[32,33]. 초기 중심하 맥 락막두께를 고려하여 맥락막두께의 변화율을 비교하였을 때도 마찬가지의 결과를 보였다. Kim et al. [31]의 연구에서는 삼출성 나이관련황반변성을 세 가지 하위유형으로 분류하고 그중 한 유형으로서 망막혈관종성증식을 주사 후 3개월까지 살펴본 반 면, 본 연구에서는 망막혈관종성증식만을 대상으로 보다 장기 간인 주사 후 6개월까지의 경과를 보았다는데 의의가 있다. 또 한 변화량뿐만 아니라 초기 맥락막두께를 고려한 변화율까지 상세히 기술하였다.
라니비주맙과 애플리버셉트를 비교하였을 때, 주사 후 중심 하 맥락막두께 감소에 있어서는 차이를 보였지만 총 투여 횟수 는 유의한 차이를 보이지 않았다. 망막혈관종성증식에서 맥락 막두께와 병변의 활성도 및 재발과의 연관성에 대해서는 아직 명확한 결론이 내려져있지 않은 상태이다. Kim et al. [27]은 망 막혈관종성증식에서 치료 후 경과관찰 중에 맥락막두께가 증 가되는 현상이 재발과 관련된 소견임을 보고하였으나, Maruko et al. [34]은 맥락막두께의 변화가 재발과 연관되어 있지 않다 고 보고하였다. 맥락막두께가 병변의 활성도와 강한 상관관계 를 보이는 결절맥락막혈관병증이나 중심장액성맥락망막병증과 는 망막혈관종성증식이 병태생리적인 측면에서 차이를 보이기 때문인 것으로 보이며, 망막혈관종성증식에서 맥락막두께 변화 와 활성도 및 재발과의 관계를 논하기 위해서는 보다 많은 연구 결과들이 필요할 것으로 보인다. 본 연구에서도 첫 3회 주사 후 3개월 경과시점까지는 두 약제 사이에 재발률 및 추가 주사 횟 수가 유의한 차이를 보이지 않았지만, 맥락막두께의 증가가 재 발에 선행한다는 가정하에 두 약제 사이의 맥락막두께 감소 차 이가 이후 재발률과 어떠한 연관성을 보일지에 대해서는 추가적 인 연구가 필요할 것이다.
최대교정시력과 중심망막두께 변화 관련하여서는 Kim et al.
[18]의 연구와 비슷한 결과를 보였다. 저자들은 망막혈관종성증
식을 대상으로 6개월 추적 관찰한 결과 라니비주맙과 애플리버 셉트 모두 시력을 개선하고 중심망막두께를 줄이는 데 만족할 만한 효과를 보였으며 6개월 동안의 시력변화 정도와 중심망막 두께 감소 정도는 두 약제 사이에 통계적으로 유의한 차이가 없 었다고 보고하였는데, 본 연구에서도 마찬가지의 결과를 보여 두 약제 모두 망막혈관종성증식을 치료하는 데 있어서 주사 후 6개월까지는 좋은 효과를 기대할 수 있으며 시력호전이나 중심 망막두께 변화에 있어서는 특정 약제가 더 우위에 있지 않다는 것을 뒷받침해주었다.
본 연구는 후향적인 단면연구법에 의한 분석이고, 경과관찰 기간이 6개월로 짧았다는 점에서 제한점이 있다. Small sample size에서 오는 통계적인 문제점도 배제하기 힘들다. 약제 선택에 있어서 기준이 되는 지침이 부재하였다는 것 또한 큰 제한점이 다. 담당의사의 재량에 의해 약제가 선택되었고 이에 따른 변수 가 작용하였을 것으로 보인다. 또한 맥락막두께에 영향을 미칠 수 있는 요소들이 충분히 보정되지 않았다. 기존 보고에 따르면 맥락막두께는 일중변동, 굴절력, 안축장, 고혈압 및 당뇨의 유 무와 연관되어 있다[35-38]. 초기 특성 비교에서 굴절력, 고혈압, 당뇨의 유무가 두 군간에 유의한 차이를 보이지 않음을 확인하 였지만, 후향적 단면연구인 관계로 모든 요인들이 통제될 수는 없었다. 마지막으로 맥락막두께 측정의 경우 두께를 측정하는 객관적인 소프트웨어의 부재로 주관적인 측정법에 의해 연구가 진행되었다는 한계점을 갖는다. 그러나 이미 발표된 문헌과 같 은 방법을 사용하여 두 명의 저자가 측정하였고 측정자간 신뢰 도가 높았다는 점에서 주관성으로 인한 한계를 어느 정도 보완 하였다고 판단된다.
