Address reprint requests to Geun-Yeol Jo, M.D., Ph.D.
Department of Rehabilitation Medicine, Haeundae Paik Hospital, Inje University College of Medicine 875, Haeun-daero, Haeundae-gu, Busan, Korea
TEL: 82-51-797-3250, FAX: 82-51-797-0298, E-mail: [email protected]
투고일: 2014년 8월 13일, 1차 수정일: 2014년 10월 10일, 2차 수정일: 2014년 11월 17일, 게재확정일: 2014년 11월 17일
INTRODUCTION
The etiological factors that result in sciatic nerve injury include insidious and traumatic causes. Insidious causes include mass lesions and metabolic syndrome.
However, traumatic causes occur in association with musculoskeletal injury, such as hip fracture or disloca- tion, direct trauma, improper positioning or immobiliza- tion during surgical procedures, and anesthesia. Lower extremity nerve entrapment is a rare postoperative com- plication.1 Common peroneal neuropathy is a relatively
common neurological complication related to body position during surgery, but sciatic nerve neuropathy related to surgical positioning is rare.2Only a few cases of sciatic neuropathy following surgical procedures in the sitting or lithotomy position have been reported in the foreign literature. Here, we report the first case of the clinical manifestations, electrodiagnostic findings, and injury mechanism of unilateral acute sciatic nerve palsy following a surgical procedure in the semi- Fowler’s position.
반화울러씨자세로 회전근개 수술을 시행한 후에 발생한 좌골신경 마비
1인제대학교 해운대백병원 재활의학과, 2울산세민병원
신민하
1∙조근열
1∙김우진
1∙최희은
1∙이미은
1∙도환권
1∙박상옥
2– Abstract –
Sciatic Nerve Palsy after Semi-Fowler’s Position during the Rotator Cuff Operation
Min-Ha Shin, M.D.
1, Geun-Yeol Jo, M.D., Ph.D.
1, Woo-Jin Kim, M.D.
1,
Hee-Eun Choi, M.D.
1,Mi-Eun Lee, M.D.
1, Hwan-Kwon Do, M.D.
1, Sang-Ok Park, M.D.
21Department of Rehabilitation Medicine, Haeundae Paik Hospital, Inje University College of Medicine
2Ulsan Semin Hospital
Sciatic neuropathy following surgery performed in the hip flexed position is uncommon and has been dis- cussed in only a few published case reports, particularly in the sitting position. We report a very rare case of unilateral sciatic neuropathy after a right rotator cuff operation under general anesthesia in the semi- Fowler’s position. Awareness by surgeons of sciatic nerve injury during surgery in the semi-Fowler’s posi- tion may prevent such intraoperative complications.
Key Words: sciatic neuropathy, intraoperative complications, electromyography
CASE REPORT
A 36-year-old male patient visited the outpatient clinic with pain in his left buttock and weakness in the left ankle, which developed after a right shoulder operation 1 month ago at a local clinic. Due to persistent ankle weakness, he was referred to our rehabilitation clinic 38 days after symptom onset. His body weight and height were 100 kg and 167 cm, respectively. He was obese with a body mass index of 35.8 kg/m2(normal range, 20~25 kg/m2). His medical and family histories revealed no evidence of hereditary neuropathy with liability to pressure palsies.
The operation record described a right rotator cuff repair in the semi-Fowler’s position under general anes- thesia for 3 hr. Weakness and hypoesthesia of his left ankle were noticed immediately after recovery from anesthesia. Direct tenderness on his left buttock without evidence of trauma was observed on physical examina- tion. The manual muscle test revealed that left knee extension strength was 5/5, whereas flexion was 2/5, and left ankle dorsiflexion, plantar flexion, and left long toe extension was 0/5 on the Medical Research Council scale. Muscle strength in all right lower extremity mus- cles was 5/5. Sensation to light touch and pinprick below the left knee had decreased, except for the medial calf area (saphenous nerve distribution). The left knee and ankle reflexes were absent, but normal reflexes were detected on the right side. Pathological reflexes were negative.
An electrodiagnostic examination was performed 40 days after symptom onset using Viking Select electrodi-
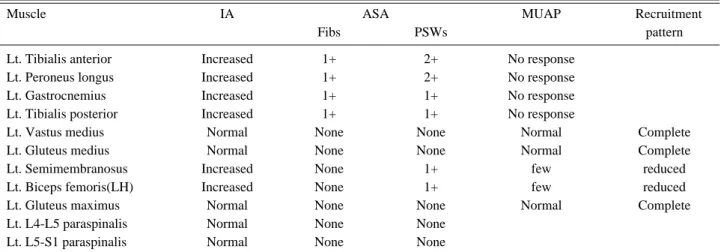
agnostic equipment (Nicolet, San Carlos, CA, USA). We referred to the normal data and the examination tech- nique of a nerve conduction study in Dumitru, 2nd edi- tion.3Compound action potentials (CMAPs) of the left common peroneal nerve were absent in a nerve conduc- tion study. Further CMAPs of the left posterior tibial nerve revealed prolonged distal latency, slightly decreased conduction velocity, and decreased amplitude compared with those on the opposite side. Sensory nerve action potentials (SNAPs) of the left superficial peroneal nerve and sural nerve were absent, whereas the right superficial peroneal and sural nerves evoked SNAPs within the normal range (Table 1). No somatosensory evoked potentials were observed by the left posterior tib- ial nerve. Needle electromyography (EMG) of the left lower limb revealed marked denervation in the left tib- ialis anterior, peroneus longus, gastrocnemius medial head and tibialis posterior muscles. And motor unit action potentials (MUAPs) were not induced on volition in the same muscles. There was increased insertional activity with reduced recruitment of MUAPs in the left semimembranosus and biceps femoris long head mus- cles. No abnormalities were observed in the quadriceps, gluteal, or paraspinal muscles (Table 2).
