책임저자:김명수, 서울시 서대문구 신촌동 134 연세대학교 의과대학 외과학교실, 120-752 Tel: 02-2228-2123, Fax: 02-313-8289 E-mail: [email protected]
접수일 : 2009년 11월 19일, 심사일 : 2010년 5월 19일 게재승인일 : 2010년 5월 24일
성인 신장이식 후 재발한 초점성 분절성 사구체경화증의 임상양상
연세대학교 의과대학 외과학교실
1, 연세대학교 장기이식센터
2주동진1,2ㆍ이정준1,2ㆍ이병모1,2ㆍ김명수1,2ㆍ허규하1,2ㆍ김수진1,2ㆍ김순일1,2ㆍ김유선1,2
Clinical Characteristics of Focal Segmental Glomerulosclerosis Recurrence after Adult Renal Transplantation
Dong Jin Joo, M.D.
1,2, Jung Jun Lee, M.D.
1,2, Byung Mo Lee, M.D.
1,2, Myoung Soo Kim, M.D.
1,2, Kyu Ha Huh, M.D.
1,2, Soo Jin Kim, M.D.
1,2, Soon Il Kim, M.D.
1,2and Yu Seun Kim, M.D.
1,2Department of Surgery, Yonsei University College of Medicine
1, Research Institute for Transplantation, Yonsei University
2, Seoul, Korea
Background: Recurrence of focal segmental glomerulosclerosis (FSGS) after kidney transplantation is a frequent and still unpredictable complication. Moreover, risk factors for recurrence have not yet been clearly identified.
Methods: We enrolled into our study 2,882 adult kidney recipients who underwent transplantation between April 1979 and April 2009. We retrospectively reviewed clinical manifestations of recurrence of FSGS.
Results: Among the 2,784 adult renal recipients, forty four had undergone renal transplantation for primary FSGS. Of the 44, 12 (27.3%) showed recurrent FSGS. Mean duration between transplantation and FSGS recurrence was 22.8±37.4 months.
There were no significant differences in patient characteristics in the recurrence and non-recurrence groups. The cumulative incidence of FSGS recurrence was 13.8% within 1 year after kidney transplantation and 23.2% within 3 years. The overall graft survival rate in the recurrence group was significantly lower than that of the non-recurrence group ( P =0.0018) and non-FSGS group ( P =0.0001). Graft failure happened more in the recurrence group (75%) than in the non-recurrence group (37.5%, P =0.042).
Conclusions: We failed to find any significant risk factors for FSGS recurrence after renal transplantation.
Key Words: Focal segmental glomerulosclerosis, Kidney transplantation, Risk factors, Recurrence 중심 단어: 국소분절성사구체경화증, 신장이식, 위험인자, 재발
서 론
Focal segmental glomerulosclerosis (FSGS, 초점성 분 절성 사구체경화증)은 여러 원인에 의해 발생할 수 있는 병리학적 소견이다. 소아 말기 신부전의 11%, 성인의 경 우 1∼5% 정도에서 FSGS가 원인질환이 되고 있다(1). 일 차성 FSGS는 신장이식 후에도 20%에서 80%까지도 재발 률을 보고하고 있다(2-5). FSGS는 이식 초기부터 재발할 수 있는 질환으로 FSGS 재발 시에는 이식신의 기능지연
(delayed graft function)과 급성거부반응, 그로 인한 이식 신의 소실까지도 초래할 수 있다(6,7). 1972년 Hoyer 등 (8)에 의해 이식신에서의 FSGS의 재발이 보고된 이래 FSGS의 위험인자와 치료에 대한 많은 연구가 진행되었음 에도 불구하고 아직까지 재발의 위험인자에 대해서도 명 확히 밝혀진 바가 없는 실정이며, 대부분의 보고는 소아 신장이식에 국한된 것이었다. 이에 본 연구에서는 성인에 서 시행한 신장이식 후 발생한 FSGS 재발의 위험인자와 임상양상, 치료효과 및 이식신의 임상경과 등에 논하고자 한다.
대상 및 방법
1979년 4월부터 2009년 4월까지 연세대학교 세브란스 병원 장기이식센터에서 시행한 총 2,882예의 신장이식
중 만 18세 이상 성인을 대상으로 시행한 2,784예의 이 식 증례를 후향적인 방법으로 조사하였다. 대상 환자의 이식 후 임상적 경과와 이식신 생검을 통한 조직학적 진 단을 기본적으로 조사하였으며, 이식 후 FSGS가 재발한 환자에 대하여서는 발병 시기, 진단 당시의 이식신 상태 등을 조사하였으며 이식 후 FSGS가 재발한 그룹과 재발 하지 않은 그룹을 나누어 비교 분석하였다.
