228
Corresponding to: Kyo-Young Song, M.D., Department of Surgery, The Catholic University of Korea, Kangnam St. Mary's Hospital, 505 Banpo-dong, Seocho-gu, Seoul, Korea. Tel: +82-2-590-2728, Fax: +82-2-590-1406, E-mail: [email protected]
Received October 15, 2007, Accepted December 31, 2007
Departments of Surgery and
1Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea
Min-Hyung Kim, M.D., Kyo-Young Song, M.D., Jung-Ho Shim, M.D., Chan-Kwon Jung, M.D., Ph.D.
1, Seung-Nam Kim, M.D., Ph.D. and Cho-Hyun Park, M.D., Ph.D.
Laparoscopic Wedge Resection of GISTs Involv- ing the Second Portion of the Duodenum
Min-Hyung Kim, M.D., Kyo-Young Song, M.D., Jung-Ho Shim, M.D., Chan-Kwon Jung, M.D., Ph.D.
1, Seung-Nam Kim, M.D., Ph.D. and Cho-Hyun Park, M.D., Ph.D.
Departments of Surgery and
1Pathology, College of Medi- cine, The Catholic University of Korea, Seoul, Korea The optimal surgical procedure for treatment of gastro- intestinal stromal tumors (GISTs) of the duodenum remains undefined. Therefore, various surgical procedures have been introduced as treatment options for duodenal GISTs. Due to the anatomical complexity, the laparoscopic approach has been considered as a contraindication. Especially for GISTs located at the second portion of the duodenum, a laparo- scopic wedge resection is technically difficult to perform. We describe the surgical technique of laparoscopic wedge re- section with hand-sewn closure for GISTs that involve the second portion of the duodenum. (J Korean Surg Soc 2008;74:228-232)
Key Words: Duodenum, Gastrointestinal stromal tumors (GISTs), Laparoscopic wedge resection, Hand- sewn closure
INTRODUCTION
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors arising within the gastrointestinal tract.(1) The stomach is the most
common site of GISTs, and about 20% of these are found in the duodenum.(2) They rarely involves the lymphatic channels, therefore, local resection without lymph node dissection has been the treatment choice.
For the duodenal GISTs, the type of approach and the extent of resection should be determined by the size and exact site of the lesion.(3 5) Because of the anatomic complexity, laparoscopic approach has been considered as a contraindication. Especially, the GISTs located at the 2
ndportion of duodenum, laparoscopic wedge resection is technically difficult. Uehara et al.(6) reported that 40% of patients with duodenal GISTs required pancreaticoduodenectomy for treat- ment. However, since this procedure has been asso- ciated with excessive morbidity, it should be reser- ved for the patients with high risk potential of malig- nant disease.
We described here the surgical technique of lapa- roscopic wedge resection with hand-sewn closure for the GISTs that involved the second portion of the duodenum.
CASE REPORT
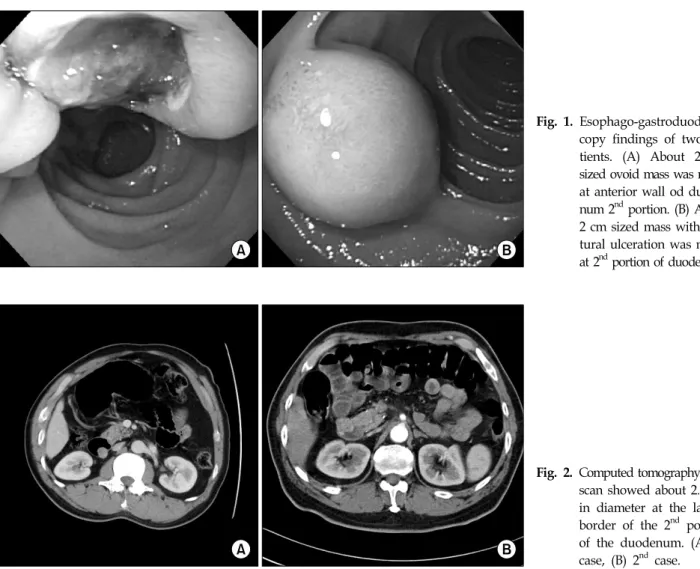
A 44 old man visited a local hospital for routine esophagogastroduodenoscopic examination (EGD), and this revealed the presence of tumor in the second portion of the duodenum (Fig. 1A). Upon admission, the patient appeared well-nourished and the physical examination findings were unremarkable.
Laboratory evaluation showed the peripheral blood
cell count, blood chemistry and serum tumor mar-
kers to be within the normal limits. The computed
tomography (CT) scan revealed a tumor measuring
2.0 cm in diameter at the duodenum's 2
ndportion
(Fig. 2A).
