Received: February 8, 2017 Revised: March 2, 2017 Accepted: March 16, 2017.
Corresponding author: Ji Won Yoo
Division of Geriatric Medicine, Department of Internal Medicine, University of Nevada School of Medicine, 1701 W Charleston Blvd., #230, Las Vegas, NV 89102, US
Tel: +1-702-671-6496, Fax: +1-702-671-2376, E-mail: ji.yoo@unlv.edu Copyright Ⓒ 2017 The Korean Academy of Clinical Geriatrics
This is an open access article distributed under the term s of the Creative Com m ons Attribution Non-Com m ercial License (http://creativecom m ons.org/ licenses/by-nc/4.0) which perm its unrestricted non-com m ercial use, distribution, and reproduction in any m edium , provided the original work is properly cited.
미국 장기 요양기관 진료 및 장기요양 정책 고찰
Xibei Liu 1 , 한규태 2 , Takashi Yamashita 3 , 유지원 4
1
아리조나주립대 의과대학 내과학교실,2
연세대학교 의과대학 예방의학교실,3
메릴랜드주립대 사회인류보건학부,4
네바다주립대 의과대학 내과학교실Long-term Care Practice and Health Policy in the United States
Xibei Liu 1 , Kyu-Tae Han 2 , Takashi Yamashita 3 , Ji Won Yoo 4
1
Department of Medicine, University of Arizona College of Medicine, Tuscon, Arizona, USA,
2Department of Public Health, Yonsei University College of Medicine, Seoul, Korea,
3Department of Sociology, Anthropology, and Health Administration &
Policy, University of Maryland Baltimore County, Baltimore, Maryland,
4Division of Geriatric Medicine, Department of Internal Medicine, University of Nevada School of Medicine, Las Vegas, Nevada, USA
In the United States, nursing homes have evolved dramatically over the past several years, responding to a variety of government and market-driven forces. The almshouse, common at the turn of the 20
thcentury, has been transformed into a highly-regulated institution for people who often have severe physical and mental disabilities. Nursing homes, more than ever, present the clinician with a set of unique and complex care issues. This review will discuss United States long-term care practice and health policy in the context of population needs, government policy, and reimbursement, and staffing patterns using a patient story.
Key Words: Health service, Nursing home, United States
서 론
미국 베이비부머가 노인인구에 편입되면서 장기요양서 비스 수요가 증가되었다. 이로 인한 장기요양서비스 대 부분의 요양급여를 제공하고 서비스 질관리를 담당하는 해당 보건당국은 최근 진료의 질과 요양급여를 연동시 키는 정책을 도입하였다. 취임 첫 날 전임 오바마 대통 령이 주력해온 Affordable Care Act (ACA)를 “Repeal and
Replace”하겠다는 트럼프 대통령 시대를 맞이했다. 한편, 미 공화당 지도부를 포함한 정치권과 미 의사협회, 소비자 권익 사회단체 등에서는 곧이어 분명한 반대 및 우려를 표명하였다. 누구도 쉽게 미국 장기요양 정책이 어떻게 변 화될지 모르는 혼돈의 시대에 높여있다. 이번 종설은 미국 요양기관 진료 및 장기요양 정책 고찰로서 최근 노인인구 가 급증하는 한국 의료계에 참고 자료가 될 수 있다.
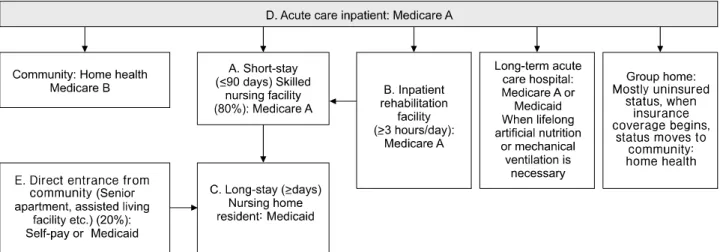
Figure 1. Utilization and payment of long-term care. Modified from Yoo et al.
