한국 폐경 여성에서 호르몬치료 전후 Leptin계, 골의 생화학적 인자, 골밀도 사이의 연관성
서울대학교 의과대학 산부인과학교실
1, 서울대학교병원 의생명연구원
2김 훈
1․이희준
1․고하늬
2․구승엽
1,2․김석현
1,2․최영민
1,2․김정구
1,2The Association among Serum Leptin System, Bone Biochemical Markers and Bone Mineral Density Before and After Hormone Therapy
Hoon Kim
1, Hee Jun Lee
1, Hanee Koh
2, Seung-Yup Ku
1,2, Seok Hyun Kim
1,2, Young Min Choi
1,2, Jung Gu Kim
1,21
Department of Obstetrics and Gynecology, Seoul National University College of Medicine,
2
Biomedical Research Institute, Seoul National University Hospital, Seoul, Korea
Objectives: To investigate the relationships between serum leptin, soluble leptin receptor (sLR) and bone mineral density (BMD) and bone biochemical markers and to evaluate association among these factors after hormone therapy (HT) in postmenopausal Korean women.
Methods: Serum leptin, sLR, biochemical markers, osteoprotegerin (OPG) and soluble receptor activator of NF-kB ligand (sRANKL) were measured by enzyme linked immunosorbent assay in 159 postmenopausal Korean women. The BMD at the lumbar spine (LS) and femoral neck (FN) was determined by dual energy X-ray absorptiometry, and changes of these factors were also measured in 70 postmenopausal women receiving HT.
Results: After adjustment for age and year since menopause, body mass index (BMI) was found to be significantly correlated with leptin (r=0.42, P<0.0001), sLR (r=-0.24, P<0.005), free leptin index (FLI, r=0.47, P<0.0001) and serum OPG was also correlated with serum leptin (r=-0.24, P<0.005) or sLR (r=-0.16, P<0.05). Serum leptin levels and FLI in obese women (BMI>25 kg/m
2) were significantly higher than those in women with normal weight, whereas sLR levels were lower in the former women than in the latter women. After HT, serum leptin levels (P<0.005) and FLI (P<0.05) decreased significantly and decreased serum sLR levels (P<0.05) was found only in obese women. The percent changes in BMD at FN after HT were negatively correlated with the changes of sLR after HT.
Conclusions: Circulating leptin system is not associated with BMD but BMI. Leptin and FLI decrease after HT and the changes of sLR reflects changes in BMD at FN after HT.
Key Words: Biochemical markers, Bone density, Hormone replacement therapy, Leptin
Received: February 15, 2013 Revised: April 9, 2013 Accepted: April 20, 2013
Corresponding Author: Jung Gu Kim, Department of Obstetrics and Gynecology, Seoul National University Hospital, 28 Yeongeon-dong, Jongno-gu, Seoul 110-744, Korea
Tel: +82-2-2072-3256, Fax: +82-2-762-3599, E-mail: [email protected]
Leptin은 146개의 아미노산을 갖는 펩티드 호르몬 으로 주로 지방세포에서 생산되며 염색체 7q31.3에 위치한 ob 유전자에 코딩되어 있는데, 음식 섭취를 억제하고 에너지 소비를 자극하여 체중조절에 중요 한 역할을 한다고 알려져 있다.
1Leptin은 여러 가지 수용체를 통하여 작용하는데 특히 수용성 수용체 (soluble leptin receptor, sLR)는 leptin과 결합하여 순 환계 내 leptin의 작용을 매개한다.
지방은 연부 조직의 골격에 대한 부하, 췌장 세포 로부터 호르몬 분비, 지방세포로부터 leptin 등의 분 비 등을 통하여 골과 연관성이 있는 것으로 생각되 고 있다.
2,3또한 leptin은 직접적으로 조골세포의 생 산과 분화를 증가시키고 또한 파골세포의 생성을 억 제하는 작용을 하는 반면 뇌의 시상하부에 직접 작 용하여 이와 반대되는 작용을 한다고 알려져 있다.
즉 leptin이 결핍된 생쥐의 뇌실 내로 leptin을 주입할 경우 오히려 골형성이 억제되고 골흡수가 자극되는 데 이는 교감신경계 및 파골세포의 β 교감신경 수 용체(beta adrenergic receptor)를 통하여 이루어진다.
