대한소화기학회지 1999;34:10 - 20
2)
접수: 1998년 5월 23일, 승인: 1998년 6월 18일 연락처: 방춘상, 442-060, 경기도 수원시 팔달구 지동 93
가톨릭의과대학 부속 성빈센트병원 내과 Tel: (0331) 240-2522, Fax: (0331) 253-8898
※ 본 연구는 1998년도 수원 성빈센트병원 연구비로 이루 어졌음.
서 론
세계보건기구(World Health Organization)는 H.
pylori 감염이 위암 발생에 중요한 역할을 한다고 정
H elic ob act e r p y lori 감염이 아포토시스, B c l- 2 및 세포 증식에 미치는 영향
가톨릭대학교 의과대학 내과학교실, 병리학교실*
방춘상・최명규・김진일・한석원・정인식・박두호・장은덕*
E ffe c t s o f H el i c ob a c t er p yl or i In fe c t i o n o n Ap o p t o s i s , B c l -2 a n d Ce l l P r o li fe r a t i o n
Ch o o n S a n g B h a n g , M.D., Myu n g Gy u Ch o i , M.D., J in Il Ki m , M.D., S o k Won Ha n , M.D., In S i k Ch u n g , M.D., D o o H o P a rk , M.D.
a n d Eu n D e o k Ch a n g , M.D.*
Departments of Internal Medicine and Pathology* College of Medicine, The Catholic University of Korea, Seoul, Korea
Background/Aims: Helicobacter pylori may promote gastric carcinogenesis mediated by the induc
tion of gastric epithelial cell proliferation. Programmed cell death (apoptosis) is linked to cell pro liferation and the bcl-2 oncogene inhibit apoptosis. The aim of this study was to assess the effect of H. pylori infection on apoptosis, Bcl-2 and gastric epithelial proliferation in chronic gastritisMethods: We examined the apoptosis with in situ TdT-mediated dUTP nick end labeling and the
proliferating cell nuclear antigen (PCNA) and Bcl-2 with immunohistochemical staining. Results: Hpylori-positive patients showed significantly higher apoptosis index and PCNA index (2.81±1.19 and
5.13±2.0, respectively) than negative patients (1.69±0.99 and 2.90±1.50, respectively). Successful eradication of H. pylori infection significantly reduced apoptosis and epthelial proliferation (The indices are 1.10±0.75 and 2.94±1.32). Apoptosis index was significantly related to PCNA index Bcl-2 expression was not different between H. pylori-positive and negative patients. Conclusions:This study suggests that H. pylori infection may increase apoptosis and epithelial proliferation, and such increases are reversed by the eradication of H. pylori. (Kor J Gastroenterol 1999;34:10 - 20
Key Words: H. pylori, Apoptosis, PCNA, Bcl-2, Gastric cancer
방춘상 외 6인. Helicobacter pylori 감염이 아포토시스, Bcl-2 및 세포 증식에 미치는 영향 11
의하고 H. pylori의 감염을 group I carcinogen, 즉 확실한 위암의 원인이라고 규정하였다.1 H. pylori가 위암을 일으키는 기전은 아직 확실히 밝혀지지 않 았으나, H. pylori 감염에 의한 비타민 C 농도의 감 소2-5 및 위상피세포의 과증식 등6-8이 제시되고 있 다.
세포의 사망에는 두 가지 기전, 즉 세포 괴사(ne- crosis)와 programmed cell death (apoptosis; 아포토 시스)가 있으며 세포의 수 및 조직의 통합성(inte- grity)은, 세포 증식과 아포토시스에 의한 세포 소실 의 균형에 의해 유지된다. 이러한 균형이 깨지면서 여러 가지 질병이 발생하게 되며,9 다양한 종양에서 아포토시스와 세포의 증식이 증가됨이 관찰되었 다.10-13 특히 포유류의 위장관 상피세포의 수는 주로 아포토시스에 의해 조절되는데14 H. pylori에 감염된 만성 위염에서도 세포 사망은 괴사에 의한 것은 거 의 없이 주로 아포토시스에 의해 일어난다고 하였 다.15 또한 H. pylori 감염에 의해 위상피세포의 과증 식이 일어나는데,6-8 이러한 상피세포의 과증식은 H.
pylori 감염에 의한 세포 손상이나 사망을 반영하며 아포토시스의 증가에 의해 유발될 수 있을 것으로 보고되고 있다.16 암유전자인 bcl-2는 세포의 증식에 는 거의 영향을 미치치 않으나 아포토시스를 억제하 여 세포 사망을 막는 역할을 하며 암 발생에도 관여 하는 것으로 알려져 있다.17,18
1998년 한 연구19에서 위암 발생에 있어 정상 위 점막이 표재성 위염, 만성 위축성 위염, 장상피화생, 이형성을 거쳐 암으로 발전되는 모델을 제시하였다.
위암의 대부분은 위축성 변화가 있는 점막에서 발생 되고20 위축성 위염이 있는 사람에서 위암의 발생이 높은 것으로 알려져 있다.21 현재 위축성 위염이나 장상피화생은 위암의 전구병소로 인정되고 있으며 22-25 특히 H. pylori 감염은 위암 발생 과정 중 조기 에 관여할 것으로 생각된다.8
본 연구의 목적은 첫쩌, H. pylori 음성이면서 내시 경 및 조직학적으로 위염의 소견이 없는 비궤양성 소 화불량 환자와 H. pylori 감염이 있는 만성 위염 환자 에서 위상피의 아포토시스, 세포 증식 및 Bcl-2 발현 의 차이를 조사하고 둘째, 이러한 차이가 균 박멸치 료 후에 개선될 수 있는지를 관찰하는 것이었다.
