서 론
호산구근막염은 피부경화증 유사한 소견의 피부병변과 근막의 염증이 동반된 질환으로, 말초혈액에서는 호산구 증가, 염증지표의 상승, 고감마글로불린혈증 등이 나타난다.1 주로 상하지에 통증을 동반한 홍반성 부종이 발생하며 발열이나 근육통이 동반될 수 있 으나 그 원인과 병인 기전 및 예후 등에 대해서는 명확히 알려져 있 지 않다. 저자들은 호산구근막염이 의심되는 21세 여자에서 조직 학적 검사를 통해 이를 확진하여 보고하고자 한다. 또한 문헌고찰 을 통하여 현재까지 국내에 보고된 호산구근막염을 특징을 정리하 였다.
증 례
환자: 박OO, 21세 여자
주소: 1개월 전부터 발생한 양측의 하지부종
현병력: 1개월 전부터 손, 발이 붓고 저린 증상이 발생하여 개인 병원을 방문하여 혈액검사를 시행하였으나 특이 소견이 없었다. 이 뇨제로 증상 조절을 시도하였으나 호전이 없고 부종이 점차 진행하 여 본원 류마티스 내과를 방문하였다. 환자는 최근 1개월간 약 4 kg 체중이 증가하였으며, 부종은 발등에서부터 종아리, 허벅지로 진행 하며, 손의 부종도 동반되었으며 발등과 무릎의 통증을 호소하였 다. 환자는 증상 발생 2주 전 수영을 시작하였던 것 이외에 생활 환 경의 변화는 없었고 특별히 복용하는 약도 없었다고 하였다. 본원
Allergy Asthma Respir Dis 8(2):96-101, April 2020 https://doi.org/10.4168/aard.2020.8.2.96 CASE REPORT
Correspondence to: Joo-Hee Kim https://orcid.org/0000-0002-1572-5149
Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, 22 Gwanpyeong-ro 170 beon-gil, Dongan-gu, Anyang 14068, Korea
Tel: +82-31-380-3719, Fax: +82-31-380-3973, E-mail: [email protected]
• This research was supported by a grant from Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education (NFR-2017R1C1B5076565).
Received: April 25, 2019 Revised: June 19, 2019 Accepted: June 19, 2019
© 2020 The Korean Academy of Pediatric Allergy and Respiratory Disease The Korean Academy of Asthma, Allergy and Clinical Immunology This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License
호산구근막염: 증례보고와 문헌고찰
조현웅,1 김현아,2 권미정,3 고성혜,4 김주희,1 김환일,1 박지영,1 박성훈,1 황용일,1 장승훈,1 정기석1
1한림대학교성심병원 호흡기-알레르기내과, 2한림대학교성심병원 류마티스내과, 3한림대학교성심병원 병리과, 4한림대학교성심병원 영상의학과
Eosinophilic fasciitis: A case report with a brief literature review
Hyun-Woong Cho,1 Hyun-Ah Kim,2 Mi Jung Kwon,3 Sung Hye Koh,4 Joo-Hee Kim,1 Hwan Il Kim,1 Ji-Young Park,1 Sung-Hoon Park,1 Yong-Il Hwang,1 Seung Hun Jang,1 Ki-Suck Jung1
1Division of Pulmonary, Allergy, and Critical Care Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang; 2Division of Rheumatology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang; 3Department of Pathology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang; 4Department of Radiology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea
Eosinophilic fasciitis (EF) is a scleroderma-like immune-allergic disorder of unknown etiology and pathogenesis. This rare disease is characterized by the progressive induration of the skin and soft tissue, and peripheral eosinophilia. Here, we report a case of EF. A 21-year-old female was referred due to edema in the upper and lower extremities for 1 month. Laboratory results were unremark- able except for severe eosinophilia. Parasite infestation, venous thrombosis, and cardiac and renal problems were excluded. Mag- netic resonance imaging of both the lower extremities revealed symmetrical thickening and contrast enhancement of crural fascia with adjacent subcutaneous fat infiltration. A full-thickness biopsy at the lower extremity showed infiltration of the fascia by eosino- phils, plasma cells, and lymphocytes with marked edema. Thus, this patient was confirmed to have EF and she was treated with sys- temic corticosteroids, resulting in a remarkable improvement in both edema and eosinophilia. (Allergy Asthma Respir Dis 2020;8:96-101) Keywords: Edema, Eosinophilia, Eosinophilic Fasciitis, Extremities
2017-03-16 https://crossmark-cdn.crossref.org/widget/v2.0/logos/CROSSMARK_Color_square.svg
류마티스 내과에서 혈액검사 후 진통소염제 등을 복용하면서 결과 를 기다리던 중 하지부종이 악화되고 혈액검사에서 호산구 증가가 확인되어 추가 검사 위해 입원하였으며, 호산구 증가 관련질환을 감별하기 위하여 알레르기 내과로 협진 의뢰되었다.