Fig. 1. Esophago-gastroduodenos copy findings of two pa- tients. (A) About 2 cm sized ovoid mass was noted at anterior wall od duode- num 2
ndportion. (B) About 2 cm sized mass with cen- tural ulceration was noted at 2
ndportion of duodenum.
Fig. 2. Computed tomography (CT) scan showed about 2.0 cm in diameter at the lateral border of the 2
ndportion of the duodenum. (A) 1
stcase, (B) 2
ndcase.
The second patient was a 62-year-old male who presented to our out-patient clinic with intermittent epigastric pain and tarry stools for 2 months. For the laboratory data, the complete blood counts showed a hemoglobin level of 9.6 g/dl and a hematocrit of 29.5%, and the blood chemistry and serum tumor marker were within the normal limits. EGD showed a 2.0×2.0 cm sized ulcerofungating mass at the 2
ndportion of the duodenum (Fig. 1B). Subsequent hypotonic duodenography revealed a bulging mass with ulceration. CT revealed a tumor measuring 2.0 cm in diameter at the lateral border of the 2
ndportion of the duodenum (Fig. 2B).
In both patients, the tumors were less than 2 cm and the expanding nature was mainly endophytic with slight exophytic. Therefore, the authors decided to perform the surgery laparoscopically.
Under the general anesthesia, these patient were placed in a supine position with the surgeon and
assistant standing at the patient's right side. A nasogastric tube was not inserted. A 10 mm camera port was inserted just below the umbilicus with using the open technique (Hasson's method). Carbon dioxide was insufflated through this port to create a pneumoperitoneum with an insufflation pressure of 12 mmHg. Two additional 5 mm ports were inserted in the upper abdomen to identify the tumor location and two more 10 mm ports were placed to allow for manipulation of the duodenum (Fig. 3). The pelvic cavity and abdominal organ surfaces were inspected, including the liver and gastrocolic ligament. No signs of metastasis or invasion were found.
The patients were placed in the reverse-Trendelen-
burg position and tilted to the left. A laparoscopic
Kocher maneuver was then performed. To expose the
2
ndportion of duodenum, the retroperitoneum is
dissected out and lifted up to the level of the inferior
vena cava with using ultrasonic coagulating shears
Fig. 3. Trocar placement.
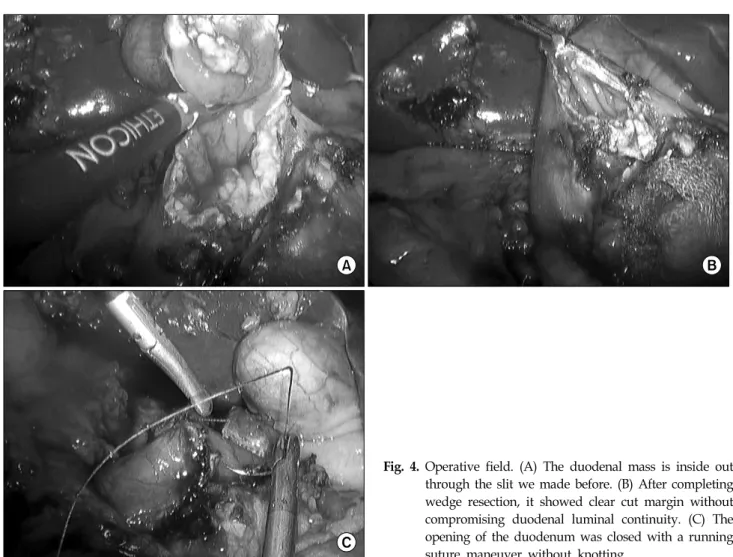
Fig. 4. Operative field. (A) The duodenal mass is inside out through the slit we made before. (B) After completing wedge resection, it showed clear cut margin without compromising duodenal luminal continuity. (C) The opening of the duodenum was closed with a running suture maneuver without knotting.
ing off the duodenum, we could fully pulled out the SMT lesion and then performed wedge resection with clear cut margin with the ultrasonic coagulating shears (Fig. 4A and 4B). The opening window of the duodenum we made before could be stitched by a continuous running suture technique intracorporeally (Fig. 4C). Reinforcement was then done two times to prevent duodenal leakage. After saline irrigation, a closed suction drain was left in the Morrison's pouch.
For the first case, the operative time was 120 min
and the estimated blood loss was 50 ml. The patho-
logic exam revealed a low risk GIST. The postoperative
course was unremarkable and he started sips of
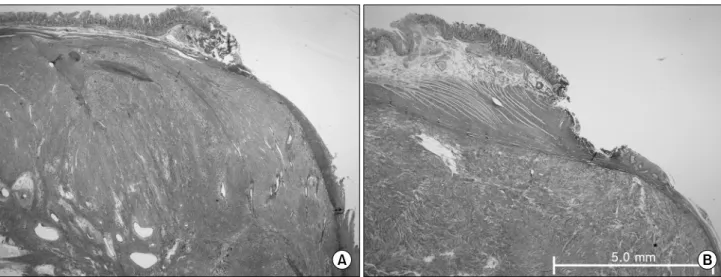
Fig. 5. Pathological finding of the 1
stcase. It showed negative margin status. (A) 1
stcase, (B) 2
ndcase.
