ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Correspondence to: Chang Hyeong Lee, M.D.
Department of Internal Medicine, Daegu Catholic Medical Center, 3056-6 Daemyeong-4 dong, Nam-gu, Daegu 705-718 Korea
Tel: +82-53-650-4043, 4050, Fax: +82-53-622-2072 E-mail: [email protected]
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 접수: 2005년 3월 18일, 승인: 2005년 9월 8일
연락처: 이창형, 705-718, 대구광역시 남구 대명 4동 3056-6번지 대구가톨릭대학교 의과대학 내과학교실
Tel: (053) 650-4043, 4050, Fax: (053) 622-2072 E-mail: [email protected]
* 이 연구는 2001년도 대구가톨릭대학교 의과학연구소 연구 비 지원으로 이루어졌음.
위선종 및 위선암 주변점막의 조직 변화와 세포자멸사 및 세포증식 발현율
대구가톨릭대학교 의과대학 내과학교실, 해부병리학교실*, 의학통계학교실†
정진태ㆍ이창형ㆍ유성수ㆍ하형근ㆍ배종석ㆍ권중구ㆍ김은영ㆍ김호각ㆍ조창호*ㆍ신임희
†Grading of Histology, Expression of Apoptosis and Cell Proliferation in Gastric Mucosa Adjacent to Gastric Adenoma or Adenocarcinoma
Jin Tae Jung, M.D., Chang Hyeong Lee, M.D., Sung Soo You, M.D., Hyung Keun Ha, M.D., Jong Seok Bae, M.D., Joong Goo Kwon, M.D., Eun Young Kim, M.D.,
Ho Gak Kim, M.D., Chang Ho Cho, M.D.*, and Im Hee Shin, M.D.†
Departments of Internal Medicine, Pathology*, and Biomedical Statistics†, Catholic University of Daegu School of Medicine, Daegu, Korea
Background/Aims: Helicobacter pylori (H. pylori) infection can lead to gastric adenoma and carcinoma through atrophic gastritis and intestinal metaplasia. Imbalance between apoptosis and proliferation may play a role in gastric carcinogenesis. We tried to investigate H. pylori infection rate, grade of gastritis, environmental risk fac- tors, expression rate of apoptosis and cell proliferation in mucosa adjacent to tumor, and we also tried to find significant factors associated with gastric carcinogenesis. Methods: Endoscopically diagnosed twenty cases of intestinal type gastric carcinoma, 20 cases of gastric adenoma, and 40 cases of control (normal or gastritis) were enrolled. H. pylori infection rate, histologic grading, apoptosis and immunohistochemical stain (Ki-67 and p53) to check mucosal proliferation were done in endoscopically biopsied tissues at antrum and body at least 2 cm apart from adenoma or carcinoma. Results: In three groups, H. pylori infection rates were not significantly different. In the multivariate analysis, only atrophy of gland was a significant risk factor for adenoma compared to control group (OR 3.7). Intestinal metaplasia in antrum and alcohol drinking were significant risk factors for carcinoma compared to control group (OR 4.4 and 4.9 respectively). Expressions of apoptosis, Ki-67 and p53 were not significantly different in three groups. Conclusions: Intestinal metaplasia in antrum and alcohol drinking are significant risk factors for gastric carcinoma. Degree of mucosal proliferation and apoptosis in gastric mucosa adjacent to tumor are not significantly different in three groups. (Korean J Gastroenterol 2005;46:269-275)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Helicobacter pylori; Gastric adenoma; Gastric carcinoma; Carcinogenesis; Apoptosis
270 대한소화기학회지: 제46권 제4호, 2005
서 론
대부분 상피세포암과 마찬가지로 위암 발병에도 여러 가 지 인자와 단계가 관련한다. Helicobacter pylori (H. pylori) 감염으로 위점막 손상이 생기고 위축성 위염과 장상피화생 을 거쳐서 위선종을 유발하고 장형(intestinal type)선암이 유 발된다.1-5 그러나 H. pylori 감염과 위암 발생은 관련이 없다 는 견해도 있다.6,7
정상 위점막은 세포자멸사에 의한 세포손실과 세포증식 으로 동적인 균형을 이루는데 H. pylori 감염에 의한 위십이 지장 질환에서는 세포자멸사 및 세포증식이 증가한다.8,9 이 때 H. pylori 박멸치료를 하면 증가된 세포자멸사와 세포증 식이 감소한다.10
위암환자의 주변점막에서 심한 위축성 위염이 관찰되는 데 위암 또는 위선종조직은 정상 점막보다 세포자멸사와 세 포증식이 증가한 경우는 많으나11-13 종양의 주변점막에서 세포자멸사와 세포증식의 변화 정도에 대해서 연구한 경우 는 드물다.