과거력 및 개인력: 소아 시절 아토피 피부염 및 두드러기 병력이 있었으나 10여 년 전부터는 증상이 소실된 상태였다.
가족력: 특이사항 없었다.
진찰 소견: 손과 발, 종아리에 부종이 관찰되었으며, 눌러서 잘 들어가지 않는 비함요성 부종이었다(Fig. 1). 발등과 발바닥 피부는 약간의 발적과 경화성 병변이 관찰되었으나 손은 정상 피부 소견이 었다. 무릎과 발등의 통증을 호소하였으나 상하지 관절의 압통 및 발적은 없었으며, 손과 발의 레이노 현상(Raynaud’s phenomenon) 도 관찰되지 않았다. 상지와 하지의 근력은 모두 정상이었다. 내원 당시 생체 징후는 정상이었으며, 심잡음은 청진되지 않았으며 흉부 와 복부진찰은 정상이었으며, 촉진되는 임파선 비대도 없었다.
검사 소견: 류마티스내과 외래에서 시행한 일반 혈액검사는 백혈 구 10,800/μL (호산구 18%, 절대 호산구 수 1,944/μL)이었으나 1주 후 입원하여 시행한 혈액검사에서 백혈구는 17,100/μL (호산구 41%, 절대 호산구 수 7,011/μL)로 상승되었다. 그러나 혈색소 11.9 g/dL, 혈소판 118 K/μL은 정상 범위였으며, 말초혈액도말검사에서는 경도 의 정구성정색소성 빈혈과 호산구증다증 이외에 다른 소견은 관찰 되지 않았다. 혈청 생화학 검사에서 blood urea nitrogen 10.2 mg/dL, creatinine 0.73 mg/dL, aspartate aminotransferase/alanine ami- notransferase 19/16 IU/L, alkaline phosphatase 74 U/L, gamma- glutamyl transpeptidase 8 IU/L 및 creatine kinase 48 IU/L로 모두 정상이었다. 그러나 Lactate dehydrogenase 742 IU/L (정상: 0–249 U/L)로 상승되었으며, eosinophil cationic protein는 129 μg/L (정 상: 0–15 μg/L)로 증가되어 있었다. 혈청 내 총 면역글로불린 E는
40.0 IU/L로 정상 범위였고 피부반응검사에서는 유럽형과 미국형 집먼지진드기에 3+소견 이외에 나머지 흡입 및 음식물 항원에서는 음성 소견을 보였다. 적혈구 침강률은 2 mm/hr (정상: 0–16 mm/hr) 로 정상이었고 보체 검사에서는 C3과 C4가 83.8 mg/dL (정상: 36–
160 mg/dL), 13.9 mg/dL (정상: 15–45 mg/dL)로 C4가 약간 감소된 소견을 보였다. 혈청 총 면역글로불린 G는 1,102.70 mg/dL (정상:
680–1,620 mg/dL)으로 정상 범위에 있었다. 자가 항체 검사에서는 anti-nuclear antibody가 양성으로 homogeneous 형태였고, anti- neutrophil cytoplasmic antibodies는 음성 그리고 류마티스 인자 는 정상 범위였다. 대변 및 혈액 기생충검사에서 모두 음성 소견이 었다.