1) 정의
신장이식 당시의 연령이 만 18세 이상인 성인 환자를 본 연구의 대상자로 설정하였다. 신장이식 전의 FSGS 진 단은 단백뇨가 처음 감지되어 조직검사를 시행하여 확진 한 경우로 정의하였다. 신장이식 이후 FSGS의 재발은 요 단백의 배출이 1.0 g/day/m2 이상인 경우를 기준으로 하 였고 0.1 g/day/m2 이하일 경우 단백뇨의 완전관해가 이 루어진 것으로 판정했다. 또한 이식신 생검을 통해 광학 현미경으로 FSGS가 증명되거나, 전자현미경으로 사구체 상피세포의 족돌기 소실이 관찰된 경우도 포함하였다.
2) 이식 후 면역억제
대상 환자들의 면역억제요법은 1984년 이전에는 아자티오 프린(azathioprine)과 부신피질호르몬(prednisolone)을 사 용하였으며, 이후에는 시클로스포린(cyclosporine A)과 부 신피질호르몬으로 이중요법 또는 아자티오프린이나 마이코 페놀산을 추가한 삼중요법을 사용하였다. 1998년부터는 타크 로리무스(tacrolimus)를 도입하여 사용하였고, 1999년부터 는 부분적으로 인터루킨-2 수용체 차단제(interleukin-2 re- ceptor blocker)인 daclizumab이나 basiliximab을 면역유도 요법으로 사용하였다. 이식 후 면역억제제는 시클로스포린 의 경우 혈중농도를 150∼200 ng/mL에 맞추어 조절하였으 며 타크로리무스의 경우 5∼10 ng/mL에 맞추어 조절하였다.
급성거부반응 치료로는 스테로이드 강타요법(steroid pulse therapy, methylprednisolone 500 mg/day×4 times for 5 days)을 기본적으로 시행하였으며 이에 반응하지 않 는 경우 항림프구항체(anti-lymphocyte antibody, ALG), OKT3 또는 anti-thymocyte antibody (ATG)를 사용하였 다. 환자 사망, 이식신의 제거 및 투석으로의 전환 등을 이식신 소실로 간주하였다.
3) 통계
FSGS의 발병 연령, FSGS 발병부터 신장이식까지의 기 간, 투석기간, 공여자 연령, HLA 부적합 항체 개수, 투석 방법, 이식 후 6개월 이내의 거부반응 경력 등을 FSGS 재 발의 위험인자로 고려하여 위험인자를 분석하였다. 두 그
룹간의 평균비교는 Mann Whitney test를 이용하였다. 이 식신의 생존율은 Kaplan-Meier method를 사용하였다. 통 계적 수치는 평균과 표준편차로 나타내었으며, P value가 0.05 미만인 경우를 통계적으로 유의하다고 정의하였다.
결 과
연구기간 중 만 18세 이상의 성인 신장이식은 2,784예 시행되었고 그 중 이식 전 FSGS로 신이식을 받은 환자는 총 44명(1.6%) 이었다. 44명의 성인 환자에 대해 44예의 신이식이 시행되었으며 이 중 2명의 환자는 재이식이었 다. 이들에 있어서 FSGS의 발병 연령은 평균 266±12.2 (9∼60)세였으며, 이식 받을 당시의 연령은 평균 31.8±
12.4세로 FSGS 진단 후 신장이식을 받기까지의 평균기간 은 61.9±52.2개월이었다. 이식 전 평균 투석기간은 17.7
±24.0개월이었다. 44명의 FSGS 환자 중 신장이식 후 재 발한 경우는 12명(27.3%)이었다. 이중 9명은 신장 조직검 사를 통해 확인된 FSGS의 재발이었고 3명은 1.0 g/day/
m2 이상의 단백뇨를 배설하여 조직검사 없이 임상적으로 진단되었다.