이에 저자들은 장형선암, 위선종, 대조군에서 종양 주변 점막에서 H. pylori 감염률, 위염의 조직소견, 여러 환경 요 인의 차이를 조사하였으며 이를 대상으로 위선종과 장형선 암군의 유의한 위험인자를 알아보았고 동시에 종양의 주변 점막에서 세포자멸사 및 세포증식에 관여하는 단백질의 발 현 양상을 비교 분석하였다.
대상 및 방법
1. 대상
1998년 9월부터 2001년 11월까지 대구가톨릭대학병원에 서 위내시경 생검을 통해 위선암으로 진단된 예 중 Lauren 분류법14에 따라 장형선암 20예, Goldstein과 Lewin등15이 제 안한 이분법에 따라 저도 형성이상 선종 20예, 그리고 대조 군으로 정상 및 경미한 만성위염을 보이는 40예를 대상으로 하였다. 선암과 선종의 경우 병변에서 2 cm 이상 떨어진 부 위의 전정부와 체부에서 채취한 조직을 대상으로 위염의 조 직소견 및 CLO (CLOTM, Delta-West, Australia) 검사를 시행 하였다.
음주력, 흡연력 및 위암의 가족력에 대한 설문조사도 함 께 시행하였으며 혈청 H. pylori 항체(GenediaTM, 녹십자, 한 국)를 조사하였다. 음주력은 주 3회 음주를 기준으로 2단계 로 구분하였고, 흡연력은 갑년으로 표시하였으며, 혈청 H.
pylori 항체는 역가가 16 RU/mL 이상을 양성으로 하였다.
2. 방법
1) 조직 검사
내시경 생검 조직을 10% 중성 포르말린용액에 고정한 후 계열 에탄올로 탈수하여 파라핀에 포매하였다. 파라핀에 포 매된 조직을 4μm 두께 절편으로 만들어 슬라이드에 부착 시킨 후 일반 광학현미경으로 조직 진단을 확인하였다. 위 전정부와 체부에서 만성 염증, 선 위축, 장상피화생, 염증의 활동도 및 H. pylori 집락의 밀도를 Updated Sydney system에 따라 기술하였다.16
2) 면역조직화학 염색
파라핀에 포매된 조직을 4μm 두께 절편으로 만들어 생 리식염수로 처리된 유리슬라이드에 부착시키고 60oC에서 4 시간 동안 방치하였다. 이어 탈파라핀과 함수과정을 거친 다음 항원 노출을 좋게 하기 위하여 citric acid 용액에 담근 다음 microwave를 이용하여 10분간 처리하는 과정을 3회 반 복하고 30분간 실온에 방치하였다. 내인 과산화효소를 억제 하기 위하여 3% 과산화수소수로 5분간 처리한 후 증류수로 세척하였다. 비특이 단백 결합을 방지하기 위하여 5% 양혈 청에 20분 동안 실온에서 방치하였다. 일차항체는 Ki-67 항 원 단클론 항체인 MIB-1 (Immunotech, Fullerton, CA, USA, 1:50)과 p53 (Novocastra, Newcastle, UK, 1:100)을 각각 1시간 및 2시간씩 실온에서 반응시킨 다음, tris 용액으로 5분씩 2 회 세척하였고, 이차항체로 biotin이 결합된 goat anti-rabbit IgG (DAKO, Copenhagen, Denmark)와 20분 동안 반응시켰 다. 이어 diaminobenzidine에 2분 동안 발색을 거쳐 슬라이드 를 Mayer’s hematoxylin으로 10초 동안 대조 염색하여 봉입 하였다. 음성 대조군으로는 일차항체 대신 정상 양혈청을 사용하였다.
Ki-67에 대한 면역조직화학 염색의 해석은 400배의 고배 율 시야 3군데를 검색하여 핵이 양성인 세포 수를 세어 판 정하였고, p53은 400배의 고배율 시야 3군데를 검색하여 핵 에 양성으로 표지된 세포 수가 전체 세포수의 10%를 넘으 면 양성으로 판정하였다.
3) TUNEL을 이용한 세포자멸사 관찰과 판독
TdT-mediated dUTP-biotin nick end labelling (TUNEL)을 시 행하기 위하여 파라핀에 포매된 조직을 4μm 두께 절편으로 만들어 탈파라핀과 함수과정을 거친 다음 proteinase K (20 g/mL)로 37oC에서 25분간 처리한 후 증류수로 수세하였고 실온에서 2% 과산화수소수로 내인 과산화효소의 작용을 차 단하였다. ApopTag Plus Peroxidase kit (Chemicon, Hampshire, UK)를 이용하여 세포자멸사를 일으킨 세포를 표지하였다.