Fig. 6. Hypotonic duodenography showed no passage dis- turbance or leakage.
water 2
ndpostoperative day; he was discharged on the 5
thpostoperative day.
For the second case, the operative time was 125 min and the estimated blood loss was 100 ml, and there was no significant complication during the surgery. The pathologic finding confirmed the tumor as a low risk GIST without margin involvement (Fig.
5). The patient was able to resume sips of water at 3
rdpostoperative day and he was discharged 6 days after the operation. A hypotonic gastrograffin swal- lowing test was performed before discharge, and it showed no leakage or passage disturbance (Fig. 6).
DISCUSSION
Since every GIST is now considered as potentially malignant,(7) all GISTs may need to be resected, even in small lesions and the optimal surgical treatment of the GIST entails complete removal of the tumor with clear surgical margins and routine lymph node dissection is not indicated,(1) because the lymph node involvement is infrequent. On the other hand, since not all submucosal tumors are GIST, a pre- operative pathologic diagnosis should be obtained.
Unfortunately, however, the diagnostic accuracy of various radiologic examinations remains largely uncer- tain. Therefore, if the lesion cannot definitely be proven to be benign in preoperative period, submu- cosal tumor should be resected with safe margin regardless of tumor size.
The optimal surgical procedure for GISTs located at the 2
ndportion of the duodenum is determined by the tumor size and the exact location of the tumor.
For the large sized GISTs which have the greater possibility of malignant risk,(8) more radical proce- dures such as pancreaticoduodenectomy can be con- sidered. However, wedge resection with clear margin is sufficient for the small sized GISTs.
Because the 2
ndportion of duodenum is develop-
mentally retroperitoneal organ and is located near by
the complex vascular structure, the laparoscopic local
resection of the tumor has been considered tech-
nically difficult. For the submucosal tumors located
at 2
ndportion of duodenum, the preoperative or
operative localization, such as intraoprtative duod- enoscopy or laparoscopic ultrasound should be applied to prevent the injury.
The endoscopic linear stapler is very useful for the most of the wedge resection of stomach, however, is not suitable to access the duodenal lesion because of its typical features. If when surgeons simply tried to resect the lesion with using the linear stapler only, then it is likely that the retrieved specimen is contained excessive normal tissue. Therefore, consi- dering its three dimensional slop, the duodenal lesion should be cut out just like tailoring method, and should be stitched by the suture technique. And to prevent the entanglement of the suture material itself, we strongly recommend using running suture technique. Also, the closure line of the duodenum should be perpendicular to the flow of the duo- denum to prevent the stricture.
Although the laparoscopic wedge resection of duodenal masst requires the experienced hands, especially for the intracorporeal suture technique, this type of minimal approach can be safely per- formed in selected patients. However, for the tumor located at posterior wall of duodenum, mesenteric
REFERENCES
1) Morinaga N, Sano A, Katayama K, Suzuki K, Kamisaka K, Asso T, et al. Laparoscopic transgastric tumor-everting resection of the gastric submucosal tumor located near the esophagogastric junction. Surg Laparosc Endosc Percutan Tech 2004;14:344-8.
2) Pidhorecky I, Cheney RT, Kraybill WG. Gastrointestinal stromal tumors: current diagnosis, biologic behavior, and management. Ann Surg Oncol 2000;7:705-12.
3) Sakamoto Y, Yamamoto J, Takahashi H. Segmental resection of third portion of the duodenum for a gastrointestinal stromal tumors: a case report. Jpn J clin Oncol 2003;33:364-6.
4) Crosby JA, Catton CN, Davis A. Malignant gastrointestinal stromal tumors of the small intestine: a review of 50 cases from a prospective database. Ann Surg Oncol 2001;8:50-9.
5) Sturgeon C, Chejfec G, Espat NJ. Gastrointestinal stromal tumors: a spectrum of disease. Surg Oncol 2003;12:21-6.
6) Uehara K, Hasegawa H, Ogiso S. Gastrointestinal stromal tumor of the duodenum: diagnosis and treatment. Geka 2001;63:1058-61.
7) DeMatteo RP, Lewis JJ, Leung D. Two hundred gastro- intestinal stromal tumors: recurrence patterns and progno- stic factors for survival. Ann Surg 2000;231:51-8.
8) Neuhaus SJ, Texler M, Hewett PJ, Watson DI. Port-site metastases following laparoscopic surgery. Br J Surg 1998;85:
735-41.