1) 재발군과 비재발군의 비교
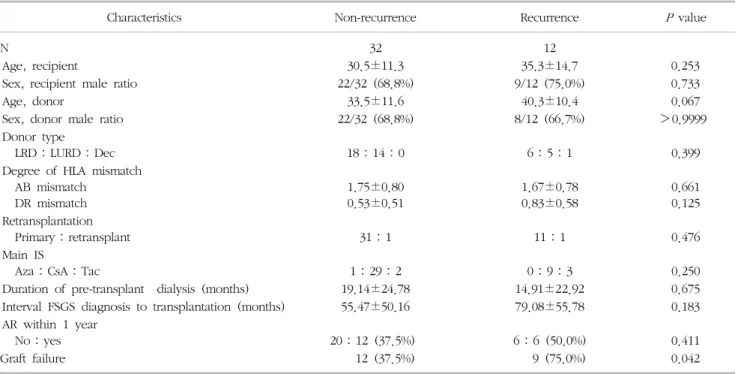
FSGS로 신이식을 받았으나 FSGS가 재발되지 않은 32명 을 비재발군으로 하고 재발한 12명을 재발군으로 하여 비 교하였을 때, FSGS 진단 당시의 연령, 이식 당시 연령, 투 석기간, FSGS 진단 후 이식까지의 기간, 이식 후 1년 이내 거부반응의 발생 병력 등에서 두 군간에 유의한 차이는 없 었다(Table 1). 통계적으로 유의하지는 않으나 FSGS 재발 군에서 공여자의 연령이 비재발군보다 높았고, FSGS 진단 후 이식을 받기까지의 기간이 더 긴 경향을 나타내었다.
2) FSGS의 재발양상
신장이식 후 FSGS의 재발까지는 평균 22.8±37.4개월이 소요되었다. 신장이식 후 FSGS 재발의 누적 발생률은 1년 이내가 13.8%, 3년까지 23.2%였으며, 12명의 재발 환자 중 7명(58.3%)은 1년 이내에 재발하였고 3년 이내에 재발 한 환자는 10명(83.3%)이었다(Fig. 1). 재발 환자에 있어서 재발 진단 당시의 24시간 소변 단백은 평균 6,759.4±
7,058.3 mg/day (62.4∼21,673.3 mg/day)였다.
3) 재발된 FSGS의 예후
이식신 생존율에 있어서 FSGS로 신장이식을 받은 환자 중 재발하지 않은 환자들은 다른 원인질환으로 신장이식 을 받은 환자들과 비교하여 통계적인 차이가 없었다
Table 1. Patient characteristics between FSGS non-recurrence group and recurrence group
Characteristics Non-recurrence Recurrence
Pvalue
N 32 12
Age, recipient 30.5±11.3 35.3±14.7 0.253
Sex, recipient male ratio 22/32 (68.8%) 9/12 (75.0%) 0.733
Age, donor 33.5±11.6 40.3±10.4 0.067
Sex, donor male ratio 22/32 (68.8%) 8/12 (66.7%) >0.9999
Donor type
LRD:LURD:Dec 18:14:0 6:5:1 0.399
Degree of HLA mismatch AB mismatch
DR mismatch
1.75±0.80 0.53±0.51
1.67±0.78 0.83±0.58
0.661 0.125 Retransplantation
Primary:retransplant 31:1 11:1 0.476
Main IS
Aza:CsA:Tac 1:29:2 0:9:3 0.250
Duration of pre-transplant dialysis (months) 19.14±24.78 14.91±22.92 0.675 Interval FSGS diagnosis to transplantation (months) 55.47±50.16 79.08±55.78 0.183 AR within 1 year
No:yes 20:12 (37.5%) 6:6 (50.0%) 0.411
Graft failure 12 (37.5%) 9 (75.0%) 0.042
Abbreviations: FSGS, focal segmental glomerulosclerosis; LRD, living related donor; LURD, living unrelated donor; Dec, deceased donor;
IS, immunosuppressive agent; Aza, azathioprine; CsA, cyclosporine A; Tac, tacrolimus; AR, Acute rejection.
Fig. 1. Cumulative incidence of FSGS recurrence after kidney transplantation.
Abbreviation: FSGS, focal segmental glomerulosclerosis.
Fig. 2. Graft survival rate.
Abbreviation: FSGS, focal segmental glomerulosclerosis.