방법은 terminal deoxynucleotidyl transferase (TdT)와 dATP가
섞인 반응액을 도포하여 37oC에서 30분간 반응시켜, TdT를 이용하여 절단된 DNA의 3'-OH 끝에 digoxigenin이 표지된 dUTP를 결합한 후 anti-digoxigenin-peroxidase와 상온에서 30 분간 반응시켰다. 그리고 3,3-diaminobenzidine으로 2분간 발 색시킨 다음 Mayer's hematoxylin으로 대조염색을 하였다.
판독은 400배의 고배율 시야 3군데를 검색하여 핵이 양성으 로 염색된 세포 수를 세어 판정하였다.
4) 통계 분석
모든 통계 분석은 SPSS Windows 11.0을 이용하였고 연속 변수의 값은 평균±표준편차로 표기하였다. 각 군의 비교에 서 연속변수는 ANOVA 검정을, 범주형 변수는 Chi-square 검정을 이용하였고, 여기에서 유의한 변수만을 대상으로 다 항 로지스틱 회귀분석을 실시하여 교차비(odds ratio, OR) 및 95% 신뢰구간을 구하였다. p값이 0.05보다 작은 경우에 유 의한 것으로 판정하였다.
결 과
1. 임상 특징
환자의 평균연령은 위선종군 58.4세(36-84세), 장형선암군 59.8세(39-77세), 대조군 55.2세(21-84세)로 유의한 차이가 없 었으며, 남자 비율은 위선종군 55% (11/20명), 장형선암군 65% (13/20명), 대조군 40% (16/40명)로 유의한 차이가 없었 다.
2. H. pylori 양성률
CLO검사의 양성률은 위선종군 75% (15/20명), 장형선암군 65% (13/20명), 대조군 65% (26/40명)로 유의한 차이가 없었
다. H. pylori 항체 양성률은 위선종군 70.6% (12/17명), 장형 선암군 66.7% (8/12명), 대조군 72.7% (24/33명)로 유의한 차 이가 없었다.
3. 환경 요인
주 3회 이상의 음주력은 위선종군 및 장형선암군이 대조 군에 비해서 유의하게 높았으며(p=0.021), 흡연력도 위선종 군 및 장형선암군이 대조군에 비해 유의하게 높았다(p=
0.002). 위암 가족력은 각 군에서 유의한 차이가 없었다 (Table 1).
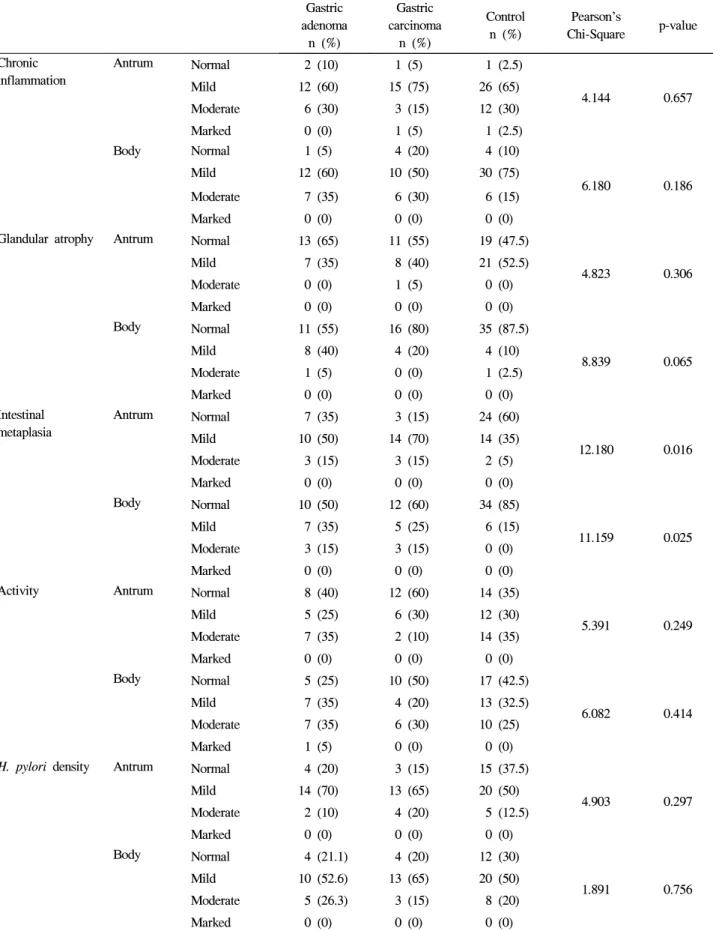
4. 위점막 조직 소견
Updated Sydney system에 따른 위 전정부와 체부에서 만 성 염증, 선위축, 염증의 활동도 및 H. pylori 집락의 밀도 정 도는 각 군에서 차이가 없었으며 장상피화생의 경우는 위선 종군 및 장형선암군이 대조군에 비해 전정부(p=0.016) 및 체 부(p=0.025)에서 유의하게 높았다(Table 2).