9Res Gerontol Nurs, 2015.
본 론
1. 환자 이야기(the patient’s story): A. 급성병원에 서 요양기관으로
77세 남자 환자 김씨는 급성신부전(혈중 크레아티닌 10.8 mg/dl)과 고칼륨혈증(8.3 mEq/L)으로 미국 네바다주 립 병원 응급실에 내원하였다. 김씨는 지난 10년 동안 제2형 당뇨, 본태성 고혈압, 수축성 울혈성 심부전(최근 3개월 전 ejection fraction 30%), 만성신부전 제4기, 관상 동맥질환 등의 다양한 만성질환을 갖고 있다. 김씨는 2004년 네바다주 거주하는 딸과 노년을 같이 지내기 위해 한국에서 이주하였다. 현재 연방정부 Center for Medicare and Medicaid Services (CMS)에서 65세 이상 노 인ㆍ보조하는 메디케어(Medicare)와 네바다주에서 빈곤 층에 제공하는 메디케이드(Medicaid)를 보조받고 있으며 사회보장청(Social Security Administration)으로부터 매달 400불씩 보조 받고 있었다. 부인은 2년 전 자궁경부암으 로 사별하였으며 이후 환자 김씨는 라스베가스에 사는 큰 딸로부터 운전ㆍ병원예약ㆍ은행업무 등의 도구적 일 상생활능력(instrumental activities of daily living)
1)
에 도움 을 받고 있었다. 입원 3일 전까지 독립적으로 일상생활 능력(activities of daily living)2)
을 유지하고 있었다.병원 입원 후 김씨는 응급 혈액투석을 받고 노인전용 병동(acute care for the elders, ACE unit)
3)
으로 옮겨져 포 괄적 노인평가(comprehensive geriatric assessment, CGA)를 받았다. 간이 인지기능검사(mini-cog test)4)
에서 2개 항목 과 시계 그리기 검사결과 부적절히 답하였다. 혼돈평가 방법(confusion assessment method)5)
상 섬망을 배제할 수있었다. 보행이 불편하여 침대에서 화장실로 이동할때 부축히 필요했으며 보행기를 갖고도 30 meter 거리인 노 인전용병동내 복도를 한 번에 보행하지 못하였다. 환자 김씨, 주 보호자인 첫째 딸, 노인전용병동 담당 주치의ㆍ 물리치료사와 몇 차례 퇴원계획을 논의한 결과 2∼3주 가량 재활 목표로 집 근처 요양병원(skilled nursing fa- cility)으로 퇴원하였다.
2. Nursing home population, availability, and flow in the united states
요양원과 요양병원은 실제 같은 장소에서 같은 의료 인력에 의해 운영되고 있으며 차이점은 해당 급여가 메 디케어와 메디케이드에 따라 달라진다. Figure 1 “가” 항 목과 같이 CMS 메디케어 A부분에서 제공되는 요양병원 입원 후 20일간 자비부담 없이, 21일부터 100일간은 하 루 170불 가량 자비부담 또는 메디케어 외 2차 사적보험 (supplementary insurance)을 통해 요양급여가 제공된다.