방사선학적 검사: 입원 당시 단순 흉부, 복부 X선 검사는 정상이 었다. 중증 호산구 증가가 동반되어 호산구 관련 질환의 감별과 호 산구의 장기침범을 확인하기 위하여 저선량 흉부 전산화단층촬영 과 복부 초음파검사를 시행하였으나 이상소견은 없었다. 하지 부 종 감별을 위하여 시행한 자기공명영상(magnetic resonance imag- ing, MRI)에서는 대칭적으로 종아리의 앞쪽과 옆쪽 근막이 강하 게 조영증강이 되었으며 인접한 부위에 지방조직의 침윤이 확인되 었다(Fig. 2A).
조직 검사: 호산구근막염 확진 및 피부경화증과의 감별진단을 위하여 국소 마취 후 우측 종아리 내측에서 전층 피부근육조직 검 사를 시행하였다. 검사 결과 근막 내로 림프구, 형질세포 및 호산구 의 침윤이 관찰되고, 일부 호산구의 탈과립현상과 근막 및 피하지 방층의 부종이 관찰되었다(Fig. 2B).
경과: 조직검사 시행 후 프레드니솔론 1 mg/kg 복용을 시작하여 3개월 동안 유지하였다. 프레드니솔론 복용 3일째부터 부종은 크게 호전되었으나 호산구는 36.6% (절대 호산구 수 4,032/μL) 였다. 2주 후 외래 방문 시 증상은 호전 중으로 호산구는 0.8%로 감소되었다 Fig. 1. The patient’s edematous hands (A) and lower extremities (B) at the initial visit.
A B
Fig. 3. The patient’s hands (A) and lower extremities (B) at 3 month of prednisolone treatment.
A B
A
Fig. 2. (A) Magnetic resonance imaging showed symmetrical thickening and contrast enhancement of the crural fascia of the anterolateral portion of both lower legs with adjacent subcutaneous fat infiltration. (B) A biopsy specimen from the lesion revealed infiltration of the fascia and the septa in subcutaneous fat by eosinophils (arrows), plasma cells, and lymphocytes and marked edema of the fascia and the septa in subcutaneous fat. Eosinophils seemed to be de- granulated (H&E; original magnification: × 400).
B
(Fig. 3). 발등과 발바닥에 보이던 피부의 발적과 경화 병변도 호전되 었다. 프레드니솔론은 2주 간격으로 0.25 mg–0.5 mg/kg으로 감량 을 시도하였고, 총 3개월간 사용 후 중단하였다(Fig. 3). 이후 1–3개 월 간격으로 1년간 추적하였으나 증상의 재발은 없었다.
이 증례는 환자로부터 사진 게재에 대한 동의서를 받았다.
고 찰
호산구근막염은 1974년 Shulman이 고감마글로블린혈증, 말초 혈액 호산구 증가, 혈침 속도 상승, 그리고 조직학적으로 두꺼워지 고 섬유화된 근막을 가진 질환으로 처음으로 기술하였다.1,2 드문 질환이라 유병률은 잘 알려져 있지 않으나 현재까지 모든 연령에서 다양하게 보고된 바 있으며, 여자에서 발생률이 높다. 대부분의 환 자에서 사지의 갑작스런 통증과 부종이 양측성으로 나타난다. 초 기에는 주로 사지 피부의 부종이 나타나지만 병이 진행함에 따라 부종이 사라지고 피부가 오므라지면서 경화성 병변으로 변하여 결 국 피부가 오렌지 껍질 양 변화를 보이게 된다. 이 증례의 환자도 갑 작스러운 부종과 통증을 호소하였고, 발등과 발바닥의 홍반 및 약 간의 경화성 변화와 함께 호산구 증가가 관찰되어 이 질환을 의심 하였다. 본 환자에서는 사지 이외에 침범한 기관은 없었으나 체간 부 병변이 동반되는 경우는 예후가 좋지 않은 것으로 알려져 있으 며, 내장침범도 있을 수는 있으나 드문 것으로 알려져 있다.