이러한 상반된 두 가지 작용 중 전자의 작용이 강력 하다고 생각되고 있다.
그러나 leptin과 골밀도의 연관성에 대한 임상적 연구는 다양한 결과를 보고하고 있다. 즉 폐경 상태, 체질량지수와 지방의 양 등의 교란인자의 보정 여 부, 인종, 남녀 차이 등에 따라 양성 상관관계를 보 고하는 연구자도 있지만
4-10체질량지수와 지방량 등 의 인자의 보정 후에 연관관계가 없다고 주장하는 연구자도 있다.
11-22그러나 이러한 연구자 대부분이 순환계 내 leptin만을 측정하였고 sLR을 측정하지 않 았다.
폐경 여성에서는 체중 증가 및 체지방의 중심화 등이 일어나는데, 호르몬 치료는 체중 증가를 막거 나 폐경전 상태로 체성분을 부분적으로 회복시킨다 고 보고되고 있다.
23,24한편 사람에서 체질량지수, 피 하지방 양이 혈청 leptin 농도의 가장 중요한 결정인 자라고 생각되고 있는데,
19,20,25-27에스트로겐은 인간 의 피하지방 조직에서 leptin 전령 RNA (mRNA) 생 산을 자극한다.
28따라서 호르몬 치료의 작용이 leptin을 통해 중개될 가능성이 시사되어 혈청 leptin 에 대한 호르몬 치료의 영향에 대한 많은 연구가 진
행되어 왔으나 그 결과는 혈청 leptin의 증가,
29-33무
변화,
26,34-37감소
38-40등으로 다양하게 보고되고 있다.
한편 아직 호르몬 치료 후 leptin 계, 특히 sLR의 변 화와 골량의 변화와의 연관성에 대한 연구는 보고된 바가 없다. 본 연구는 한국 자연폐경 여성에서 leptin, sLR, 골의 생화학적인자, 골량 사이의 연관성을 규 명하고 호르몬 치료 후 이 인자들의 변화 사이의 연 관성을 규명하기 위하여 기획되었다.
대상 및 방법
1. 연구 대상
서울대학교병원의 폐경 클리닉에 방문한 폐경 여 성 중 본 연구의 목적을 충분히 이해하고 동의한 여 성 159명을 대상으로 하였다. 폐경은 양측 난소절제 술의 과거력 없이 마지막 생리가 있은 지 적어도 1 년이 경과된 여성 중 혈청 난포자극호르몬이 40 mIU/mL 이상인 경우로 하였다. 이러한 연구대상자 에서 당뇨병, 간질환, 신장질환 등 급 ․ 만성질환이 있거나 호르몬, 활성비타민 D, 칼시토닌과 같이 골 대사에 영향을 준다고 알려진 약제를 복용한 여성 및 에스트로겐 제제 사용의 절대적 금기사항, 즉 원 인이 확실치 않은 비정상 질출혈, 급성 혈관질환, 유 방암 등이 있는 환자는 제외하였다. 연구 대상자에 게 호르몬치료를 시행하였는데 호르몬은 경구용 접 합 마 에스트로겐(conjugated equine estrogen)인 pre- marin 0.3 mg/일을 매일 투여하고, medroxyprogeste- rone acetate (MPA) 5 mg을 매달 1일에서 12일까지 1 일 1회, 취침 전에 복용하게 하였고 칼슘 1 g을 병행 투여하였다. 6개월 후 골의 생화학적 인자를 측정하 고 1년간 호르몬치료를 하였으며 1년 후 골밀도를 측정한 여성은 모두 70명이었다. 본 연구는 서울대 학교병원 의학연구윤리심의위원회(Institutional Review Board)에서 승인되었다.
2. 혈액 채취 및 체질량지수 측정
헬싱키선언에 의거하여 연구대상자들로부터 상박
부 혈관으로부터 혈액을 항응고제가 들어 있지 않은
튜브에 채취하였다. 이를 원심분리하여 혈청을 모아
서 -70
oC에 보관하였다가 leptin, sLR, 골교체인자
등의 측정에 사용하였다. 키와 체중을 측정하여 체 질량지수(body mass index, BMI (kg/m
2))를 계산하였 다. 비만도에 대해서는 아시아인 기준을 채택하여
41BMI가 25 kg/m
2이상인 경우를 비만으로 정의하였다.