대상 및 방법
1. 대 상
비궤양성 소화불량 증상을 주소로 성빈센트병원 을 방문한 환자 중 위내시경검사에서 정상이거나 위 축성 위염 및 발적성 위염 등의 만성 위염의 소견을 보였던 환자를 대상으로 하였다. 내시경검사 최소 4 주 전 비스테로이드계 항염제, 스테로이드, 프로스 타글란딘 유사체, 위산 분비를 억제시키는 약제 및 항생제 등을 복용한 환자, 소화성 궤양의 기왕력이 있는 환자, 내시경 소견에서 위 또는 십이지장궤양, 종양, 역류성 식도염의 소견을 보인 환자는 대상에 서 제외하였다. 총 47예의 대상 환자를 3군으로 나 누어 H. pylori 음성이고 내시경 및 조직학적으로 정 상 소견을 보인 21예의 환자를 1군으로 하였고, H.
pylori 양성이면서 내시경 및 조직학적으로 만성 위 염의 소견을 보인 26예의 환자 중 박멸치료에 성공 하지 못했던 환자 6예를 2군으로, 성공적인 박멸치 료가 되었던 20예를 3군으로 분류하였다.
2. 위내시경검사 및 H . p y lori 감염의 확인 내시경 및 조직학적검사에서 정상이거나 만성 위 염의 소견을 보인 47명의 환자를 대상으로 유문륜에 서 2-3 cm 떨어진 전정부에서 3개(2개는 대만부, 1 개는 소만부), 분문부에서 8 cm 떨어진 체부에서 2 개(1개는 대만부, 1개는 소만부)의 조직생검을 실시 하였다. 전정부에서 생검한 1개의 조직은 즉시 rapid urease 검사 kit (CLOtest: Delta West Pty Ltd, Wes tern Australia)에 접종하여 실온에서 24시간 이내에 medium의 색깔이 붉은색으로 변화되면 양성으로 판 정하였다. 나머지 위생검조직을 10%의 중성 완충포 르말린용액과 80% 알콜용액에 4 에서 밤새 고정시 키고 파라핀에 포매하여 4 μm 두께의 연속절편을 만든 후 hematoxylin-eosin 염색 및 Warthin-Starry silver 염색을 하였다. urease 검사 및 병리조직학적 검색법을 통해 H. pylori의 존재 여부를 확인하여 둘 중 한 군데에서라도 세균의 존재를 확인하면 양성으 로 판단하였다.
12 The Korean Journal of Gastroenterology : Vol. 34, No. 1, 1999
3. H . p y lori 박멸치료 및 추적 검사 H. pylori에 감염된 군에서는 amoxicillin 1,000 mg, omeprazole 20 mg 및 clarithromycin 500 mg을 하루 두 번 10일간 복용시킨 후 4-6주 이내에 다시 내시경검사를 시행하여 같은 방법으로 urease 시험 및 병리조직학적 검색법을 시행하였고 두 가지 검사 에서 모두 음성으로 나올 때 H. pylori가 박멸된 것 으로 판정하였다.
4. 아포토시스검사(in s it u T dT - m edia t ed dUT P n ick e n d la b elin g )
ApopTag (in situ apoptosis detection kit: Oncor, Germany)을 이용하여 검사하였다. 위생검조직을 파 라핀에 포매하여 4 μm 두께로 절편을 만든 것을 다 시 파라핀을 제거한 후 proteinase K (20 μg/ml)로 실온에서 15분 동안 처리한 후 증류수로 각 2분씩 4 번 씻어내어 조직절편에서 단백질을 제거하였다. 실 온에서 5분 동안 2% H2O2/phosphate-buffered saline (PBS)에 처리하여 endogenous peroxidase를 불활성 화시키고 다시 PBS로 2번 씻어낸 후 두 방울의 1x equilibriation buffer를 조직에 떨어뜨렸다. Working- strength terminal deoxynucleotidyl transferase (TdT) 54 μl를 조직에 떨어뜨리고 한 시간 동안 37℃의 온 도로 유지시켰다. Stop/wash buffer를 추가하고 다시 30분 동안 37℃의 온도로 유지시켰다. 각 5분 동안 3번 PBS로 씻어내고 두 방울의 anti-digoxigenin- peroxidase를 떨어뜨린 후 30분 동안 실온에서 유지 시키고 PBS로 다시 3번 씻어낸 후 diaminobenzidine (DAB)으로 발색시켰다. 양성 대조로는 편도선의 조 직을 이용하였으며, 염색 과정 중 TdT를 빼고 염색 한 조직을 음성 대조로 삼았다. 대상 환자군을 모르 는 상태에서, 병리의사가 염색된 조직을 광학현미경 으로 관찰하여 위소와(foveolae)가 장축으로 보이는 부위에서 최소 500개 이상의 상피세포를 센 후 상피 세포 100개에 대한 아포토시스 양성 세포의 백분율 을 구하여 apoptosis index로 삼았다.