임상 증상 발현 전 약 30%–46% 환자에서 격렬한 신체운동이 선 행되는 경우가 많으며 본 환자도 증상 발현 전 수영을 한 적이 있어 운동과의 관련성을 의심하였다. 이외에 스타틴 계열의 약물 복용 력, 보렐리아증과 같은 감염증, 혈소판 감소증, 만성림프구성 백혈 병, 재생불량성 빈혈 등과 같은 혈액학적 이상소견이 함께 나타나거 나 유방암, 전립선암 등의 악성질환, 갑상선 질환이나 쇼그렌병, 루 푸스 등과 같은 자가면역질환과의 연관성이 있다고 하지만 정확한 원인이나 병인 기전에 대해서는 잘 알려져 있지 않다. 조직학적 소 견에서 granzyme B를 포함한 CD8 임파구와 대식세포 등이 근막 에 침윤되고, tissue inhibitor of metalloproteinase-1과 transform- ing growth factor-β의 상승이 동반되어 면역학적 기전에 의한 것으 로 추정되나 병인 기전에 대한 연구가 더 필요한 것으로 보인다.3
확진을 위해서는 본 환자와 같이 근막과 근육을 포함하는 전층 생검이 표준 진단법으로 알려져 있다.4 초기 병변의 조직학적 소견 은 정상 표피와 진피이지만 근막과 피하지방층의 부종과 염증 등이 관찰된다. 병변이 진행할수록 근막은 정상의 2–10배 이상 두꺼워 질 수 있으며, 표피의 경화성 변화와 호산구, 임파구, 형질세포 등의 침윤이 동반된다. 조직의 호산구 침윤이 진단에 도움이 되지만 반 드시 필수적인 것은 아니다.5 Berianu 등6에 따르면, 약 40% 환자에 서는 조직 호산구 침윤이 동반되지 않았다고 하며, 말초혈액 호산 구와의 연관성도 반드시 일치하는 것은 아니라고 보고한 바 있다.
모든 환자에서 조직검사와 같은 침습적인 검사를 시행할 수 없을 경우 영상의학적 검사를 진단에 보조적인 도구로 많이 활용한다.
본 환자의 경우도 MRI를 이용하여 근막의 조영증강 여부를 확인 하고, 조직학적 검사를 위한 위치를 설정하였다. 최근 초음파검사 법으로 호산구근막염의 진단 및 조직검사 부위 확인 및 재발 여부 등을 확인하는 데 활용하기도 한다.7 그 외에 C-reactive protein (CRP), erythrocyte sedimentation rate와 같은 염증지표의 상승이 나 aldolase 상승 여부 등을 혈청학적 검사를 통해 확인해 볼 수 있 으며, CRP 상승은 불량한 예후인자의 하나로 알려져 있기도 하다.1
감별진단으로는 우선 피부경화증을 고려해야 하는데,4 말초혈액 의 호산구 증가증, 피부와 관절 이외의 장기 침범이 거의 나타나지 않는 것, 피부경화증 관련 자가항체 음성, 레이노 현상은 없는 점 등이 호산구근막염과 피부경화증과의 차이점으로 들 수 있으며, 최종적으로는 조직검사를 통하여 확진할 수 있다. 이외에도 말초 호산구 증가를 특징으로 하는 감염질환이나 과호산구증후군, 호 산구증가근육통증후군(eosinophilia-myalgia syndrome) 등의 감 별이 필요하다. 호산구증가근육통증후군은 L-tryptopan 섭취력 과 동반된 근육 경련, 전반적인 근육통, 근위부 근육 약화, 신경병 증 등이 나타나지만 본 환자에서는 그런 소견이 없어서 제외할 수 있었으며, 과호산구증후군을 배제하기 위해 말초혈액도말검사와 장기 내 호산구 침범을 확인하기 위한 흉부 전산화단층촬영 및 복 부 초음파검사를 시행하였으나 이상 소견은 관찰되지 않았다.