라니비주맙과 애플리버셉트 주사 후 맥락막두께의 감소는 신 생혈관의 활성도와 연관되어 있는 맥락막모세혈관 과투과성의 감소를 반영한다는 측면에서 긍정적인 반응으로 볼 수 있으나, 한편으로는 맥락막의 순환장애와 위축을 유발하여 망막색소상 피와 망막외층간의 결합력에 원치 않는 악영향을 미칠 수 있다 는 측면에서 치료시 주의를 기울일 필요성이 있다. 구조적인 호 전뿐만 아니라 기능적인 호전의 여부가 실제 환자를 치료함에 있어서 중요하기 때문이다. 본 연구를 통해 망막혈관종성증식 에서 유리체강내 주입술 시행 전후로 라니비주맙군과 애플리버 셉트군 모두 주사 후 6개월까지 효과적으로 중심하 맥락막두께 를 감소시키고, 애플리버셉트군에서 라니비주맙군에 비해 보다 큰 감소량을 보임을 확인하였으며, 추후 이러한 경향이 재발 또 는 맥락막 위축의 발생, 시력 예후 등에 어떠한 영향을 미칠지 에 대한 연구 또한 매우 중요할 것으로 보인다.
Conflicts of interest There are no conflicts of interest.
References
1. Yannuzzi LA, Negrão S, Iida T, et al. Retinal angiomatous proliferation in age-related macular degeneration. Retina 2001;21:416-34.
2. Freund KB, Ho IV, Barbazetto IA, et al. Type 3 neovascularization:
the expanded spectrum of retinal angiomatous proliferation.
Retina 2008;28:201-11.
3. Park KH, Song SJ, Lee WK, et al. The results of nation-wide registry of age-related macular degeneration in Korea. J Korean Ophthalmol Soc 2010;51:516-23.
4. Gross NE, Aizman A, Brucker A, et al. Nature and risk of neovascularization in the fellow eye of patients with unilateral retinal angiomatous proliferation. Retina 2005;25:713-8.
5. Bottoni F, Massacesi A, Cigada M, et al. Treatment of retinal angiomatous proliferation in age-related macular degeneration:
a series of 104 cases of retinal angiomatous proliferation. Arch Ophthalmol 2005;123:1644-50.
6. Kim JH, Kim JR, Kang SW, et al. Thinner choroid and greater drusen extent in retinal angiomatous proliferation than in typical exudative age-related macular degeneration. Am J Ophthalmol 2013;155:743-9, 749.e2.
7. Cohen SY, Dubois L, Tadayoni R, et al. Prevalence of reticular pseudodrusen in age-related macular degeneration with newly diagnosed choroidal neovascularisation. Br J Ophthalmol 2007;91:354-9.
8. Spaide RF, Koizumi H, Pozzoni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol 2008;146:496–500.
9. Mrejen S, Spaide RF. Optical coherence tomography: imaging of the choroid and beyond. Surv Ophthalmol 2013;58:387–429.
10. Yamazaki T, Koizumi H, Yamagishi T, Kinoshita S. Subfoveal choroidal thickness in retinal angiomatous proliferation. Retina 2014;34:1316-22.