6)
Figure 1 “나” 항목과 같이 요양병원 기관에서 하루 3시 간 이상(주말에 관계 없이) 재활에 관련된 물리ㆍ작업ㆍ 언어ㆍ심리치료를 받을 경우 단기집중재활(inpatient re- habilitation)로 간주한다.6)
단기집중재활의 평균 요양일수 는 5일에 불과하며 가장 흔한 주진단은 중풍과 고관절 골절이다.6)
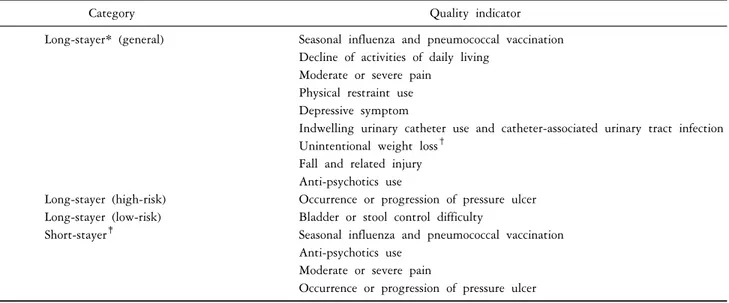
단기집중재활은 요양병원ㆍ요양원과 같은 요 양기관에서 이루어진다. 하루 3시간 이상 단기집중재활 에서 하루 2시간 이하 요양병원에 해당되는 재활 일정으 로 바뀔 뿐이다. Figure 1 “다” 항목과 같이 91일 이상 요양원(nursing home)에 머무를 경우 장기거주자에 해당 되며 급여는 메디케어에서 메디케이드로 전환 과정을Table 1. CMS quality indicators of long and short nursing home stays
Category Quality indicator
Long-stayer* (general) Seasonal influenza and pneumococcal vaccination Decline of activities of daily living
Moderate or severe pain Physical restraint use Depressive symptom
Indwelling urinary catheter use and catheter-associated urinary tract infection Unintentional weight loss
†Fall and related injury Anti-psychotics use
Long-stayer (high-risk) Occurrence or progression of pressure ulcer Long-stayer (low-risk) Bladder or stool control difficulty
Short-stayer
‡Seasonal influenza and pneumococcal vaccination
Anti-psychotics use Moderate or severe pain
Occurrence or progression of pressure ulcer
CMS: center for medicare and medicaid services. *Long-stayer, ≥91 days in nursing home.
†Unintentional weight loss, 4.5 kg weight loss in the past 6 months or 10% weight loss in the past 12 months.
‡Short-stayer, ≤90 days in nursing home.
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-instruments/NursingHomeQualityInits/NHQIQualityMeasures.html.
Accessed 21 January 2017.
거치게된다. 대게 환자 명의의 부동산 등이 요양원에 저 당이 잡혀 매달 공제되며 남은 재산이 해당 주에서 지정 한 생활보호기준에 해당되면 메디케이드로 전환되며 삶 을 마무리 할 때까지 자비부담 없이 요양원에 머무를 수 있다. Yoo 등
8)
에 의하면, 요양병원에서 요양원 상태로 장기거주자가 되는 경우는 28%로 보고 되었다. 2015년 발간된 CMS 장기요양 개요서(CMS nursing home compen- dium) 기준으로 요양기관 장기 거주자의 연간 총 비용이 전국 평균 $90,500 (한화 약 1억 1천만 원)이다.7)
또한, 같은 개요서에서는2014년 기준 미국에는 15,640개의 요 양원이 있으며 약 백오십만 명 환자가 거주하고 있다.7)
요양기관은 72.2% 민간 영리기관이며 공공기관 운영체 는 6.2%에 불과하다.7)
100∼199병상의 중형규모 요양기 관이 44.1%로 가장 흔하다. 65세 이상은 85%이며 평균 나이는 82.6세이다.7)
기계적으로 변형된 식이가 필요한 경우는 35%, 인공영양의 경우는 5%이다. 60∼70%의 경 우 요실금 또는 보행장애로 도움이 필요하다.7)
Figure 1“라” 항목과 같이 급성 병원을 통해 요양병원으로 들어 오는 경우는 80%이며, Figure 1 “마” 항목과 같이 지역 사회, 예를 들면 노인아파트(senior apartment) 등에서 직 접 요양원으로 들어오는 경우는 대략 20%이다.
9)
3. Quality of care and quality of life
통합예산총괄조정법(Omnibus Budget Reconciliation Act) 이 1987년 제정된 이후 연방 정부산하 CMS와 주정부산 하 건강기구에서는 매년 장기요양기관의 진료의 질을 평가하고 일반에 공개한다. 요양기관 평가의 기준은 주 정부산하 기구에서 시설관리 등 실사조사, 온라인으로 진료결과 및 간호인력을 자체보고한다. 주요 진료의 질 평가 항목은 Table 1과 같이 장기 거주와 단기 거주자로 구분되어진다.