3. 골밀도 측정
연구대상자에서 척추, 대퇴골경부의 골밀도 측정 에 Lunar사(Lunar PPX-L, Medison, Wisconsin, USA) 의 이중에너지 엑스레이 흡수계측기(dual energy X-ray absoptiometry, DXA)를 이용하였다. 이 측정기 의 요추 골밀도 측정에서의 체내 변이계수(in vivo coefficient of variation)는 1.4%, 대퇴골 경부에서는 2.1%이었다. 1년간 호르몬치료를 받은 여성들은 치 료 후 1년에 골밀도를 측정하였다. Kanis 등
42의 정 의에 따라 골감소증은 한국인 젊은 여성의 평균치의 1∼2.5 표준편차의 감소가 있는 경우, 골다공증은 한 국인 젊은 여성의 평균치보다 2.5 표준편차 이상의 감소가 있는 경우에 진단하였고 골감소증과 골다공 증 여성을 저골량여성으로 분류하였다.
4. 혈청 골교체 인자와 OPG 및 sRANKL측정 혈청 osteocalcin (OST)은 ELSA-OSTEO 키트(CIS bio international, France)를 이용하여 면역방사선 측 정법(radioimmunoassay)으로 측정하였다. 측정 민감 도는 0.4 ng/mL이었고 측정 간의 변이는 5.2%, 측정 내 변이는 3.8%이었다. 혈청 bone alkaline phos- phatase (BAP)는 미국 Metra Biosystems사(Mountain View, CA, USA)의 Alkphase-B 키트를 사용하여 면 역측정법으로 측정하였다. 측정 민감도는 0.7 U/L이 었고 측정 간의 변이는 5.2%, 측정 내 변이는 3.9%
이었다. 혈청 CrossLaps (CTX)는 덴마크 Osteometer 사(Osteometer Biotech, Herlev, Denmark)의 혈청 CTX 키트를 사용하여 측정하였다. 측정 민감도는 94 pM 이었고 측정 간의 변이는 5.4%, 측정 내 변이는 5.0%이었다. OPG 측정은 정량적 효소면역키트 (R&D Systems, Minneapolis, USA)를 사용하여 측정 하였다. OPG 측정 민감도는 0.195 ng/mL이었고 측 정 간의 변이는 8.1%, 측정 내 변이는 11.7%이었다.
sRANKL 측정은 독일 Biomedica Gruppe사(Wien, Austria)의 RANKL 효소면역 키트를 사용하여 sRANKL
를 측정하였다. sRANKL 측정 민감도는 0.2 pg/mL이 었고 측정 간의 변이는 7.2%, 측정 내 변이는 3.9%
이었다.
5. 혈청 leptin과 sLR 측정 및 유리 leptin지수 (free leptin index, FLI) 계산
Leptin 측정은 미국 R&D사의 정량적 효소면역키 트를 사용하여 측정하였다. 즉, 생쥐 leptin 항체를 가진 미세판에 검체를 넣어 실온에서 2시간 방치한 후 4회 세척하고 leptin-horseradish peroxidase 결합체 용액을 넣어 실온에서 1시간 반응시켰다. 그 후 3회 세척하고 tetramethylbenzidine 기질용액을 넣어 실온 에서 30분간 반응시킨 후 정지용액을 넣은 다음 450 nm에서의 흡광도를 측정하고 표준곡선에서 농도를 구하였다. Leptin 측정 민감도는 7.8 pg/mL이었고 측 정 간의 변이는 4.2%, 측정 내 변이는 3.0%이었다.
sLR도 미국 R&D사의 정량적 효소면역키트를 사 용하여 측정하였다. 즉 sLR 항체를 가진 미세판 구 멍에 검체를 넣고 실온에 있는 진탕기 위에서 2시간 반응시킨 후 4회 세척하였다. 진탕기 위에서 leptin- horseradish peroxidase 결합체 용액을 넣어 실온에서 2시간 반응시켰다. 그 후 4회 세척하고 tetramethyl- benzidine 기질용액을 넣어 실온에서 30분간 반응시 킨 후 정지용액을 넣은 다음 450 nm에서의 흡광도 를 측정하고 표준곡선에서 농도를 구하였다. sLR측 정 민감도는 0.02 ng/mL이었고 측정 간의 변이는 5.3%, 측정 변이는 4.9%이었다. FLI는 혈청 leptin 농 도를 혈청 sLR 농도로 나누어서 계산하였다(ng/ng).