11. Peters S, Heiduschka P, Julien S, et al. Ultrastructural findings in the primate eye after intravitreal injection of bevacizumab. Am J Ophthalmol 2007;143:995-1002.
12. Schraermeyer U, Julien S. Effects of bevacizumab in retina and choroid after intravitreal injection into monkey eyes. Expert Opin Biol Ther 2013;13:157-67.
13. Ünlü C, Erdogan G, Onal Gunay B, et al. Subfoveal choroidal thickness changes after intravitreal bevacizumab therapy for neovascular age-related macular degeneration. Int J Ophthalmol 2015;8:849-51.
14. Cho HJ, Lee TG, Han SY, et al. Long-term visual outcome and
prognostic factors of Intravitreal anti-vascular endothelial growth factor treatment for retinal angiomatous proliferation.
Graefes Arch Clin Exp Ophthalmol 2016;254:23-30.
15. Gharbiya M, Parisi F, Cruciani F, et al. Intravitreal anti-vascular endothelial growth factor for retinal angiomatous proliferation in treatment-naive eyes: long-term functional and anatomical results using a modified PrONTO-style regimen. Retina 2014;34:298-305.
16. Kim DB, Kim JH, Jeong SH, et al. Twelve-month outcomes of intravitreal anti-vascular endothelial growth factor therapy for retinal angiomatous proliferation. J Korean Ophthalmol Soc 2013;54:1700-7.
17. Oishi A, Tsujikawa A, Yamashiro K, et al. One-year result of aflibercept treatment on age-related macular degeneration and predictive factors for visual outcome. Am J Ophthalmol 2015;159:853-60.e1.
18. Kim OJ, Kim JH, Kim JW, et al. Comparison of short-term clinical outcomes between intravitreal ranibizumab and aflibercept in retinal angiomatous proliferation. J Korean Ophthalmol Soc 2016;57:243-7.
19. Riusala AM, Immonen IJ. Predictors of structural findings in old disciform lesions. Am J Ophthalmol 2004;138:245-53.
20. Margolis R, Spaide RF. A pilot study of enhanced depth imaging optical coherence tomography of the choroid in normal eyes.
Am J Ophthalmol 2009;147:811-5.
21. Chung SE, Kang SW, Lee JH, Kim YT. Choroidal thickness in polypoidal choroidal vasculopathy and exudative agerelated macular degeneration. Ophthalmology 2011;118:840-5.
22. Xu L, Mrejen S, Jung JJ, et al. Geographic atrophy in patients receiving anti-vascular endothelial growth factor for neovascular age-related macular degeneration. Retina 2015;35:176-86.
23. McBain VA, Kumari R, Townend J, Lois N. Geographic atrophy in retinal angiomatous proliferation. Retina 2011;31:1043-52.
24. Grunwald JE, Daniel E, Huang J, et al. Risk of geographic atrophy in the comparison of age-related macular degeneration treatments trials. Ophthalmology 2014;121:150-61.
25. Grunwald JE, Pistilli M, Ying GS, et al. Growth of geographic atrophy in the comparison of age-related macular degeneration treatments trials. Ophthalmology 2015;122:809-16.
26. Mrejen S, Jung JJ, Chen C, et al. Long-term visual outcomes for a treat and extend anti-vascular endothelial growth factor regimen in eyes with neovascular age-related macular degeneration. J Clin Med 2015;4:1380-402.
27. Kim YK, Park SJ, Woo SJ, Park KH. Choroidal thickness change after intravitreal anti-vascular endothelial growth factor treatment in retinal angiomatous proliferation and its recurrence. Retina 2016;36:1516-26.
28. Yamazaki T, Koizumi H, Yamagishi T, Kinoshita S. Subfoveal choroidal thickness after ranibizumab therapy for neovascular age-related macular degeneration: 12-month results.
Ophthalmology 2012;119:1621-7.
29. Koizumi H, Kano M, Yamamoto A, et al. Short-term changes in choroidal thickness after aflibercept therapy for neovascular age-related macular degeneration. Am J Ophthalmol 2015;159:627-33.