10)
항정신약물 사용ㆍ억제대 사용이 요양원 환자에게 부정적 결과를 미치는 최근 연구결과11)
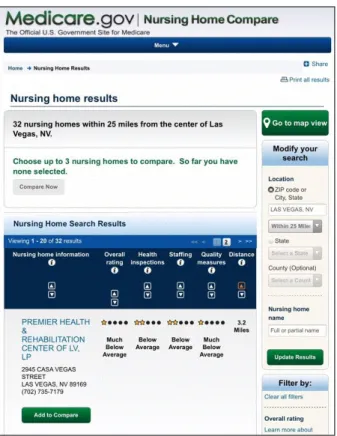
를 반영 해 요양원 환자들에게 항정신약물 사용ㆍ억제대 사용 여 부를 2015년부터 진료의 질 평가 항목에 포함되었다.Figure 2와 같이 CMS는 매년 요양기관의 진료의 질을 5 등급으로 나눠(5등급 최고등급, 1등급 최저등급) ‘Nursing Home Compare’라는 항목으로 CMS 누리집에 공개한다.
12)
환자ㆍ보호자들이 병원에서 퇴원하는 시점에서 집주변 요양기관을 정해야되는 경우가 많아 2002년 부터시행된 Nursing Home Compare은 점차 많이 사용되고 있다.요양보험은 평가된 요양기관의 진료의 질이 소속된 환자안전에 우려될 경우 해당 주정부산하 보건국에 행 정조치를 권고한다. Grabowski 등
13)
에 의하면 2012년 전 국적으로 11.2% 요양기관이 “결핍(deficiency)” 상태로 행 정주의를 받았고, 5.9%의 경우 요양기관 폐쇄 등 강력한Figure 2. Nursing home compare in center for medicare and medicaid services. http://www.medicare.gov/nursinghomecompare/
search.html. Accessed 21 January 2017.
행정조치를 받았다. 하지만, Werner 등
14)
에 의하면 5등 급 Nursing Home Compare는 진료의 질과 연관성이 통계 적으로 유의하지 않은데, 이유로 Nursing Home Compare 가 진료결과나 간호인력보다는 시설관리에 의해 결정되 기 때문으로 분석되고 있다.또한, Kim 등
15)
에 의하면, 요양원 장기 거주하는 환자 들을 대상(중등도ㆍ진행 치매환자 제외)으로한 삶의 질 과 Nursing Home Compare 간의 상호연관성 연구에서 환 자 개인의 삶의 질은 Nursing Home Compare 요양기관 5 등급 진료의 질과는 연관성이 없었다. 일상생활능력이 독립적일수록 환자 개인의 삶의 질은 높았다.15)
4. Minimum data set and financing
요양보험국에서는 Minimum Data Set (MDS)이라는 보 고서를 요양기관이 정해진 기간동안 작성해 온라인으로 보고하도록 규정하고 있다. MDS는 주로 요양기관 내 전 담 간호사가 각 환자마다 작성하며 새로 기관에 들어온 지 2주 이내, 주요 변동이 생길 때, 매 90일마다, 그리고 퇴원 또는 사망 시 요양기관에 작성의무가 있다. MDS는
이름이 내포하는 의미와 달리 방대한 정보를 포함하며 (첫 평가 시 45쪽, Minimum Data Set 3.0 comprehensive version 1.14.1)
16)
일상생활능력(ADL)2)
등 임상정보, 환자 의 퇴원계획, 사전의사결정이 포함된다.또한, MDS는 내재된(built-in) 연동기능, 이른바 ‘case-mix measure’ 기능
17)
을 통해 임상기록이 자동산출되어 요양 기관이 요양보험국 또는 주정부산하 건강기구로부터 받 는 요양급여를 포괄수가제(case-payment) 형식으로 결정 한다. 요양급여는 재활에 중점을 둔 고관절 골절이나 중 풍 환자에 많은 가중치를 두고, 주로 간호에 중점을 둔 치매환자에게는 적은 가중치를 두어서 환자에 따라 요 양기관이 받는 급여비는 3배 가까이 차등이 생길 수 있 다.17)