5. 주변점막의 면역조직화학 염색
종양의 주변점막에서 세포자멸사와 세포 증식에 관련된 단백질 발현을 관찰한 결과 세포자멸사는 위선종군 12.4±
7.5, 장형선암군 16.7±13.3, 대조군 16.7±10.1로 유의한 차 이가 없었고(p=0.308), Ki-67 발현율은 위선종군 24.3±14.6, 장형선암군 30.3±14.2, 대조군 34.6±17.6으로 유의한 차이 가 없었으며(p=0.068), p53 발현율도 위선종군 50.0%, 장형선 암군 65.0%, 대조군 65.8%로 유의한 차이가 없었다(p=0.469).
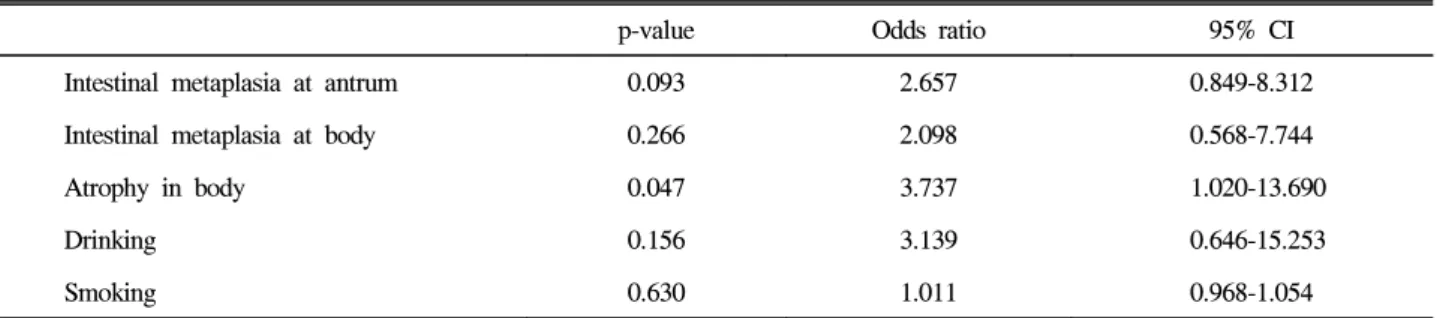
6. 종양발생에 관여하는 위험인자 분석
대조군에 비해서 위선종과 장형선암의 발생에 유의한 인 자는 전정부 및 체부의 장상피화생과 체부의 선위축, 음
Table 1. Analysis of Environmental Risk Factors for Gastric Adenoma and Carcinoma Gastric
adenoma n (%)
Gastric carcinoma
n (%)
Control n (%)
Pearson's
Chi-Square p-value
Alcohol drinking
<3 times/week 11 (55) 8 (42.1) 31 (77.5)
7.738 0.021
≥3 times/week 9 (45) 11 (57.9) 9 (22.5) Family history of gastric cancer
Absent 15 (75) 14 (70) 32 (80)
0.759 0.684
Present 5 (25) 6 (30) 8 (20)
Smoking (pack-years, mean±SD) 16.3±16.4 24.3±24.2 6.9±14.2 0.002*
* ANOVA test.