30. Branchini L, Regatieri C, Adhi M, et al. Effect of intravitreous anti-vascular endothelial growth factor therapy on choroidal thickness in neovascular age-related macular degeneration using spectral-domain optical coherence tomography. JAMA Ophthalmol 2013;131:693-4.
31. Kim JH, Lee TG, Chang YS, et al. Short-term choroidal thickness changes in patients treated with either ranibizumab or aflibercept: a comparative study. Br J Ophthalmol 2016 Mar 7.
[Epub ahead of print]
32. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration.
Ophthalmology 2012;119:2537-48.
33. Stewart MW, Rosenfeld PJ. Predicted biological activity of intravitreal VEGF Trap. Br J Ophthalmol 2008;92:667-8.
34. Maruko I, Iida T, Oyamada H, et al. Subfoveal choroidal thickness changes after intravitreal ranibizumab and photodynamic therapy for retinal angiomatous proliferation. Retina 2015;35:648- 54.
35. Tan CS, Ouyang Y, Ruiz H, et al. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci 2012;53:261–6.
36. Ikuno Y, Kawaguchi K, Nouchi T, et al. Choroidal thickness in healthy Japanese subjects. Invest Ophthalmol Vis Sci 2010;51:2173–6.
37. Akay F, Gundogan FC, Yolcu U, et al. Choroidal thickness in systemic arterial hypertension. Eur J Ophthalmol 2016;26:152–7.
38. Querques G, Lattanzio R, Querques L, et al. Enhanced depth imaging optical coherence tomography in type 2 diabetes.
Invest Ophthalmol Vis Sci 2012;53:6017–24.
망막혈관종성증식에서 유리체강내 라니비주맙과 애플리버셉트 주입술 후 맥락막두께 변화의 비교
목적: 망막혈관종성증식 환자에서 유리체강내 라니비주맙과 애플리버셉트 주입술 후 중심하맥락막두께의 변화를 비교하고자 한다.
대상과 방법: 처음으로 망막혈관종성증식으로 진단된 후 라니비주맙 또는 애플리버셉트 주입술을 시행 받고 6개월 이상 경과관찰 가능 했던 36명 39안(라니비주맙 21안, 애플리버셉트 18안)을 대상으로 하였다. 첫 주사 전, 주사 후 3개월, 6개월째 중심하맥락막두께를 측정하여 약제군별로 시간에 따라 의미 있는 변화를 보이는지 확인하였고, 시기별 변화량을 측정하여 약제에 따른 차이를 비교하였다.
최대교정시력 및 중심망막두께도 함께 측정하여 비교하였다.
결과: 라니비주맙군과 애플리버셉트군 모두 주사 전 중심하맥락막두께와 비교하여 주사 후 3개월, 6개월째 통계적으로 유의한 감소를 보였다(p<0.001, in all). 라니비주맙 주사 후 3개월, 6개월째 변화량은 17.7 ± 10.9 μm, 13.0 ± 11.0 μm, 애플리버셉트 주사 후 변화량은 24.5 ± 12.5 μm, 18.3 ± 11.1 μm로 애플리버셉트군에서 보다 큰 변화량을 보였으며 3개월째는 통계학적으로 유의한 차 이가 없었으나 6개월째는 유의한 차이를 보였다(p=0.094, 0.043). 두 군 모두에서 최대교정시력 및 중심망막두께는 주사 전과 비교 하여 주사 후 6개월까지 유의하게 호전되었으며, 호전정도는 두 군 사이에 유의한 차이를 보이지 않았다.
결론: 망막혈관종성증식 환자의 치료에서 두 약제 모두 주사 후 6개월까지 유의하게 중심하맥락막두께를 감소시켰고, 애플리버셉트를 주사하였을 때 라니비주맙에 비해 보다 큰 맥락막두께 감소를 보이는 경향을 확인하였다.
국문초록