다만, 촉탁의를 포함한 의사 및 유사의사에게 주어 지는 급여는 MDS에 적용되지 않고 행위별 수가제(fee- for-service)에 의해 결정된다.요양보험국에서는 시범 사업으로 가치기반구매(value- based purchasing) 프로그램을 통해 급성병원이송을 줄이 고 진료의 질 향상된 요양기관에 추가 인센티브 급여를 제공하였으나 Grabowski 등
18)
에 의하면 시범 사업이 요 양기관의 전반적인 진료의 질 향상을 이끌지 못하였다.미 하원에서는 2014년 의료비 절감을 목적으로 가치기 반구매 프로그램을 2018년부터 전국적으로 도입하는 법 을 통과시켜
19)
요양병원 입소 30일 이내 급성병원 이송 이 생길 경우 요양기관에 지급하는 급여비를 2% 삭감할 예정이다.20)
5. Staffing patterns
장기요양 개요서
7)
에 의하면, 요양원의 경우 환자 일 인당 하루 평균 4.04시간(242분) 요양서비스를 받으며 이중 대부분 2.5시간은 간호보조사(certified nursing assis- tant) 담당이며 물리ㆍ작업ㆍ언어치료의 경우 0.35시간, 의사 및 유사의사(mid-level practitioner; physician assistant, nurse practitioner)에 의한 진료시간은 0.15시간에 불과하 다. CMS는 각 요양기관에 의료감독인(medical director)을 임명하여 야간ㆍ주말에 요양기관 환자들이 의사들의 진료 접근성을 담보하고자 한다.7)
미국의료감독학회(American Medical Director Association)에서는 요양기관에 거주하는 환자에게 흔한 5가지 진료 지침을 2013년 다음과 같이 발표하였다.21)
첫째, 진행성 치매환자에게 인공영양 보 다는 수기영양을 권하고, 둘째, 장기거주 환자에게는 인 슐린 슬라이딩 스케일을 적용하지 말고, 셋째, 요로감염증상 및 징후가 명확하지 않으면 소변 배양을 하지 말 고, 넷째, 명확한 평가 전까지 치매환자 정신행동증상에 항정신약물을 자제하며, 마지막으로 기대수명이 제한된 환자에게는 statin 사용을 자제할 것. 또한 CMS는 요양기 관에 들어온 환자에 대해 의사가 첫 90일동안은 매달, 이후 최소 두 달에 한 번씩 진료를 보게 하여 최소한의 의료서비스를 보장하고 있다.
7)
간호인력의 잦은 이직으로 인한 근속기간 단축이 요 양기관 관리의 큰 과제이다. 최근 Grabowski 등
22)
의 보고 에 의하면 간호인력 직장만족도는 근속기관에 유의하게 연관이 있으며 이들의 근속기간이 짧을수록 소속된 요 양기관 환자들의 급성병원 이송 확률이 높아지는 것으 로 알려져 있다. 특히 간호보조사의 낮은 임금이 이직의 주요 요인으로 뽑히는데 아직 이렇다할 해결책이 보이 지 않고 있다.6. 환자 이야기(The patient’s story): B. 요양기관에 서 다시 병원으로
요양병원에서 재활치료를 받는 중 섬망이 발생되어 정확한 진단과 원할한 치료를 위해 급성 병원으로 이송 되었다. 급성 요로감염이 진단되어 정맥주사 항생제 투 여 받은 후 활력징후 및 정신상태가 안정되어 다시 요양 기관으로 돌아왔다.