5. P CNA (pr olif er a t in g ce ll n uclea r a n - t ig e n ) 및 B cl- 2 면역조직화학염색검사 위상피세포의 증식을 알아보는 데는 titrated thy- midine, bromodeoxyuridine (BrdU), Ki-67 및 PCNA 등을 이용한 방법들이 있다. 이 중 PCNA는 G1, S 그리고 G2 세포주기에 만들어지며 S 주기에서 가장 많이 합성되는 36 KD의 핵단백으로 세포주기를 조 절하는 단백으로 알려져 있다.26 PCNA 면역조직화 학염색검사는 간단하고 재현성이 있으며, 세포 증식 측정의 표준 방법으로 인정되는 Vincristine meta- phase arrest 검사법으로, 측정한 위소와세포 생성률 과 잘 일치됨이 확인되었다.27 이러한 이유 등으로 현재 위상피세포의 증식을 측정하는 데 많이 사용되 는 방법 중 하나이다.7,27-29 PCNA 검사는 Biotiny- lated PCNA 단일 클론성 항체(Zymed laboratory inc, USA)를 이용하였으며 Biotinylated mouse anti- PCNA와 streptavidin-peroxidase로 처리한 후 DAB 로 발색하고 hematoxylin으로 대비염색을 하였다.
염색된 조직은 광학현미경으로 관찰하여 위소와가 장축으로 보이는 부위에서 최소 500개 이상의 상피 세포를 센 후 상피세포 100개에 대한 PCNA 양성 세 포의 백분율을 구하여 PCNA index로 삼았다. 양성 대조로는 Zymed사에서 제공된 PCNA 양성 대조 조 직절편을 이용하였으며, 일차항체 대신에 PBS로 대 치하여 염색한 것을 음성 대조로 삼았다. Bcl-2 검사 는 단일 클론성 mouse anti-human Bcl-2 oncoprotein 항체(Dako, Denmark)를 이용하였으며 AEC (3-amino- 9-ethylcarbazole) kit를 이용하여 발색시키고 광학현 미경을 이용하여 Bcl-2에 대한 발현의 유무를 확인 하였다. 양성 대조로는 편도선의 조직을 이용하였으 며 외투층(mantle zone)에서 강하게 염색되었고 배 중심(germinal center)에서는 대부분의 세포가 음성 이었다. 음성 대조는 동량의 일차항체에 대한 non- immune mouse IgG 혈청으로 처리한 후 염색이 되 지 않은 조직을 이용하였다. PCNA 및 Bcl-2 염색 후 양성 세포의 관찰은 대상 환자군을 모르는 상태 에서 병리의사가 시행하였다.
Bhang et al. Effects of Helicobacter pylori Infection on Apoptosis, Bcl-2 and Cell Proliferation 13
6. 통계 처리
통계 처리는 Window용 version 1.0 SigmaStat를 이용하였으며 실험에 따른 결과의 값은 평균±표준 편차로 표현하였다. H. pylori 감염 유무에 따른 apoptosis index 및 PCNA index의 비교는 독립인 표 본 T 검정을 이용하였고 H. pylori 박멸 전후의 비교 는 짝을 이룬 표본 T 검정으로 비교하였다. Apop- tosis index와 PCNA index와의 상관관계는 피어슨 상관계수(Pearson correlation coefficient)를 구하여 알아보았고 Bcl-2 단백 발현은 Fisher' s exact 검사로 비교하였다. 통계적인 유의성은 p값이 0.05 이하일 때로 하였다.
결 과
1. 대상군
총 47예를 대상으로 하였으며 H. pylori 음성인 환 자는 21예(남자 9예, 여자 12예, 평균 연령 38±10.4) 이고 H. pylori 양성인 환자는 26예(남자 10예, 여자 16예, 평균 연령 40.8±8.7)로 차이를 보이지 않았다.
2. H . p y lori 감염 유무에 따른 아포토시스, P CN A 및 B cl- 2 발현
Apoptosis index 및 PCNA index는 H. pylori 음성 인 환자(21예)에서 각각 1.69±0.99, 2.90±1.50이었 으며, H. pylori 양성인 환자(26예)에서는 각각 2.81
±1.19, 5.13±2.0으로 H. pylori 양성인 환자에서 유 의하게 높았다(p<0.01). Bcl-2 단백의 발현은 H.
pylori 음성인 환자에서 21예 중 2예(9.5%)였고, H.
pylori 양성인 환자에서 26예 중 3예(11.5%)로 차이
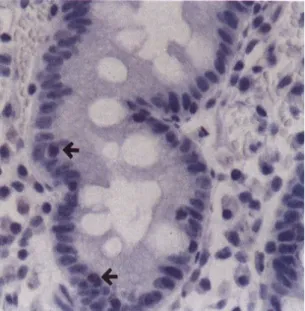
를 보이지 않았다(Table 1). H. pylori 음성인 환자에 서, 아포토시스 양성인 세포는 대부분 위소와의 표 면에서 관찰되었으며 증식구역(proliferating zone;
위선의 경부)에서 드물게 보였다. 반면에 PCNA 양 성 세포는 주로 증식구역에서 관찰되었다(Fig. 1).
H. pylori 양성 환자에서는 음성인 환자에 비해 상대 적으로 많은 수의 아포토시스 양성인 세포가 증식 구역에서 관찰되어 위소와의 아래쪽으로 이동하는 양상을 보였다. PCNA 양성인 세포는 H. pylori 음 성인 환자에 비해 상대적으로 표면에서 많이 관찰 되어 위소와의 표면으로 증식구역이 이동함을 알 수 있었다(Fig. 2). Bcl-2 단백의 발현은 H. pylori 감 염 유무에 관계없이 일부 환자에서만 핵 주위로 약 하게 나타났다(Fig. 3).