272 대한소화기학회지: 제46권 제4호, 2005
Table 2. Histological Differences between Antrum and Body in Three Groups according to the Updated Sydney System Gastric
adenoma n (%)
Gastric carcinoma
n (%)
Control n (%)
Pearson's
Chi-Square p-value Chronic
inflammation
Antrum Normal 2 (10) 1 (5) 1 (2.5)
4.144 0.657 Mild 12 (60) 15 (75) 26 (65)
Moderate 6 (30) 3 (15) 12 (30) Marked 0 (0) 1 (5) 1 (2.5) Body Normal 1 (5) 4 (20) 4 (10)
6.180 0.186 Mild 12 (60) 10 (50) 30 (75)
Moderate 7 (35) 6 (30) 6 (15) Marked 0 (0) 0 (0) 0 (0) Glandular atrophy Antrum Normal 13 (65) 11 (55) 19 (47.5)
4.823 0.306 Mild 7 (35) 8 (40) 21 (52.5)
Moderate 0 (0) 1 (5) 0 (0) Marked 0 (0) 0 (0) 0 (0) Body Normal 11 (55) 16 (80) 35 (87.5)
8.839 0.065 Mild 8 (40) 4 (20) 4 (10)
Moderate 1 (5) 0 (0) 1 (2.5) Marked 0 (0) 0 (0) 0 (0) Intestinal
metaplasia
Antrum Normal 7 (35) 3 (15) 24 (60)
12.180 0.016 Mild 10 (50) 14 (70) 14 (35)
Moderate 3 (15) 3 (15) 2 (5) Marked 0 (0) 0 (0) 0 (0) Body Normal 10 (50) 12 (60) 34 (85)
11.159 0.025 Mild 7 (35) 5 (25) 6 (15)
Moderate 3 (15) 3 (15) 0 (0) Marked 0 (0) 0 (0) 0 (0) Activity Antrum Normal 8 (40) 12 (60) 14 (35)
5.391 0.249 Mild 5 (25) 6 (30) 12 (30)
Moderate 7 (35) 2 (10) 14 (35) Marked 0 (0) 0 (0) 0 (0) Body Normal 5 (25) 10 (50) 17 (42.5)
6.082 0.414 Mild 7 (35) 4 (20) 13 (32.5)
Moderate 7 (35) 6 (30) 10 (25) Marked 1 (5) 0 (0) 0 (0) H. pylori density Antrum Normal 4 (20) 3 (15) 15 (37.5)
4.903 0.297 Mild 14 (70) 13 (65) 20 (50)
Moderate 2 (10) 4 (20) 5 (12.5) Marked 0 (0) 0 (0) 0 (0) Body Normal 4 (21.1) 4 (20) 12 (30)
1.891 0.756 Mild 10 (52.6) 13 (65) 20 (50)
Moderate 5 (26.3) 3 (15) 8 (20) Marked 0 (0) 0 (0) 0 (0)
주력, 흡연력이었으며, 이들 유의한 변수를 대상으로 다항 로지스틱 회귀분석을 실시한 결과, 위선종군은 체부 선위축 (OR=3.7, 95% CI=1.0-13.7)이, 장형선암군은 전정부 장상피 화생(OR=4.4, 95% CI=1.4-13.4) 및 음주력(OR=4.9, 95% CI=
1.1-22.6)이 유의한 인자였다(Table 3, 4).
고 찰
H. pylori 감염은 만성 위염, 장상피화생, 위궤양 및 위암 을 일으키는 중요한 원인이다.17,18 특히 위암 발생에서 H.
pylori가 체부 위염을 일으킴으로써 위축성 위염, 장상피화 생, 선종, 형성이상 단계를 거쳐 장형선암이 발생한다는 소 위 Correa 학설이 많이 받아들여지고 있다.1-3,19 위축성 위염 과 장상피화생은 위암을 발생시키는 인자이며20 위축성 위 염의 정도와 범위가 심할수록 위암을 발생시킬 위험성이 크 다. 위암환자의 전정부와 체부의 조직이 정상대조군보다 위 선의 위축과 장상피화생이 더 심하다.21 이번 연구에서 종양 발생에 관여하는 위험인자 분석에서 체부의 선위축 및 전정 부의 장상피화생이 위선종 및 장형선암에 유의한 인자였다.
위선종 및 위암군의 H. pylori 감염률이 대조군보다높아 H. pylori와 위암과 연관성이 있다.22 H. pylori와 위종양의 연 관성에 대한 연구 결과를 해석할 때 고려해야 할 것으로는 첫째, 대조군의 H. pylori 감염률이 높은 경우 위종양군과 대 조군의 차이를 구분하기가 불충분하여 위험도가 실제보다 낮은 점, 둘째, H. pylori 감염이 위축성 변화와 장상피화생
을 일으키고 결국 위선종이나 위암이 생기는 동안 생존에 불리한 환경으로 인해 H. pylori의 군집이 사라져23 이로 인 해 위종양군의 H. pylori 감염률이 낮게 측정되는 것, 셋째, 위종양군과 대조군 간의 동질성이 확보되지 않을 때 위험도 측정오차 등이다. 이번 연구에서 위종양군과 대조군의 연령 및 성별은 차이가 없었으나 H. pylori 감염률은 차이가 없었 다. 이는 대조군의 H. pylori 감염률이 65-73%로 비교적 높 았고, 위종양군 및 대조군의 대상환자 수가 적은 점이 일부 기여했을 것이다.