진단 기준은 유럽과 미국에서 Table 1과 같이 제시한 바 있다.1,4 주진단기준인 (1) 표피와 진피층의 부종, 경화 및 비후성 병변과, (2) 전층 조직검사에서 근막의 비후와 임파구, 대식세포 및 호산구의 침윤, 부진단기준으로 (1) 호산구가 0.5×109/L 이상, (2) 혈청 총 감 마글로불린이 1.5 g/L 이상, (3) 근력약화 또는 혈청 aldolase 상승, (4) 그루브 사인이나 오렌지 껍질양 변화, (5) MRI T2 강조영상에서 Table 1. Proposed criteria for the diagnosis of patients with eosinophilic fasci- itis1,4
Major criteria
1. Swelling, induration, and thickening of the skin and subcutaneous tissue that is symmetrical or nonsymmetrical, diffuse (extremities, trunk and abdomen) or localized (extremities)
2. Fascial thickening with accumulation of lymphocytes and macrophages with or without eosinophilic infiltration (determined by full-thickness wedge biopsy of clinically affected skin)
Minor criteria
1. Eosinophilia > 0.5× 109/L 2. Hypergammaglobulinemia > 1.5 g/L
3. Muscle weakness and/or elevated aldolase levels 4. Groove sign and/or peau d’orange
5. Hyperintense fascia on magnetic resonance T2-weighted images
Exclusion criteria: diagnosis of systemic sclerosis. Presence of both major criteria, or 1 major criterion plus 2 minor criteria, establishes the diagnosis of eosinophilic fas- ciitis.
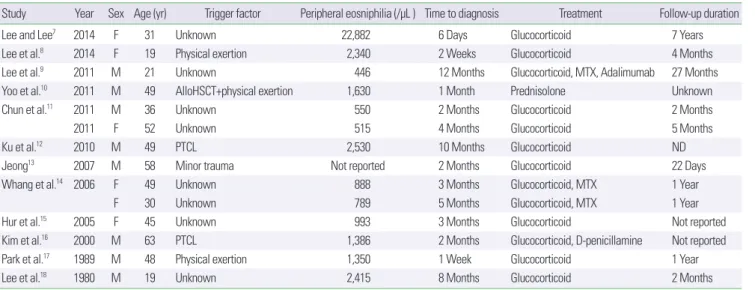
Table 2. Summary of previously reported cases of eosinophilic fasciitis in Korea
Study Year Sex Age (yr) Trigger factor Peripheral eosniphilia (/μL ) Time to diagnosis Treatment Follow-up duration
Lee and Lee7 2014 F 31 Unknown 22,882 6 Days Glucocorticoid 7 Years
Lee et al.8 2014 F 19 Physical exertion 2,340 2 Weeks Glucocorticoid 4 Months
Lee et al.9 2011 M 21 Unknown 446 12 Months Glucocorticoid, MTX, Adalimumab 27 Months
Yoo et al.10 2011 M 49 AlloHSCT+physical exertion 1,630 1 Month Prednisolone Unknown
Chun et al.11 2011 M 36 Unknown 550 2 Months Glucocorticoid 2 Months
2011 F 52 Unknown 515 4 Months Glucocorticoid 5 Months
Ku et al.12 2010 M 49 PTCL 2,530 10 Months Glucocorticoid ND
Jeong13 2007 M 58 Minor trauma Not reported 2 Months Glucocorticoid 22 Days
Whang et al.14 2006 F 49 Unknown 888 3 Months Glucocorticoid, MTX 1 Year
F 30 Unknown 789 5 Months Glucocorticoid, MTX 1 Year
Hur et al.15 2005 F 45 Unknown 993 3 Months Glucocorticoid Not reported
Kim et al.16 2000 M 63 PTCL 1,386 2 Months Glucocorticoid, D-penicillamine Not reported
Park et al.17 1989 M 48 Physical exertion 1,350 1 Week Glucocorticoid 1 Year
Lee et al.18 1980 M 19 Unknown 2,415 8 Months Glucocorticoid 2 Months
alloHSCT, allogeneic hematopoietic stem cell transplantation; MTX, methotrexate; ND, not done; PTCL, peripheral T-cell lymphoma.