3. H . p y lori 박멸치료 전후의 아포토시스, P CN A 및 B cl- 2 발현
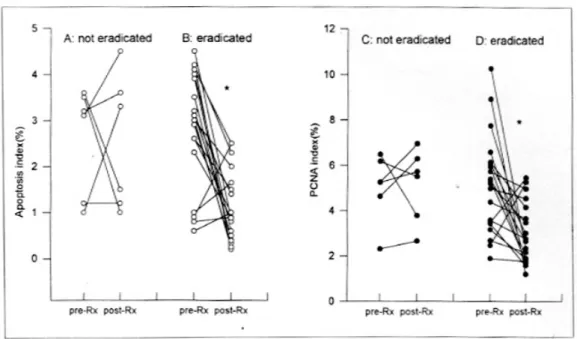
박멸치료에 실패했던 6예의 환자(2군)에서는 치 료 전의 apoptosis index 및 PCNA index는 치료 후 와 차이를 보이지 않았다(p=0.91, 0.85). 박멸치료에 성공하였던 20예의 환자(3군)에서는 치료 전의 apop- tosis index 및 PCNA index가 박멸된 후에 유의하게 감소하였다(p<0.01, Table 2, Fig. 4). 2군에서 Bcl-2 단백의 발현은 6예 중 치료 전후로 1예도 나타나지 않았으며(0%) 3군에서는 치료 전에 20예 중 3예 (15%)에서 발현되었고 치료 후에는 2예(10%)에서 발현되어 치료 전후로 차이를 보이지 않았다. 2군에 서는 치료 전에 아포토시스 양성인 세포가 증식구역 에서, PCNA 양성인 세포가 위소와의 표면쪽에서 다 수 관찰되었던 것이 치료 후에도 계속같은 양상을 보였다. 3군에서는 치료 전에 2군과 같은 양상을 보
Table 1. Apoptosis Index, PCNA Index and Bcl-2 Expression according to H. pylori Infection
H. pylori negative (n=21) H. pylori positive (n=26)
Apoptosis index PCNA index Bcl-2 expression
1.69±0.99 2.90±1.50 2 (9.5%)
2.81±1.19*
5.13±2.0*
3 (11.5%) Values of apoptosis index and PCNA index represent mean±SD.
* p<0.01 compared with H. pylori negative patients.
14 대한소화기학회지 : 제 34 권 제 1 호 1999
Fig. 1. Distribution of apoptosis and PCNA positive cells (arrows) in H. pylori negative patient. A, In situ apoptosis as detected by TUNEL (×100) showed a brown colored nucleus in the surface epithelium; B, Immunohistochemical staining for PCNA (×100) showed several brown colored nuclei mainly in the proliferative zone.
Fig. 2. Distribution of apoptosis (arrows) and PCNA positive cells in H. pylori positive patient. A, In situ apoptosis as detected by TUNEL (×200) showed that apoptotic cells were also seen in the deep portion of foveolae; B, Immunohistochemical staining for PCNA (×100) showed that many immunoreactivities were diffusely located in the whole foveolae.
방춘상 외 6인. Helicobacter pylori 감염이 아포토시스, Bcl-2 및 세포 증식에 미치는 영향 15
였다가 치료 후에는 아포토시스 양성인 세포는 대 부분 위소와의 표면에서 관찰되고 증식구역에서 드 물게 보였으며 PCNA 양성인 세포는 주로 증식구역 에서 관찰되었다. Bcl-2 단백의 발현은 2군과 3군의 일부 환자에서만 치료 전후에 핵 주위로 약하게 나 타났다.
4. Apopt os is index 와 P CNA in dex 와의 관계 Apoptosis index와 PCNA index는 뚜렷한 양적 상 관관계를 보여서(피어슨 상관계수 r=0.65, p<0.01) 아포토시스가 증가함에 따라 상피세포의 증식도 증 가됨을 알 수 있었다(Fig. 5).
고 찰
Programmed cell death라고 불리우는 아포토시스 는 여러 가지 형태학적, 생물학적, 분자유전학적으 로 특징적인 변화를 나타내는 세포 사망의 한 형태 이다.30,31 이러한 과정은 정상 조직의 교체(turnover) 시에 세포를 제거하는 소위 생리학적인 자살기전이 며,9,32 또한 DNA 손상시에 이를 제거함으로써 변이 된 DNA가 복제될 위험성을 없애주는 역할을 한 다.33 한편 아포토시스에 의한 세포 사망과 세포 증 식의 균형은 조직의 항상성을 유지하는 데 중요한 작용을 하는데, 이러한 균형이 깨지면서 다향한 형 태의 질병이 발생하게 된다.9 암 발생과 관련하여, 아포토시스는 단순히 세포의 소실만을 나타내는 것 이 아니라 세포 증식과도 밀접한 관계를 가지고 있 어서, 여러 가지 다양한 종류의 암이나11,12,34 전이된 대장암13 에서 동시에 증가되고 대장의 선종에서도 이형성의 정도가 심해짐에 따라 증가되는 것으로 보 고되고 있다.35 한편 H. pylori 감염은 위암 발생에 있어 중요한 역할을 하는 것으로 생각되고 있는데, 최근에 H. pylori 감염이 아포토시스를 유발시킬 수 있는 것으로 알려졌으며16,36,37 그 유발물질로는 산화 질소,38-40 암모니아,41 lipopolysaccharide,36 TNF-α, CD 95 (Fas) ligand,42 CagA 및 VacA 단백 등16이 제 시되고 있고, 항산화약제 투여로 감소된다고 하였 다.39 저자들도 H. pylori 양성이며 만성 위염을 가진 환자가 음성인 환자에 비해 아포토시스 및 세포 증 식이 증가되어 있음을 관찰하였다. 또한 H. pylori 양 성인 환자에서는 상대적으로 많은 수의 아포토시스 Fig. 3. Immunohistochemical staining for Bcl-2 (×200)
showed several perinuclear staining cells (arrowos) in the deep portion of foveolae.