(P=0.7504; Fig. 2). 그러나 신이식 후 FSGS가 재발된 군에 서는 이식신 생존율이 유의하게 저하되었다(P=0.0001;
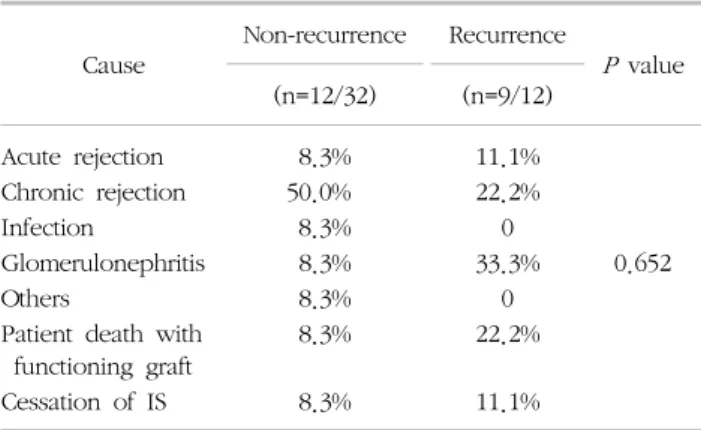
Fig. 2). 12명의 FSGS 재발군 중 9명(75.0%)의 환자에서 이식신의 소실이 관찰되었다. 비재발군 32명 중에서는 12 명(37.5%)의 환자에서 이식신의 소실이 관찰되었다(Table 1, P=0.042). 이들 재발군에서 FSGS 재발 이후의 평균 이 식신 생존율은 54.5±63.9개월이었다. 이식신 소실의 원인 을 보면, 비재발군에서는 만성거부반응이 18.8%로 가장
많은 원인이었고, 재발군에서는 사구체신염 즉, FSGS 재발 자체가 25.0%로 가장 많았다(Table 2).
고 찰
신이식 후 이식신 소실의 원인 중 5% 정도는 원인질 환의 재발인 것으로 알려져 있다(9). 이 중 특히 FSGS는 그 빈도와 재발률이 높고 재발 시에는 이식신의 소실을
Table 2. Causes of graft loss
Cause
Non-recurrence Recurrence
P
value (n=12/32) (n=9/12)
Acute rejection 8.3% 11.1%
Chronic rejection 50.0% 22.2%
Infection 8.3% 0
Glomerulonephritis 8.3% 33.3% 0.652
Others 8.3% 0
Patient death with functioning graft
8.3% 22.2%
Cessation of IS 8.3% 11.1%
Abbreviation: IS, immunosuppressive agent.
가져올 수 있어 신장이식 후 특별한 관심을 가져야 하는 질환이다. 최근의 연구에 의하면, FSGS를 가진 환자들의 거의 대부분은 신장이식 후 2∼24개월 이내에 신증후군 에 해당하는 단백뇨를 보인다고 보고하고 있으며 성인 신이식에 있어서는 평균 14일 만에 재발하는 소아 FSGS 환자의 신이식에서 보다 늦게 나타나는 것으로 보고하고 있다(5). Crosson (10)은 FSGS로 신이식을 받은 환자의 75%에서 4주 이내에 재발한다고 보고하기도 하나, 현재 로서는 전체 신이식의 20%에서 재발이 발생하며 그 절반 인 10%에서 이식신의 소실에 이르는 것으로 알려져 있다 (9). 본 연구에서도 FSGS가 말기 신부전의 원인질환이었 던 환자들 중 신장이식 후 27.3%에서 재발을 보였으며 재발한 환자의 58.3%의 환자가 1년 이내에 재발한 것으 로 나타났다. 이식 후 1개월 이내에 나타난 경우도 2예 있었다. 본 연구의 FSGS 재발 환자에서 신장이식 후 FSGS의 재발까지는 평균 22.8±37.4개월이 소요된 바 상 기 연구의 결과들과 다르지 않았다.
1972년 Hoyer 등(8)이 처음 이식신에서의 FSGS 재발 을 보고한 이래로 전세계적으로 여러 기관들에서 이와 관련한 보고들이 발표되었다(2,3,5,11-13).