6. 통계분석
모든 자료는 평균±표준오차(mean±standard error,
SE)로 표시하였고 모든 통계 분석은 SPSS 19.0
(SPSS inc, Chicago, Illinois)을 사용하였다. 호르몬 치
료 전 leptin계, 골의 생화학적 인자의 비교에는
student t-검사, 호르몬 치료 후 변화 비교에는 paired
t-test를 사용하였다. 호르몬 치료 전 leptin계 인자,
골의 생화학적 인자, 골밀도 사이의 연관성에는 단
순회귀분석법을 사용하여 Pearson 상관계수를 구하
였으며 또한 연관성이 있는 경우에는 연령, 폐경기
간, 체질량지수를 보정한 편상관분석법(partial corre-
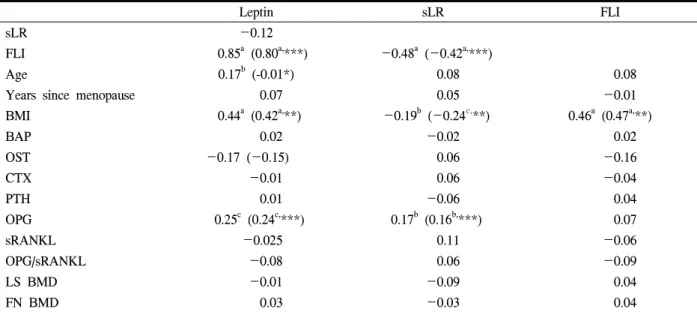
Table 1. Correlation coefficients between demographic data, leptin system, bone biochemical markers, and bone mineral density (n=159)
Leptin sLR FLI
sLR -0.12
FLI 0.85
a(0.80
a,***) -0.48
a(-0.42
a,***)
Age 0.17
b(-0.01*) 0.08 0.08
Years since menopause 0.07 0.05 -0.01
BMI 0.44
a(0.42
a,**) -0.19
b(-0.24
c,**) 0.46
a(0.47
a,**)
BAP 0.02 -0.02 0.02
OST -0.17 (-0.15) 0.06 -0.16
CTX -0.01 0.06 -0.04
PTH 0.01 -0.06 0.04
OPG 0.25
c(0.24
c,***) 0.17
b(0.16
b,***) 0.07
sRANKL -0.025 0.11 -0.06
OPG/sRANKL -0.08 0.06 -0.09
LS BMD -0.01 -0.09 0.04
FN BMD 0.03 -0.03 0.04
sLR, soluble leptin receptor; FLI, free leptin index BMI, body mass index; BAP, bone alkaline phosphatase; OST, osteocalcin; CTX, CrossLaps; PTH, parathyroid hormone; OPG, osteoprotegerin; sRANKL, soluble receptor activator for nuclear factor-kappa B; LS, lumbar spine; FN, femoral neck
P value by correlation analysis and partial correlation analysis
a
P<0.0001,
bP<0.05,
cP<0.001
*adjusted for BMI, **adjusted for age, and years since menopause, ***adjusted for age, and years since menopause, and BMI
lation analysis)으로 분석하였다. 모든 통계학적 분석 에서 P<0.05인 경우만 유의하게 판정하였다.