Table 2. Apoptosis Index, PCNA Index and Bcl-2 Expression before and after Treatment of H. pylori
H. pylori not cleared (n=6) H. pylori cleared (n=20)
Before After Before After
Apoptosis index PCNA index Bcl-2 expression
2.60±1.18 5.02±1.49 0 (0%)
2.52±1.47 5.15±1.62 0 (0%)
2.88±1.21 5.17±2.16 3 (15%)
1.10±0.75*
2.94±1.32*
2 (10%) Values of apoptosis index and PCNA index represent mean±SD.
* p<0.01 compared with pre-treatment.
16 The Korean Journal of Gastroenterology : Vol. 34, No. 1, 1999
양성 세포가 위소와의 표면뿐 아니라 증식구역에서 나타나고, PCNA 양성인 세포는 증식구역 이외에 아포토시스가 일어나는 위소와의 표면에서도 관찰 되어, H. pylori 감염이 아포토시스와 세포 증식의 출현 및 분포에 중요한 영향을 미치고 있음을 알 수 있었다. H. pylori 감염시 위상피세포의 과증식은 세 포 손상에 의한 직접적인 결과로43 혹은 가스트린의 증가에 의한 반응27으로 보고되고 있고, 최근 아포토 시스의 증가에 따른 세포 손실을 상쇄하기 위해 나 타나는 것으로 제시되었다.16,42 본 연구에서 아포토 시스와 세포 증식과는 뚜렷한 양적 상관관계를 나 타내어 아포토시스의 증가와 세포 증식과는 밀접한 관계를 가지고 있을 것으로 생각된다. 과증식된 위 상피세포는 발암요인에 예민하게 반응하고44 돌연변 이가 일어날 기회가 많아지는데45 특히 위소와의 표 면에 위치한 증식세포는 발암물질에 예민하게 반응 한다.46 H. pylori의 감염에 의해 상피세포 및 DNA 가 손상되고 이를 제거하기 위해 아포토시스가 일 어나며, 이에 의한 세포 손실을 상쇄하기위해 또는 Fig. 4. The effect of H. pylori eradication on apoptosis and PCNA index. A, There was no significant difference before and after treatment in apoptosis index in patients who remained positive for H. pylori after treatment (p=0.91); B, Eradication of H. pylori caused a significant reduction in apoptosis index (*p<0.01); C, There was no significant difference before and after treatment in PCNA index in patients who remained positive for H.
pylori after treatment (p=0.85); D, Eradication of H. pylori caused a significant reduction in PCNA index (*p<0.01).
Fig. 5. Relationship between apoptosis index and PCNA index. There was a signficant correlation between both of them (r=0.65, p<0.01).
Bhang et al. Effects of Helicobacter pylori Infection on Apoptosis, Bcl-2 and Cell Proliferation 17
직접적인 세포 손상의 결과로 상피세포의 과증식이 일어남에 따라 위암 발생의 위험이 증가될 수 있을 것이다.
한편 아포토시스는 p53, bcl-2, c-myc, ras, c-fos 등의 다양한 종류의 암유전자와 종양억제유전자에 의해 조절되는데47 주로 p53과 bcl-2에 대한 연구가 많이 이루어졌다. 암유전자인 bcl-2는 아포토시스를 억제하여 세포 사망을 막는 역할을 하는데 정상적으 로 위장관에서의 분포는 모세포(stem cell)와 증식구 역에 국한되어 나타나며, 세포가 분화되고 아포토시 스가 일어나는 점막의 표면에서는 bcl-2의 발현은 없어진다. 이러한 분포는 증식세포의 생존을 증가시 키고 완전히 분화된 세포는 아포토시스에 의해 제거 될 수 있도록 하여 준다.48 이러한 bcl-2 유전자의 과 발현이 림프종에서 발견된 후49 여러 가지 비혈액암 에서도 관찰되었다.50-52 Korsmeyer17는 여포성 림프 종의 발생 과정 중 bcl-2의 이상 발현에 의한 아포토 시스의 억제가 세포 성장을 촉진하게 되고, 생존이 연장됨에 따라 이차적인 유전자의 이상을 유도하여 악성으로 변화될 수 있을 것이라고 설명하였다. 최 근 Bcl-2의 이상 발현은 대장암의 전구병소인 선종53 과 위암의 전구병소인 장상피화생이나 이형성에서 도54,55 관찰되었으며 증식구역 외의 지역에도 전체 적으로 분포되었다. 저자들이 관찰한 바에 의하면 H. pylori에 감염된 만성 위염을 가진 환자에서는 아 포토시스 및 상피세포의 증식이 일어났으나 Bcl-2의 이상 발현은 보이지 않았다. 그러나 계속되는 상피 세포의 과증식에 의한 미성숙 세포의 생성이 유도되 고 장상피화생/이형성으로 진행됨에 따라 bcl-2의 이 상발현 및 p53의 변이가 일어나게 되면, 아포토시스 가 억제됨으로써 손상된 DNA를 가진 세포가 제거 되지 않고 생존하여 암 발생에 관여하는 다른 이차 적인 변화를 획득할 수 있을 것으로 생각된다.