근막의 조영증강 소견을 제시하였다. 주진단기준 2개를 만족하거 나 주진단기준 1개와 부진단기준 2개를 만족하면 호산구근막염으 로 진단할 수 있다. 본 환자의 경우 주진단기준 2가지와 호산구증 다증과 MRI 영상 소견의 부진단기준을 만족하였다.
기존에 보고된 국내 증례를 정리해 보니 모두 Table 1의 진단기 준을 만족하였으며, 총 14개의 증례가 확인되었다(Table 2).7-18 국내 에 보고된 환자들은 남자가 여자보다 조금 더 많았으며(남:여=
1.3:1.0), 평균 연령은 40.6±14.6세였다. 진단까지 걸린 시간은 평균 2.5개월로 가장 짧은 경우는 2주였고, 진단이 늦어질수록 스테로이 드 치료 이외에 면역억제제를 사용하는 빈도가 높았다. 면역억제제 를 사용한 4명9,14,16을 제외한 대부분의 환자들은 재발 없이 치료가 종결되었다. 그러나 Mertens 등19이 보고한 호산구성 근막염 환자 35예를 보면, 평균연령이 53세로 높고, 진단까지의 기간이 약 7개월 로 국내 환자들에 비해 약 3배 정도 길었다. 또한, 국내 환자들이 스 테로이드로 대부분 치료가 호전되었던 것에 비해 서양의 환자들은 대부분 면역억제제를 함께 사용하였으며 영구적인 피부섬유화가 후유증으로 대부분 동반되어 국내 환자들의 임상양상과는 차이를 보이고 있다. 이처럼 스테로이드 제제 치료에도 불구하고 증상이 지속되거나, 스테로이드 치료를 중단한 후에 다시 재발하는 경우에 는 methotrexate, cyclosporin, hydroxychloroquine, azathioprine, D-penicillamine 등의 이차적인 약제를 선택할 수 있으며, 최근에 는 infliximab, tocilizumab, rituximab, eculizumab 등의 생물학적 제제를 이용하여 성공적으로 치료한 사례도 보고되고 있다.4 일본 에서 진행된 연구에서는 체간부 병변이 동반되거나 진단 당시 morphea like 피부 병변이 관찰되는 경우 피부섬유화가 지속되는 불량한 예후로 보고하였다.20 그러나 대부분 호산구근막염은 증례 위주의 보고들이므로 호산구근막염 환자들의 장기 추적 결과 및
예후에 대한 추가적인 연구가 필요할 것으로 생각한다.
저자는 전형적인 임상 증상을 보이고 조직검사를 통해서 확진되 었으며 스테로이드 치료에 반응을 보인 호산구근막염 환자를 경험 하여 문헌 고찰과 함께 보고하는 바이다.
REFERENCES
1. Pinal-Fernandez I, Selva-O’ Callaghan A, Grau JM. Diagnosis and classi- fication of eosinophilic fasciitis. Autoimmun Rev 2014;13:379-82.
2. Lakhanpal S, Ginsburg WW, Michet CJ, Doyle JA, Moore SB. Eosinophilic fasciitis: clinical spectrum and therapeutic response in 52 cases. Semin Arthritis Rheum 1988;17:221-31.