세포자멸사와 세포증식의 불균형이 종양의 발생 및 진행 에 관계한다.24 세포자멸사는 프로그램된 세포사로 세포증 식에 대해 보완적이면서 반대 역할을 하여 세포수를 조절하 고 항상성을 유지한다. 정상 위점막에서는 1-3%의 세포자멸 사가 관찰된다. H. pylori 감염이 세포자멸사를 유발시킬 수 있으며 H. pylori 감염을 동반한 위점막의 세포자멸사 빈도 는 16.8%로 높으며 H. pylori 제균치료 시 3.1%로 감소한 다.8,9 소화성 궤양, 위염, 장상피화생, 형성이상 및 위암 환 자를 대상으로 한 여러 보고25-28에서 H. pylori 감염은 위점 막 상피세포의 세포자멸사를 증가시킨다. 한편, p53 종양억 제유전자는 17번 염색체에 존재하며 세포주기 조절, DNA 복구 및 합성, 세포자멸사에 중요한 역할을 한다.29 p53 유전 자 돌연변이는 많은 종양에서 나타나는데 위암에서는 42.5- 57%의 높은 빈도로 발현하며 불량한 예후인자와 연관이 있
다.30,31 p53 유전자 기능상실로 세포자멸사가 억제됨으로써
손상된 DNA를 가진 세포가 제거되지 않고 생존하여 암 발 Table 3. Odds Ratios of Gastric Adenoma to Control in Multiple Logistic Regression Analysis
p-value Odds ratio 95% CI
Intestinal metaplasia at antrum 0.093 2.657 0.849-8.312 Intestinal metaplasia at body 0.266 2.098 0.568-7.744
Atrophy in body 0.047 3.737 1.020-13.690
Drinking 0.156 3.139 0.646-15.253
Smoking 0.630 1.011 0.968-1.054
Table 4. Odds Ratios of Gastric Carcinoma to Control in Multiple Logistic Regression Analysis
p-value Odds ratio 95% CI
Intestinal metaplasia at antrum 0.010 4.378 1.426-13.443 Intestinal metaplasia at body 0.347 1.882 0.503-7.037
Atrophy in body 0.948 0.944 0.167-5.347
Drinking 0.042 4.899 1.062-22.604
Smoking 0.183 1.028 0.987-1.069
274 대한소화기학회지: 제46권 제4호, 2005
생에 관여할 수 있다. Ki-67 단일클론 항체는 휴지기 세포에 는 없지만 증식하는 세포의 세포주기에 존재하는 핵 항원과 반응하며 진행위암 및 림프절전이가 동반된 위암에서 높은 표지 지수를 보인다.32
종양조직의 세포자멸사 및 세포증식 발현율을 관찰한 연 구에서 장형선암은 선종에 비해 p53 및 Ki-67의 발현이 유 의하게 높았고 세포자멸사는 낮은 빈도를 보였다.33 세포자 멸사/세포증식 비는 염증이 심할수록 비례하여 증가하였으 나 만성위염군보다 장상피화생, 형성이상, 위암으로 진행할 수록 세포자멸사에 비해 더 과도한 세포증식으로 세포자멸 사/세포증식 비는 감소한다.34 위종양군의 세포증식이 위궤 양군보다 낮았으며 이는 위종양군의 감소된 급성 염증이나 선위축과 연관이 있다.28 이번 연구는 종양의 주변점막에서 세포자멸사 및 세포증식 단백질의 발현을 관찰하였는데 장 형선암 및 위선종군의 주변점막은 대조군과 차이가 없었다.
이는 각 군의 H. pylori 감염률이 차이가 없는 점, 세포자멸 사를 관찰한 TUNEL 방법은 고정방법과 고정시간에 영향을 받는 한계가 있는 점, 종양의 주변점막은 위염 또는 장상피 화생으로 대조군과 크게 다르지 않는 점이 기여했을 것이 다.
결론적으로 세포자멸사와 세포증식의 불균형이 위암발생 에 관여하는 것으로 생각하나 종양 주변점막의 세포자멸사 및 세포증식 단백질 발현율은 대조군과 차이가 없었다. 향 후 대상 환자수의 보완과 H. pylori 감염 음성 및 양성 환자 를 구분하여 주변점막의 세포자멸사 및 세포증식 발현율의 차이를 알아보고 관계하는 Bcl-2, Bcl-XL, Bax 등의 추가 검 사가 필요할 것으로 생각한다.