한편 cagA 양성인 균주는 위암 발생과 밀접한 관 계가 있다고 알려져 있으며,56,57 최근에 이에 따른 아포토시스와 위상피세포의 증식에 관한 연구가 이 루어지고 있다. 한 보고58에서 CagA 단백 양성인 균 주에 감염된 환자에서 상피세포의 과증식은 있으나 상대적으로 아포토시스의 증가는 없음을 관찰하였 고, 이로 인해 제거되지 않는 돌연변이 세포가 축적
되어 위암 발생의 위험이 증가될 것이라 하였다. 그 러나 cagA 유전자의 유무와 관계없이 H. pylori에 감염되었을 때 상피세포의 증식과 아포토시스가 모 두 증가된다는 보고59,60도 있어 아직 이에 대한 연구 가 더 필요할 것으로 생각된다.
H. pylori 감염은 그 자체만으로 직접 위암을 발생 시키기보다는 위축성 위염 등을 일으키는 간접적인 방법으로 위암 발생에 관여할 것으로 생각된다.61 만 성 위염 및 장상피화생 등은 암성 변화를 일으키기 적당한 조건, 즉 위산 분비 및 위액 내 비타민 C 농 도의 감소, N-nitroso 화합물의 증가, 위상피세포의 과증식 등을 제공한다.62 비록 H. pylori에 대한 균 박멸이 위암의 전구병변인 위축성 위염 및 장상피화 생을 개선시키지는 못하지만63,64 위암 발생기전으로 생각되는 상기의 조건들을 개선시키는 것으로 알려 져 있다.2-6,8 또한 본 연구에서 보면 아직 Bcl-2의 이 상 발현이 나타나지 않은 만성 위염에서 균 박멸치 료로 상피세포의 증식과 관련된 아포토시스의 증가 와 분포를 정상적인 모양으로 환원시킬 수 있었다.
요 약
목적: Helicobacter pylori는 위상피세포의 증식을 증가시킴으로써 위암 발생을 유발시킬 수 있다. Pro- grammed cell death (apoptosis; 아포토시스)는 세포 증식과 관련되며 bcl-2 암유전자는 아포토시스를 억 제시킨다. 이 연구의 목적은 만성 위염에서 H. pylori 감염이 아포토시스, Bcl-2 그리고 위상피세포의 증 식에 미치는 영향을 알아보기 위함이다. 대상 및 방 법: 저자들은 in situ TdT-mediated dUTP nick end labeling 방법으로 아포토시스를 검사하였으며 PCNA 와 Bcl-2에 대한 면역조직화학적 염색을 시행하였 다. 결과: H. pylori 양성인 환자(2.81±1.19, 5.13±
2.0)는 음성인 환자(1.10±0.75, 2.94±1.32)에 비해 아포토시스 및 PCNA index가 의미 있게 높게 나타 났으며 H. pylori 감염에 대한 성공적인 박멸치료가 되었던 환자에서는 아포토시스와 상피세포의 증식 이 의미 있게 감소되었다(1.10.±0.75, 2.94±1.32).
또한 apoptosis index는 PCNA index와 유의한 상관 관계를 보였다. Bcl-2의 발현은 H. pylori 양성인 환
18 대한소화기학회지 : 제 34 권 제 1 호 1999
자와 음성인 환자 사이에 차이를 보이지 않았다. 결 론: H. pylori의 감염은 아포토시스과 위상피세포의 과증식을 유발시킬 수 있으며 이러한 변화는 H.
pylori에 대한 박멸치료로 감소되었다.
색인단어: H. pylori, 아포토시스, PCNA, Bcl-2, 위암
참 고 문 헌
1. International Agency for Research on Cancer. World Health Organization. Schistosomes, liver flukes and Helicobacter pylori. IARC Monogr Eval Carcinog Risks Hum 1994;61:218-220.
2. Sobala GM, Schorah CJ, Shires S, et al. Effect o eradication of Helicobacter pylori on gastric juice ascorbic acid concentrations. Gut 1993;34:1038- 1041.
3. Ruiz B, Rood JC, Fontham ETH, et al. Vitamin C concentration in gastric juice before and after anti-Helicobacter pylori treatment. Am J Gatroen terol 1994;88:533-539.
4. Rokkas T, Papatheodorou G, Karameris A, Mavro georgis A, Kalogeropoulos N, Giannikos N. Helico bacter pylori infection and gastric juice vitamin C levels. Impact of eradication. Dig Dis Sci 1995;40 615-621.
5. 방춘상, 김진일, 정인식, 장은덕. Helicobacter pylori 감염과 위액내 비타민 C 농도와의 관계. 대한소화기 학회지 1997;30:18-29.
6. Cahill RJ, Xia H, Gallen CK, Beattie S, Hamilton H, O' Morain C. Effect of eradication of Helico bacter pylori infection on gastric epithelial cel proliferation. Dig Dis Sci 1995;40:1627-1631.
7. Panella C, Ierardi E, Polimeno L, et al. Proliferative activity of gastric epithelium in progressive stage o Helicobacter pylori infection. Dig Dis Sci 1996;41 1132-1138.
8. Cahill RJ, Kilgallen C, Beattie S, Hamilton H O' Morain C. Gastric epithelial cell kinetics in the progression from normal mucosa to gastric carci noma. Gut 1996;38:177-181.
9. Thompson CB. Apoptosis in the pathogenesis and
treatment of disease. Science 1995;267:1456-1462.
10. Leoncini L, Vecchino MT, Megha T, et al. Correla- tion between apoptosis and proliferative indices in malignant non-Hodgkin' s lymphomas. Am J Pathol 1993;142:755-763.