3. French LE, Shapiro M, Junkins-Hopkins JM, Wolfe JT, Rook AH. Eosin- ophilic fasciitis and eosinophilic cellulitis in a patient with abnormal cir- culating clonal T cells: increased production of interleukin 5 and inhibi- tion by interferon alfa. J Am Acad Dermatol 2003;49:1170-4.
4. Fett N, Arthur M. Eosinophilic fasciitis: current concepts. Clin Dermatol 2018;36:487-97.
5. Barnes L, Rodnan GP, Medsger TA, Short D. Eosinophilic fasciitis. A pathologic study of twenty cases. Am J Pathol 1979;96:493-518.
6. Berianu F, Cohen MD, Abril A, Ginsburg WW. Eosinophilic fasciitis: clin- ical characteristics and response to methotrexate. Int J Rheum Dis 2015;
18:91-8.
7. Lee JW, Lee JY. A case of eosinophilic fasciitis: imaging findings from early diagnosis to complete remission. J Korean Soc Radiol 2014;71:150-4.
8. Lee HS, Chang SJ, Kang MS, Yoon CS, Kim KW, Sohn MH, et al. A case of eosinophilic fasciitis presenting as pitting edema of the lower extremi- ties. Allergy Asthma Immunol Res 2014;6:179-82.
9. Lee SS, Kim HO, Na JB, Lee JS, Suh YS, Cheon YH, et al. A case of steroid and methotrexate-resistant eosinophilic fasciitis treated with adalimumab.
J Rheum Dis 2011;18:306-10.
10. Yoo IS, Kim MK, Song ST, Kim JH, Kim JM, Jo DY, et al. Eosinophilic fasciitis as the initial manifestation of graft-versus-host disease. J Rheum Dis 2011;18:64-7.
11. Chun JH, Lee KH, Sung MS, Park CJ. Two cases of eosinophilic fasciitis.
Ann Dermatol 2011;23:81-4.
12. Ku KH, Kim HK, Lee HS, Kim GT, Ok CH, Jung MH, et al. Suspicious eosinophilic fasciitis preceding peripheral T cell lymphoma. Korean J Asthma Allergy Clin Immunol 2010;30:233-6.
13. Jeong HJ. Eosinophilic fasciitis localized on the left lower extremity: a case report. J Korean Acad Rehabil Med 2007;31:478-81.
14. Whang YJ, Kim KM, Oh SJ, Jang KY, Lee SI, Yoo WH, et al. Diagnostic availability of ultrasonography and the effects of methotrexate therapy in patients with eosinophilic fasciitis: report of two cases. J Korean Rheum Assoc 2006;13:56-63.
15. Hur JW, Lee HS, Uhm WS, Jun JB, Bae SC, Park CK, et al. Eosinophilic fasciitis associated with autoimmune thyroiditis. Korean J Intern Med 2005;20:180-2.
16. Kim H, Kim MO, Ahn MJ, Lee YY, Jung TJ, Choi IY, et al. Eosinophilic
fasciitis preceding relapse of peripheral T-cell lymphoma. J Korean Med Sci 2000;15:346-50.
17. Park MK, Jeon SJ, Suh KS, Kim ST. A case of eosinophilic fasciitis. Korean J Dermatol 1989;27:729-33.
18. Lee JB, Kim SC, Kim YK. Eoxinophilic FAsciitis: report of a case. Korean J Dermatol 1980;18:361-5.
19. Mertens JS, Thurlings RM, Kievit W, Seyger MMB, Radstake TRD, de Jong EMGJ. Long-term outcome of eosinophilic fasciitis: a cross-sectional evaluation of 35 patients. J Am Acad Dermatol 2017;77:512-7.e5.
20. Endo Y, Tamura A, Matsushima Y, Iwasaki T, Hasegawa M, Nagai Y, et al.
Eosinophilic fasciitis: report of two cases and a systematic review of the literature dealing with clinical variables that predict outcome. Clin Rheu- matol 2007;26:1445-51.