그러나, 이러한 노력에도 불구하고 FSGS의 재발의 명 확한 위험인자나 기전 및 예방법에 대해서는 알려진 바 없다. 현재까지 논의된 위험인자로는 발병연령, 만성신부 전으로의 진행기간, 이식 전 신생검에서 사구체간질 과세 포성, human leukocyte antigen (HLA) matching, 투석 기간, 신공여자의 종류, 시클로스포린 사용 여부 등이 있 다. 이 중, HLA matching 은 일란성 쌍생아 간의 이식 후 재발에 대한 보고(14) 이후로 재발의 위험인자로 생각 되었으나 최근의 보고들에 따르면 역시 의미가 없는 것 으로 보고되고 있다(15-17). 시클로스포린 역시 T-세포 조절체로서 FSGS 발병기전을 억제하여 재발을 막으리라
기대되었으나 오히려 재발의 위험인자로 보고되기도 하 며 아자티오프린 사용군과 유의한 차이는 없어 보인다(4, 18). 투석기간 역시 위험인자로서 의미 없다는 보고가 지 배적이다(15-17). 대상군이 적기는 하지만 국내에서 보고 된 FSGS의 재발에 대한 이전 연구에서도 재발군과 비재 발군 간의 상기의 위험인자들에 대해서 유의한 차이를 보이지 않은 것으로 보고하였다(19).
본 연구는 적은 수의 환자를 대상으로 하여 Cox-reg- ression 모델을 활용한 다인자 분석을 시행할 수는 없었 다. 다만, 통계적 유의성은 없었으나 재발군에서 공여자 의 연령이 좀더 많은 경향이 있었으며, FSGS의 유병기간 이 더 긴 경향을 나타내었다. 기존의 연구들에서도 공여 자의 연령이 FSGS 재발의 위험인자라고 보고하기도 하 였다(4,20). 또한 최대 사구체 직경이 FSGS 재발의 예측 인자라는 보고도 있다(21). FSGS는 알려진 바와 같이 순 환하는 체액성 인자들(circulating humoral factor)에 기 인하는 질환이다(22,23). 이러한 이유로 고연령의 공여 신장에서는 투과성이 증가함으로 인해 FSGS의 재발이 잘 되는 것으로 생각된다(20). 이는 또한 30세 이상의 공 여 신장에서 사구체의 크기가 증가하는 것과도 관련이 있을 것으로 보고되고 있으며 FSGS 재발군에서 비재발 군보다 평균 사구체의 크기가 더 크다고 보고된 것도 이 와 관련이 있을 것으로 추정된다(21). 즉, 연령이 증가함 에 따라 사구체의 크기가 증가하면서 항체에 대한 투과 성이 증가하여 체액성 면역과 관련한 질환인 FSGS의 재 발이 잘 되는 것으로 보인다. FSGS의 유병기간이 재발의 위험인자라는 것에 대해서는 앞서 언급했듯이 논란의 여 지가 있으나 본 연구가 적은 인원을 대상으로 하였으므 로 향후 이에 대한 추가적인 연구가 필요할 것이다.
본 연구에서 언급하지는 않았으나 FSGS가 재발되었을 경우, 어떻게 치료해야 할 것인지에 대해서는 아직까지 논란의 여지가 있다. 재발성 FSGS에 대하여 아직까지 정 립된 치료법은 없으나 혈장 반출술과 사이크로포스파마 이드(cyclophosphamide)의 투여가 효과적인 것으로 알 려져 있다(24-26). 그러나 아직도 이에 대한 전향적 연구 가 진행되어 있지 않으며 간헐적인 치료 결과들이 보고 되고 있는 실정이다. 본 연구에 포함된 12명의 재발성 FSGS 환자들 중 최근 2명의 환자에서 혈장반출술과 사 이크로포스파마이드를 투여하였다. 그 중 1명의 환자는 반복적인 혈장반출술 이후 단백뇨의 관해를 보였다가 반 복적으로 재발되어 결국 이식신의 소실에 이르렀고, 다른 한 명의 환자는 현재 혈장반출술 이후 단백뇨가 줄면서 호전을 보이고 있다. 향후 이러한 FSGS의 치료 방법과 그 결과에 대한 광범위한 연구가 필요할 것이다.
결 론
FSGS로 신장이식을 받은 환자들의 이식신 생존율은 다른 원인질환으로 신장이식을 받는 환자들과 비교하여 차이가 없었으나, 이식 후 재발되었을 때 이식신 소실의 가능성이 높은 질환이다. 본 연구에서는 통계적으로 유 의한 FSGS의 재발에 대한 위험인자를 확인할 수는 없었 으나, 향후 더 많은 수의 환자를 대상으로 하는 연구가 필요할 것이며 재발된 FSGS의 치료에 대한 전향적 연구 가 필요할 것이다.
감사의 글
본 논문은 2009년도 연세대학교 의과대학 장기이식연 구소의 연구비 지원으로 이루어졌음.
REFERENCES