결 과
1. Leptin계, 골의 생화학적 인자, 골량 사이의 연관성
Table 1은 인류학적 인자, leptin계, OPG-sRANKL 계, 골교체인자, 골밀도 사이의 연관성을 보여주고 있다. 즉 leptin은 연령(r=0.17, P<0.05), 체질량지수 (r=0.44, P<0.0001), osteocalcin (r=0.17, P<0.05), OPG (r=0.25, P<0.005)와 연관성이 있었고 sLR도 체질량 지수(r=-0.19, P<0.05), OPG (r=0.15, P<0.05)와 상 관관계가 있었으며 FLI는 체질량지수(r=0.46, P<
0.0001)만 상관관계가 있었다. 이 중 체질량지수는 연령, 폐경기간을 보정한 후에도 leptin (r=0.42, P<
0.0001), sLR (r=-0.24, P<0.005), FLI (r=0.47, P<
0.0001)의 연관성이 유지되었다. 골의 생화학적 인자
는 연령, 폐경기간, 체질량지수를 보정한 후에 OPG 와 leptin (r=-0.24, P<0.005) 또는 sLR (r=-0.16,
P<0.05) 사이의 연관성이 유지되었으나 체질량지수를 보정 후에 leptin과 연령 사이의 연관성은 사라졌 다.
체질량지수를 정상체중여성과 비만여성으로 구분
하였을 때 대퇴골 경부, 요추에서의 골밀도, 혈청
BAP, OST, CTX 농도, 혈청 OPG, SRANKL 농도 및
그 비가 비만여성군(25 kg/m
2이상)에서 높았으나 유
의한 차이는 보이지 않았다. 비만여성에서 혈청
leptin 농도는 12.3±0.8 ng/mL로 정상체중여성(25
kg/m
2미만)의 7.9±0.8 ng/mL보다 유의하게 높았고
(P<0.0001) FLI도 전자에서 0.44±0.04로 후자의
0.12±0.02보다 유의하게 높았으나(P<0.0001) sLR의
경우에는 비만여성군에서 32.1±1.55 ng/mL로 정상
체중여성의 36.8±1.0 ng/mL보다 유의하게 낮았다
(P<0.0001, Table 2). 정상체중여성과 비만여성군 모
두에서 골량 상태에 따른 이러한 leptin계 인자들의
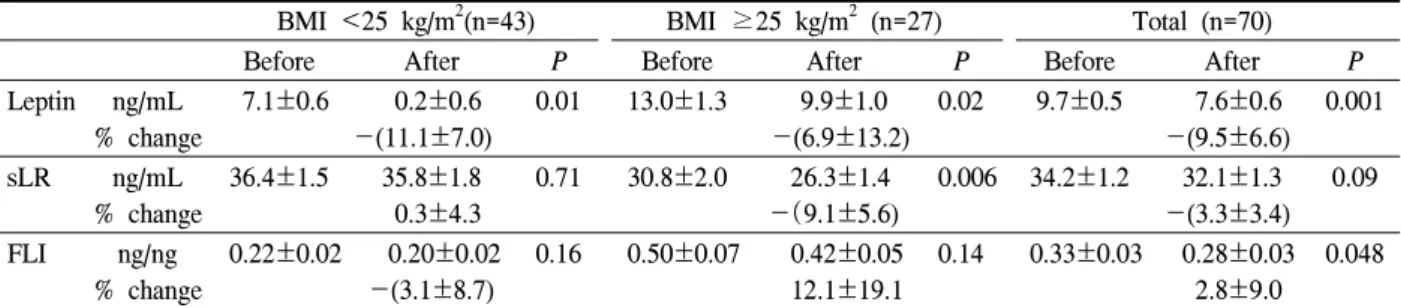
Table 3. Serum leptin, soluble leptin receptor (sLR) levels and free leptin index (FLI) before and after 6months HT according to BMI
BMI <25 kg/m
2(n=43) BMI ≥25 kg/m
2(n=27) Total (n=70)
Before After P Before After P Before After P
Leptin ng/mL
% change
7.1±0.6 0.2±0.6 -(11.1±7.0)
0.01 13.0±1.3 9.9±1.0 -(6.9±13.2)
0.02 9.7±0.5 7.6±0.6 -(9.5±6.6)
0.001
sLR ng/mL
% change
36.4±1.5 35.8±1.8 0.3±4.3
0.71 30.8±2.0 26.3±1.4 -(9.1±5.6)
0.006 34.2±1.2 32.1±1.3 -(3.3±3.4)
0.09
FLI ng/ng
% change
0.22±0.02 0.20±0.02 -(3.1±8.7)
0.16 0.50±0.07 0.42±0.05 12.1±19.1
0.14 0.33±0.03 0.28±0.03 2.8±9.0
0.048
P value by paired t-test.