7. The interface of acute and long-term care
CMS 2013년 발표23)
에 의하면 요양병원에서 급성병원 으로 이송되는 경우는 2000년 18.2%에서 2011년 24.8%로 증가되어는 추세다. 가장 흔한 원인은 패혈증(13%), 폐렴(7%), 요로감염(6%) 등이다. CMS는 2011년 한해에 만 요양병원에서 급성병원으로 이송되어 $140 billion 이 상 추가비용을 추정하였다.
23)
Yoo 등9)
및 Neuman 등24)
에 의하면, 급성병원 이송 요인은 Nursing Home Compare 요 양기관 5등급 등 시설적 요인보다는 개인적 요인에 의해 결정되었다. 이러한 비용을 줄이기 위한 노력으로 대표 적으로 요양병원과 급성병원 의료인 간 원할한 의사소 통, 선행의사결정을 강조한 INTErventions to Reduce Acute Care Transfers quality improvement (INTERACT) 프로그램25)
이 시범 도입되어 요양병원에서 급성병원으로 이송이 17% 가량 감소되었다. 전국적으로 요양기관들이 맞춤 프 로그램을 개발해 요양병원애서 급성병원 이송을 줄이려 고 움직임이 활발하지만 전국적 감소 추세는 보이지 않고 있다.
8. 환자 이야기(the patient’s story): C. 삶의 마무 리를 요양기관에서
김씨는 재활치료를 받는 90일동안 세 번의 급성 병원 으로 이송되어 처음 계획된 만큼 원할한 재활치료를 받 지 못했다. 보행기능이 온전히 회복되지 못했고 목욕ㆍ 옷 갈아입은데 요양원 간호보조사의 도움이 필요했다.
요양원에 들어온지 3년의 시간이 지나가면서 김씨의 인 지기능도 감소해서 어느덧 하루에 의미있는 단어수가 불과 5개 내외이며 미소를 짓지 않아 functional assess- ment scale 기준
26)
으로 진행성 치매상태에 이르렀다. 또 한 손으로 음식을 떠 먹여야만 했다. 체질량지수는 불과 17였다. 김씨 딸을 비롯한 가족들과 요양원 의료진과 만 나 진료계획을 정했다. 진행성 치매의 영양공급에 대한 문헌검색 결과를 김씨 가족들에게 설명해 주었고 결국 김씨는 인공적 영양공급을 않기로 결정했다. 김씨는 더 이상 급성 병원으로 이송되지 않고 4개월 후 요양원에서 생을 마감했다.9. Advance care directives and palliative care in long-term care
미국 요양기관에서 사전의사결정 작성은 Physician Orders for Life Sustaining Treatment (POLST)
27)
도입 이후 에도 법적 위임장 (durable power of attorney) 작성은 요 양기관에서 부족한 상황이다. Hickman 등28)
에 의하면 전 국 규모 연구에서 요양기관에 처음 들어올 때 작성은 26%, 1년 거주시점은 40% 이하에 그치고 있다. Jennings 등29)
에 의하면 캘리포니아주 보건당국은 2009년부터 요 양기관에서 의무적으로 POLST 작성을 의무사항 시행한 2년 후 요양기관에서 사전의사결정 작성률이 절반 가까 이(49%)로 증가되었다.한편, 2014년 미노인의학회
30)
는, 진행된 치매환자의 경우 튜브영양법등 인공영양이 기대수명을 늘리지 않고 오히려 급성 병원이송과 불필요한 항생제 사용이 늘어 나고 있어, 인공영양을 권하지 않고 손으로 떠먹이는 수 기영양을 권한다.결 론
미국 장기요양 진료 및 장기요양 정책에 대해 환자
이야기를 중심으로 고찰해 보았다. 장기요양시설에 촉탁 의제도
31)
를 도입하는 등 급격한 노인인구증가에 따른 진 료와 정책 변화가 요구되는 한국 노인의료계에 참고 자 료가 되길 바란다.REFERENCES