요 약
목적: 위암은 H. pylori 감염으로 위축성 위염과 장상피화 생을 거쳐서 발생하며 세포자멸사와 세포증식의 불균형이 관련되어 있다. 저자들은 종양 주변점막에서 H. pylori 감염 률, 위염의 조직소견, 여러 환경 위험인자를 조사하여 위종 양 발생에 관여하는 유의한 위험인자를 분석하였고 세포자 멸사 및 세포증식 단백질의 발현을 조사하였다. 대상 및 방 법: 1998년 9월부터 2001년 11월까지 대구가톨릭대학병원 에서 위내시경 생검을 통해 장형선암으로 진단된 20예, 저 도 형성이상 선종 20예, 대조군 40예를 대상으로 선암과 선 종의 병변으로부터 2 cm 이상 떨어진 부위의 전정부와 체 부에서 채취한 조직에서 H. pylori 감염률, 위염의 조직소견, Ki-67과 p53 단백질의 발현율 및 세포자멸사를 조사하였다.
결과: H. pylori 감염률은 각 군 간에 차이가 없었다. 음주력 및 흡연력, 전정부 및 체부의 장상피화생의 정도는 위선종 과 장형선암군이 대조군에 비해 유의하였다. 다항 로지스틱
회귀분석 결과, 위선종군에서는 체부 선위축(OR=3.7), 장형 선암군에서는 전정부 장상피화생(OR=4.4) 및 음주력(OR=4.9) 이 유의한 위험인자로 나타났다. 주변 점막의 세포자멸사 및 세포증식 발현율은 각 군 사이에 차이가 없었다. 결론:
음주력 및 장상피화생이 장형선암 발생에 독립적으로 유의 한 인자였고 종양의 주변점막에서 세포증식 단백질의 발현 과 세포자멸사는 대조군과 위종양군 간에 차이가 없었다.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 색인단어: Helicobacter pylori, 위선종, 위선암, 종양발생, 세
포자멸사
참고문헌
1. Parsonnet J, Friedman GD, Vandersteen DP, et al. Helico- bacter pylori infection and the risk of gastric carcinoma. N Engl J Med 1991;325:1127-1131.
2. Talley NJ, Zinsmeister AR, Weaver A, et al. Gastric carci- noma and Helicobacter pylori infection. J Natl Cancer Inst 1991;83:1734-1739.
3. Nomura A, Stemmermann GN, Chyou PH, Kato I, Perez- Perez GI, Blaser MJ. Helicobacter pylori infection and gastric carcinoma among Japanese Americans in Hawaii. N Engl J Med 1991;325:1132-1136.
4. An international association between Helicobacter pylori in- fection and gastric cancer. The EUROGAST Study Group.
Lancet 1993;341:1359-1362.
5. International Agency for Reserch on Cancer, World Health Organization. Schistosomes, liver flukes and Helicobacter pylori.
IARC working group on the evaluation of carcinogenic risks to humans. IARC Monogr Eval Carcinog Risks Hum 1994;
61:218-220.
6. Kuipers EJ, Gracia-Casanova M, Pena AS, et al. Helicobacter pylori serology in patients with gastric carcinoma. Scand J Gastroenterol 1993;28:433-437.
7. Kato S, Onda M, Matsukura N, et al. Genetic polymorphisms of the cancer related gene and Helicobacter pylori infection in Japanese gastric cancer patients. An age and gender matched case-control study. Cancer 1996;77(suppl):1654S-1661S.
8. Moss SF, Calam J, Agarwal B, Wang S, Holt PR. Induction of gastric epithelial apoptosis by Helicobacter pylori. Gut 1996;38:498-501.
9. Piotrowski J, Piotrowski E, Skrodzka D, Slomiany A, Slo- miany BL. Induction of acute gastritis and epithelial apoptosis by Helicobacter pylori lipopolysaccharide. Scand J Gastroen- terol 1997;32:203-211.
10. Lynch DA, Mapstone NP, Clarke AM, et al. Cell proliferation in Helicobacter pylori associated gastritis and the effect of
eradication therapy. Gut 1995;36:346-350.
11. Xin Y, Wu D, Zhao F. Study of the relationship between the expression of Ki-67 antigen and the pathobiological beha- viours of stomach cancer. Zhonghua Zhong Liu Za Zhi 1997;
19:382-384.