Table 2. Serum leptin, soluble leptin receptor (sLR) levels and free leptin index (FLI) in postmenopausal women according to BMI and status of bone mass
BMI <25 kg/m
2BMI ≥25 kg/m
2Normal BMD (n=29)
Lower bone
mass (n=72) Total (n=101) Normal BMD (n=18)
Lower bone
mass (n=40) Total (n=58) Leptin (ng/mL) 7.1±0.6
a8.2±0.7
b7.9±0.8
c10.4±1.3
a13.1±0.9
b12.3±0.8
csLR (ng/mL) 35.4±1.4 37.3±1.3
d36.8±1.0
e32.7±4.2 31.9±1.3
d32.1±1.55
eFLI (ng/ng) 0.21±0.02
f0.24±0.02
g0.22±0.02
h0.38±0.06
f0.47±0.05
g0.44±0.04
hBMI, body mass index; BMD, bone mineral density
P value by t-test.
a,d,f
P<0.05,
b,c,e,g,hP<0.0001
차이가 없었다.
2. 호르몬 치료 후 leptin계, 골의 생화학적 인 자, 골량 변화 사이의 연관성
6개월간 호르몬 치료 후 순환계 내 골교체인자 및 OPG, sRANKL의 유의한 변화가 없었으나 혈청 leptin 농도는 호르몬 치료 후 7.6±0.6 ng/mL로 치료 전의 9.7±0.5 ng/mL보다 유의하게 감소하였고(P<
0.005) 정상체중군과 비만여성군으로 나누어 분석하 였을 때에도 동일한 현상을 보였다(Table 3). FLI도 호르몬 치료 후 감소하였으나(P<0.05) sLR의 경우 는 비만여성에서만 감소현상을 보였다(P<0.01).
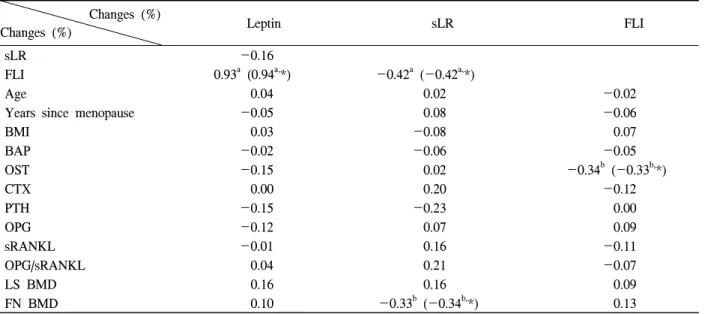
Table 4는 호르몬 치료 6개월 후 leptin계와 골의 생화학적 인자의 변화 및 1년 후 골밀도 변화 사이 의 연관성에 대한 상관관계를 보여주고 있다. 호르 몬 치료 6개월 후 FLI의 변화는 osteocalcin 변화 (r=-0.34, P<0.05)와 연관성이 있었고 sLR의 변화는 1년 후 대퇴골 경부의 골밀도 변화와 음성 상관관계
에 있었으며(r=-0.33, P<0.05) 이들 사이의 연관성 은 연령, 폐경기간, 체질량지수를 보정한 후에도 유 지되었으나 leptin계 인자들 사이의 연관성을 제외한 다른 인자들 사이에는 연관성은 없었다.