11. Aihara M, Truong LD, Dunn JK, Wheeler TM Scardino PT, Thompson TC. Frequency of apoptotic bodies positively correlates with Gleason grade in prostate cancer. Hum Pathol 1994;25:797-801.
12. Gaffney EF. The extent of apoptosis in differen types of high grade prostatic carcinoma. Histopa thology 1994;25:269-273.
13. Tatebe S, Ishida M, Kasagi N, Tsujitani S, Kaibara N, Ito H. Apoptosis occurs more frequently in metastatic foci than in primary lesions of human colorectal carcinoma: analysis by terminal deoxynu cleotidyl-transferase-mediated dUTP-biotin nick end labeling. Int J Cancer 1996;65:173-177.
14. Hall PA, Coates PJ, Ansari A, Hopwood D. Regula tion of cell number in the mammalian gastroin testinal tract: the importance of apoptosis. J Cell Sc 1994;107:3569-3577.
15. Robert ME, Weinstein WM. Helicobacter pylori- associated gastric pathology. Gastroenterol Clin North Am 1993;22:59-72.
16. Moss SF, Calam J, Agarwal B, Wang S, Holt PR Induction of gastric epithelial apoptosis by Helico bacter pylori. Gut 1996;38:498-501.
17. Korsmeyer SJ. Bcl-2 initiates a new category o oncogenes: regulators of cell death. Blood 1992;80 879-886.
18. Oren M. The involvement of oncogenes and tumo supressor genes in the control of apoptosis. Cance Metastasis Rev 1992;11:141-148.
19. Correa P. A human model of gastric carcinogenesis Cancer Res 1998;48:3554-3560.
20. Sipponen P, Kekki M, Siurala M. Age-related trend of gastritis and intestinal metaplasia in gastric carcinoma patients and in controls representing the population at large. Br J Cancer 1984;49:521-530.
21. Sipponen P, Kekki M, Haapakoski J, Ihamäki T Siurala M. Gastric cancer risk in chronic atrophic
방춘상 외 6인. Helicobacter pylori 감염이 아포토시스, Bcl-2 및 세포 증식에 미치는 영향 19
gastritis: statistical calculations of cross-sectional data. Int J Cancer 1985;35:173-177.
22. Jass JR, Filipe MI. A variant of intestinal metaplasia associated with gastric carcinoma: a histochemical study. Histopathology 1979;3:191-199.
23. Jass JR. Role of intestinal metaplasia in the histogenesis of gastric carcinoma. J Clin Patho 1980;33:801-810.
24. Correa P, Haenszel W, Cuello, et al. Gastric precan cerous process in a high risk population: cohor follow-up. Cancer Res 1990;50:4737-4740.
25. Rokkas T, Filipe MI, Sladen GE. Detection of an increased incidence of early gastric cancer in pati ents with intestinal metaplasia type III who followed up. Gut 1991;31:1110-1113.
26. Waseem NH, Lane DP. Monoclonal antibody analy sis of proliferating cell nuclear antigen (PCNA) Structural conservation and detection of a nuclear form. J Cell Sci 1990;96:1221-1229.
27. Gray MR, Darnton SJ, Hunt JA, Irlam RW, Nemeth J, Wallace HM. Accelerated gastric epithelial proli feration. Gut 1995;36:522-527.
28. Hibi K, Mitomi H, Koizumi W, Tanabe S, Saigenj K, Okayasu I. Enhanced cellular proliferation and p53 accmulation in gastric mucosa chronically infected with Helicobacter pylori. Am J Clin Patho 1997;108:26-34.
29. Abe S, Sasano H, Katoh K, et al. Immunohistoche mical studies on ECF family growth factors in normal and ulcerated human gastric mucosa. Dig Dis Sci 1997;42:1199-1209.
30. Stewart BW. Mechanisms of apoptosis: integration of genetic, biochemical, and cellular indicators. J Natl Cancer Inst 1994;86:1286-1296.
31. Hockenbery D. Defining apoptosis. Am J Patho 1995;146:16-19.
32. Que FG, Gores GJ. Cell death by apoptosis: basic concepts and disease relevance for the gastroentero logist. Gastroenterology 1996;110:1238-1243.
33. Correa P, Miller MJS. Helicobacter pylori and gastric atrophy-cancer paradoxes. J Natl Cancer Ins 1995;87:1731-1732.
34. Allan DJ, Howell A, Roberts SA, et al. Reduction in apoptosis relative to mitosis in histologically normal epithelium accompanies fibrocystic change and carcinoma of the premenopausal human breast. J Pathol 1992;167:25-32.
35. Arai T, Kino I. Role of apoptosis in modulation o the growth of human colorectal tubular and villous adenomas. J Pathol 1995;176:37-44.
36. Piotrowski J, Piotrowski E, Skrodzka D, Slimiany A Slomiany BL. Induction of acute gastritis and epithelial apoptosis by Helicobacter pylori lipopoly saccharide. Scand J Gastroenterol 1997;32:203-211.
37. Hahm KB, Lee KJ, Choi SY, et al. Possibility o chemoprevention by the eradication of Helicobacter pylori: oxidative DNA damage and apoptosis in H pylori infection. Am J Gastroenterol 1997;92:1853- 1857.
38. Sandoval M, Liu X, Oliver PD, Zhang XJ, Clark DA, Miller MJ. Nitric oxide induces apoptosis in a human colonic epithelial cell line, T84. Med Inflammation 1995;4:248-250.