12. Ikeda M, Shomori K, Endo K, Makino T, Matsuura T, Ito H.
Frequent occurrence of apoptosis is an early event in the onco- genesis of human gastric carcinoma. Virchows Arch 1998;
432:43-47.
13. Baba M, Konno H, Tanaka T, et al. Relationship of p53 and Helicobacter pylori to clinicopathological features of human remnant stomach cancer after gastric surgery for primary gastric cancer. Oncol Rep 2001;8:831-834.
14. Lauren P. The two histological main type of gastric carci- noma: diffuse and so-called intestinal type carcinoma. Acta Pathol Microbiol Scand 1965;64:31-49.
15. Goldstein NS, Lewin KJ. Gastric epithelial dysplasia and ade- noma: historical review and histological criteria for grading.
Hum Pathol 1997;28:127-133.
16. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis. The updated Sydney System.
International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996;20:1161-1181.
17. Antonioli DA. Precursors of gastric carcinoma: a critical re- view with a brief description of early (curable) gastric cancer.
Hum Pathol 1994;25:994-1005.
18. Sipponen P, Kekki M, Haapakoski J, Ihamaki T, Siurala M.
Gastric cancer risk in chronic atrophic gastritis: statistical cal- culations of cross-sectional data. Int J Cancer 1985;35:173- 177.
19. Correa P. Precursors of gastric and esophageal cancer. Cancer 1982;50:2554-2565.
20. Ming SC, Goldman H, Freiman DG. Intestinal metaplasia and histogenesis of carcinoma in human stomach. Light and elec- tron microscopic study. Cancer 1967;20:1418-1429.
21. Yoshimura T, Shimoyama T, Tanaka M, Sasaki Y, Fukuda S, Munakata A. Gastric mucosal inflammation and epithelial cell turnover are associated with gastric cancer in patients with Helicobacter pylori infection. J Clin Pathol 2000;53:532-536.
22. Komoto K, Haruma K, Kamada T, et al. Helicobacter pylori infection and gastric neoplasia: correlations with histological gastritis and tumor histology. Am J Gastroenterol 1998;93:
1271-1276.
23. Karnes WE Jr, Samloff IM, Siurala M, et al. Positive serum antibody and negative tissue staining for Helicobacter pylori in subjects with atrophic body gastritis. Gastroenterology 1991;101:167-174.
24. Kerr JF, Winterford CM, Harmon BV. Apoptosis. Its signi- ficance in cancer and cancer therapy. Cancer 1994;73:2013- 2026.
25. Scotiniotis IA, Rokkas T, Furth EE, Rigas B, Shiff SJ. Al- tered gastric epithelial cell kinetics in Helicobacter pylori- associated intestinal metaplasia: implications for gastric carci- nogenesis. Int J Cancer 2000;85:192-200.
26. Bhang CS, Choi MG, Kim JI, et al. Effects of Helicobacter pylori infection on apoptosis, Bcl-2 and cell proliferation.
Korean J Gastroenterol 1999;34:10-20.
27. Chung SS, Park HJ, Chung BC, et al. Relation of apoptosis and cell proliferation in Helicobacter pylori infection. Korean J Gastroenterol 1998;32:427-434.
28. Jang TJ, Kim JR. Proliferation and apoptosis in gastric antral epithelial cells of patients infected with Helicobacter pylori. J Gastroenterol 2000;35:265-271.
29. Lane DP. Cancer: p53, guardian of the genome. Nature 1992;
358:15-16.
30. Joypaul BV, Hopwood D, Newman EL, et al. The prognostic significance of the accumulation of p53 tumour-suppressor gene protein in gastric adenocarcinoma. Br J Cancer 1994;69:
943-946.
31. Starzynska T, Markiewski M, Domagala W, et al. The clinical significance of p53 accumulation in gastric carcinoma. Cancer 1996;77:2005-2012.
32. Kakeji Y, Korenaga D, Tsujitani S, Haraguchi M, Maehara Y, Sugimachi K. Predictive value of Ki-67 and argyrophilic nucleolar organizer region staining for lymph node metastasis in gastric cancer. Cancer Res 1991;51:3503-3506.
33. Kase S, Osaki M, Honjo S, Adachi H, Ito H. Tubular ade- noma and intramucosal intestinal type adenocarcinoma of the stomach; what are the pathobiological differences? Gastric Cancer 2003;6:71-79.
34. Lee KM, Lee DS, Yang JM, et al. Effect of Helicobacter pylori on gastric epithelial cell kinetics and expression of apoptosis-related proteins in gastric carcinogenesis. Korean J Gastroenterol 2003;42:12-19.