고 찰
본 연구에서 체질량지수가 순환계 내 leptin계, 즉 leptin, sLR, FLI와 관련된 가장 중요한 인자라는 것 이 확인되었다. 이제까지의 연구에서는
19,20,25-27leptin
만을 측정하여 지방 양과 체질량지수와의 상관성을
보였던 반면 본 연구는 sLR, FLI 또한 체질량지수와
의 연관성을 보인 최초의 연구이다. 더욱이 체질량
지수 25 kg/m
2이상을 비만으로 간주하여 분석시 비
만여성에서 혈청 leptin과 sLR이 정상체중여성에 비
하여 증가하였고, FLI는 감소하였다. 이러한 체질량
지수와는 대조적으로 연령의 경우에는 체질량지수
를 보정하였을 때 leptin과의 연관성이 사라졌다. 이
Table 4. Correlation coefficients between demographic data, changes (%) of leptin system and bone biochemical markers after 6 months of hormone therapy and changes (%) of bone mineral density after 1year of hormone therapy (n=70)
Changes (%)
Changes (%) Leptin sLR FLI
sLR -0.16
FLI 0.93
a(0.94
a,*) -0.42
a(-0.42
a,*)
Age 0.04 0.02 -0.02
Years since menopause -0.05 0.08 -0.06
BMI 0.03 -0.08 0.07
BAP -0.02 -0.06 -0.05
OST -0.15 0.02 -0.34
b(-0.33
b,*)
CTX 0.00 0.20 -0.12
PTH -0.15 -0.23 0.00
OPG -0.12 0.07 0.09
sRANKL -0.01 0.16 -0.11
OPG/sRANKL 0.04 0.21 -0.07
LS BMD 0.16 0.16 0.09
FN BMD 0.10 -0.33
b(-0.34
b,*) 0.13
sLR, soluble leptin receptor; FLI, free leptin index BMI, body mass index; BAP, bone alkaline phosphatase; OST, osteocalcin; CTX, CrossLaps; PTH, parathyroid hormone; OPG, osteoprotegerin; sRANKL, soluble receptor activator for nuclear factor-kappa B; LS, lumbar spine; FN, femoral neck
P value by correlation analysis and partial correlation analysis
a
P<0.0001,
bP<0.001
*adjusted for age, and years since menopause, and BMI
는 혈청 leptin과 연령 사이에 연관성이 없다고 보고 한 Panidis 등
27과 Iwamoto 등
13과의 연구 결과와 일 치하였다.
Leptin은 시상하부에 있는 수용체를 작용하여 교감 신경계를 통하여 골형성의 억제 작용과 말초적으로 는 골형성 촉진 및 골흡수 억제 작용 등의 상반된 작용이 있다고 알려져 있어
3골과의 연관성이 강력 히 시사되나 인간에서 골밀도와 혈청 leptin의 연관 성에 대하여는 골밀도 측정 부위에 따라 다양한 관 계가 보고되었다. 본 연구에서는 교란인자를 보정 전 및 보정 후에도 요추 및 대퇴골 경부 골밀도와 연관성이 없었는데 이는 골밀도와 leptin 사이에 연 관성이 없다고 보고한 연구들의 결과와 일치하였
다.
11-22,43또한 골밀도 상태에 따른 혈청 leptin 농도
의 차이를 관찰하지 못하였는데 이러한 결과들은 leptin이 골세포에 직접 작용하기보다는 체지방 등을 통하여 골에 작용할 것이라는 것을 시사한다. 한편 leptin과 골밀도 사이에 양성 연관성을 주장하는 연
구자도 상당수 있다. Rancho Bernardo 연구에 의하면
9연령, 체질량지수 등 다른 인자를 교정 후 혈청
leptin은 요추, 대퇴골경부, 골반에서의 골밀도와 연
관성이 있었다고 하였다. Szalay 등은 일차성 담도
경화증(primary biliary cirrhosis)을 가진 폐경여성에
서 체질량지수 보정후 혈청 leptin과 대퇴골 경부에서
의 Z 점수와 연관성이 있었다고 하였으며
7Thomas
등도 혈청 leptin과 요추, 요골 원위부, 골반에서의
골밀도와 연관성을 보고하였다.
8Yamauchi 등은 일
본 폐경여성에서 혈장 leptin과 대퇴골 경부에서의
골밀도와 연관성이 있으며 척추 골절이 있는 여성에
서 혈장 leptin 농도가 낮다고 보고하였다.
10Sherk 등
은 대퇴골 경부와 혈청 leptin 사이의 연관성은 연령
군에 따라 다르다고 하였고
6Jen 등은 백인여성에서
요추 골밀도와 혈청 leptin 사이에 연관성이 있었던
반면 흑인여성에서는 연관성이 없었다고 하여 인종
에 따라 다른 결과를 보고하였으며
5Di Carlo 등은
초기 폐경기에는 연관성이 있다가 폐경기간이 경과
함에 따라 그 연관성이 사라진다고 주장하였다.
4이 러한 다양한 결과는 체질량지수, 지방 양 등의 교란 인자의 보정 여부, 폐경 여부, 연령 차이, 성별 차이 등에 기인할 수 있다. 특히 성별에 따라서 여성의 경 우 남성보다 순환계 leptin 농도가 높다고 보고된 바 있다.