39. Bravo LE, Mannick EE, Zhang XJ, Ruiz B, Correa P, Miller MJ. H. pylori infection is associated with inducible nitric oxide synthase expression, nitroty rosine and DNA damage. Gastroenterology 1995;
108:A63.
40. Mannick EE, Bravo LE, Zarama G, et al. Inducible nitric oxide synthase, nitrotyrosinem and apoptosis in Helicobacter pylori gastritis: effect of antibiotics and antioxidants. Cancer Res 1996;56:3238-3243.
41. Tsuji S, Kawano S, Takei Y, et al. Ammonia induces gastric cell apoptosis: possible implication to Helicobacter-related gastric mucosal atrophy. Gas troenterology 1995;108:A244.
42. Wagner S, Beil W, Westermann J, et al. Regulation of gastric epithelial cell growth by Helicobacter pylori: evidence for a major role of apoptosis Gastroenterology 1997;113:1836-1847.
43. Tsuji MS, Kawano S, Tsuji T, et al. Cell kinetics o mucosal atrophy in rat stomach induced by long-term administration of ammonia. Gastroentero logy 1993;104:796-801.
20 The Korean Journal of Gastroenterology : Vol. 34, No. 1, 1999
44. Ames BN, Gold LS. Too many rodent carcinogens:
mitogenesis increases mutagenesis. Science 1990;
249:970-971.
45. Blaser MJ, Parsonnet J. Parasitism by the "slow"
bacterium Helicobacter pylori leads to altered gastric homeostasis and neoplasia. J Clin Invest 1994;94: 4-8.
46. Sørbye H, Kvinnsland S, Svanes K. Effect of salt induced mucosal damage and healing on penetration of N-methyl-N-nitrosoguanidine to proliferative cells in the gastric mucosa of rats. Carcinogenesis 1994;
15:673-679.
47. Kerr JF, Winterford CM, Harmon BV. Apoptosis. Its significance in cancer and cancer therapy. Cancer 1994;73:2013-2026.
48. Lebrun DP, Warnke RA, Cleary ML. Expression of Bcl-2 in fatal tissues suggests a role in morpho- genesis. Am J Pathol 1993;142:743-753.
49. Tsujimoto Y, Finger LR, Yunis J, Nowell PC, Croce CM. Cloning of the chromosome breakpoint of neoplastic B cells with the t (14;18) chromosome translocation. Science 1984;226:1097-1099.
50. McDonnell TJ, Troncoso P, Brisbay SM, et al. Ex- pression of the protooncogene bcl-2 in the prostate and its associaton with emergence of androgen- independent prostate cancer. Cancer Res 1992;52:
6940-6944.
51. Pezzella F, Turley H, Kuzu I, et al. Bcl-2 protein in non-small cell lung carcinoma. N Engl J Med 1993;329:690-694.
52. Pilotti S, Collini P, Rilke F, Cattoretti G, Bo RD, Pierotti MA. Bcl-2 protein expression in carcinomas originating from the follicular epithelium of the thyroid gland. J Pathol 1994;172:337-342.
53. Bedi A, Pasricha PJ, Akhtar AJ, et al. Inhibition of apoptosis during development of colorectal cancer.
Cancer Res 1995;55:1811-1816.
54. Lauwers GY, Scott GV, Hendricks J. Immunohisto- chemical evidence of aberrant Bcl-2 protein expression in gastric epithelial dysplasia. Cancer
1994;73:2900-2904.
55. Saegusa M, Takano Y, Okayasu I. Bcl-2 expression and its association with cell kinetics in human gastric carcinomas and intestinal metaplasia. J Cancer Res Clin Oncol 1995;121:357-363.
56. Blaser MJ, Perez-Perez GI, Kleanthous H, et al.
Infection with Helicobacter pylori strains possessing cagA associated with an increased risk of developing adenocarcinoma of the stomach. Cancer Res 1995;
55:2111-2115.
57. Crabtree JE, Wyatt JI, Sobala GM, et al. Systemic and mucosal humoral responses to Helicobacter pylori in gastric cancer. Gut 1993;34:1339-1343.
58. Peek RM, Moss SF, Tham KT, et al. Helicobacter pylori cagA+ strains and dissociation of gastric epithelial cell proliferation from apoptosis. J Natl Cancer Inst 1997;89:863-868.
59. Abdalla AM, Krivosheyev V, Hanzely Z, et al. Increased epithelial cell turnover in antrum and corpus of H.
pylori-infected stomach, irrespective of cagA status.
Gastroenterology 1998;114(suppl);A50.
60. Wagner S, Wingbermühle D, Beil W, et al. Significance of H. pylori cagA and vagA genotypes on apoptosis of gastric epithelial cells. Gastroenterology 1998;114(suppl):A326.
61. Watanabe Y, Kurata JH, Mizuno S, et al. Helicobacter pylori infection and gastric cancer. A nested case-control study in a rural area of Japan. Dig Dis Sci 1997;42:1383-1387.
62. Asaka M, Takeda H, Sugiyama T, Kato M. What role does Helicobacter pylori play in gastric cancer?
Gastroenterology 1997;113(6 suppl):S56-S60.
63. van der Hulst RW, van der Ende A, Dekker FW, et al.
Effect of Helicobacter pylori eradication on gastritis in relation to cagA; A prospective 1-year follow-up study.
Gatroenterology 1997;113:25-30.
64. El-Omar EM, Oien K, El-Nujumi A, et al. Helicobacter pylori infection and chronic gastric acid hyposecretion.
Gatroenterology 1997;113:15-24.