2골의 생화학적 인자의 경우 일부 연구자들이 혈청 BAP,
20NTX,
8,9CTX
33농도와 혈청 leptin 사이에 연 관성이 있어 leptin이 골형성 또는 골흡수의 지침자 역할을 할 수 있다고 주장하였으나 본 연구에서는 골밀도에서와 마찬가지로 혈청 OST, BAP, CTX 농 도 등의 골교체 인자들과 연관성이 없었는데 이는 leptin이 다양한 골교체 인자와 연관성이 없다고 주 장한 대부분의 연구자들의 결과와 일치한다.
8,10,12,13,19,21,22,43
한편 혈청 OPG는 혈청 leptin과 양성 상 관관계에 있었고 혈청 sLR과는 음성 상관관계에 있 음을 관찰하였는데 이러한 소견은 골에서 leptin은 RANKL와 결합하는 OPG를 증가시켜 파골세포의 활 성을 감소시켜서 골을 보존한다고 한 Legiran과 Brandi 등
1의 주장과 일치한다. 그러나 본 연구에서 는 비만여성과 정상체중 여성 사이에 혈청 OPG, sRANKL 농도의 차이를 관찰하지 못하였다.
폐경여성에서는 폐경전 여성에 비하여 혈청 leptin 농도가 낮음,
5높음,
6,18,25차이가 없음
36,37등으로 다 양한 결과가 보고되었다. 본 연구에서 호르몬 치료 를 6개월 시행한 경우 혈청 leptin은 비만 여부에 관 계없이 감소하였는데 이는 경구용 estradiol/norethi- sterone acetate를 3~6개월 사용 후 leptin 농도가 감 소하였다고 한 결과와
26,40경피 estradiol/norgestrel를 2년간 투여한 군에서 호르몬 치료를 시행하지 않은 군에 비해 혈청 leptin 농도가 낮았다고 보고한 Di Carlo 등
38의 결과와 일치한다. 이러한 소견들은 폐 경이 되면 여성호르몬 결핍에 의한 체지방의 증가가 일어나는데 호르몬 치료시 체지방의 증가를 막아서 leptin이 감소되었다고 가정될 수 있다. 그러나 호르 몬 치료 후 체질량지수의 유의한 변화는 관찰되지 않았다. 또한 다양한 호르몬 치료 후 혈청 leptin 농 도에 대해서는 증가,
29-33무변화
26,34-37를 보고한 연구 자들도 있다. 이러한 다양한 결과들은 호르몬 치료 의 투여방법, 유형, 용량 및 프로게스토겐 추가유무,
치료 중 체질량지수와 체성분의 변화, 연구대상군의 이질성, 채혈 시기의 차이에 기인할 수 있다. 특히 leptin은 시간에 따라 파동성 분비를 하는 것으로 알 려져 있다.
44본 연구에서는 상술한 연구자들과 달리 sLR를 같 이 측정하였고 호르몬치료 후 순환계 leptin계와 골 밀도 변화율 사이의 연관성을 분석하였는데 비만여 성에서 호르몬 치료 후 혈청 sLR이 감소하였고 이러 한 sLR 변화율과 호르몬 치료 후 1년에서의 대퇴골 경부에서 골밀도 변화율과 음성상관관계에 있음을 최초로 관찰하였다. 이는 호르몬 치료 후 6개월 시 점에 sLR 측정이 1년 후 대퇴골 경부에서의 골반응 도 예측에 사용할 수 있을 가능성을 제시한다. 실제 로 Jurimae 등
45은 노인여성에서 leptin이 1년 후 대퇴 골 경부에서의 골밀도 손실과 연관성이 있음을 보고 한 바 있다.
본 연구의 제한점으로는 연구대상자 수가 적고, 체지방대신에 체질량지수만 측정하였고 대상군에서 식이 섭취에 대한 정보가 없으며 호르몬치료도 CEE/MPA 한가지만을 사용하였다는 점 등이 있다.
향후 더욱 더 많은 연구대상자에서 이러한 결점을 교정한 대규모 연구가 필요하다고 사료된다.
참 고 문 헌