A contrast-enhanced magnetic resonance imaging (MRI) scan performed 43 days after the onset of symp- toms showed no evidence of a mass, such as tumor or hematoma, that could compress the nerve, but revealed swelling and enhancement of the left sciatic nerve on the buttock and upper thigh area on the T2-weighted coronal and axial views (Fig. 1).
After considering all data, such as those from physical
– 81 – Table 1. Results of Nerve Conduction Studies
Nerve Onset latency (ms) Amplitude (mV) Velocity(m/s)
Motor
Rt. peroneal(EDB recording) 4.0 6.0 47
Lt. peroneal(EDB recording) NP NP NP
Rt. Tibial(AH recording) 3.5 26.1 44
Lt. Tibial(AH recording) 4.5 2.6 40
Sensory
Rt. superficial peroneal 3.2 15
Lt. superficial peroneal NP NP
Rt. sural 3.2 15
Lt. sural NP NP
Rt. saphenous 2.4 6
Lt. saphenous 2.8 5
Rt: right, EDB: extensor digitorum brevis, Lt: left, NP: no potential, AH: abductor hallucis
examinations, an electrodiagnostic examination, and MRI, he was diagnosed with severe left sciatic neuropa- thy. The patient underwent a rehabilitation program, including strengthening exercises for the knee flexors ankle dorsiflexors, and plantar flexors. He also had elec- trical stimulation therapy over the left tibialis anterior, peroneus longus, and gastrocnemius muscles. No inter- val changes in motor or sensory functions were observed 1 month later. A follow-up nerve conduction study (NCS) still revealed no CMAPs from the left common peroneal nerve or SNAPs from the left superficial per- oneal, sural, medial, or lateral plantar nerves. However, a few polyphasic motor unit action potentials and partial interference patterns were observed on a needle EMG study of the left biceps femoris long head, suggesting some regeneration of the left sciatic nerve.
DISCUSSION
Sciatic neuropathy occurring as a neurological compli- cation after surgery is less well recognized than common peroneal neuropathy. In this case, the patient underwent a right rotator cuff operation in the semi-Fowler’s posi- tion and then the left-sided sciatic neuropathy occurred.
Unilateral neuropathy might be meaningful if the patient was seated in an upright position with the same bilateral leg position. Although the operation record described that the right rotator cuff repair was done in the semi- Fowler’s position, the semi-Fowler’s position is usually modified during most rotator cuff operations so patients are in a slightly lateral decubitus position for better visi- bility. Then, the opposite operation site becomes the dependent position. The opposite operative site on the Fig. 1. (A) Axial fat-supressed T2-weighted pelvic MRI shows the enlarged enhancing of the left sciatic nerve (arrow). (B) Coronal fat-suppressed T2-weighted pelvic MRI shows swelling with high signal intensity on the left sciatic nerve (arrow).
A B
Table 2. Results of Needle Electromyography
Muscle IA ASA MUAP Recruitment
Fibs PSWs pattern
Lt. Tibialis anterior Increased 1+ 2+ No response
Lt. Peroneus longus Increased 1+ 2+ No response
Lt. Gastrocnemius Increased 1+ 1+ No response
Lt. Tibialis posterior Increased 1+ 1+ No response
Lt. Vastus medius Normal None None Normal Complete
Lt. Gluteus medius Normal None None Normal Complete
Lt. Semimembranosus Increased None 1+ few reduced
Lt. Biceps femoris(LH) Increased None 1+ few reduced
Lt. Gluteus maximus Normal None None Normal Complete
Lt. L4-L5 paraspinalis Normal None None
Lt. L5-S1 paraspinalis Normal None None
IA: insertional activity, ASA: abnormal spontaneous activity, MUAP: motor unit action potential, Fib: fibrillation, PSW: positive sharp wave, Lt: left, LH: long head
– 83 – body would have more pressure and compression than the actual operation site, which may have caused the uni- lateral sciatic nerve lesion in this case.
The precise mechanism of sciatic nerve injury follow- ing surgery in the semi-Fowler’s position is not well known. Prolonged pressure in the sitting position during surgery can lead to muscle trauma and a resulting spasm of the piriformis muscle, causing sciatic compression, as described by Brown et al.1All previously reported cases of sciatic neuropathy after surgery in the sitting position involved lengthy operation times more than 9 hours1,2,4,5; however, it took only 3 hours for sciatic neuropathy to occur in this case. The subjects of previous cases were children from 10~17 years old. Their thin body habitus and the prolonged surgery duration were predisposing factors for sciatic compressive palsy.2A thin body habi- tus increases susceptibility of the sciatic nerve to com- pression injuries at the level of the ischial tuberosity dur- ing prolonged surgery in the sitting position. The patient in this case was obese and was in the semi-Fowler’s position for only 3 hours during surgery. The left sciatic nerve was swollen, asymmetrically enlarged, and enhanced just after the region where the sciatic nerve passes through the distal portion to the piriformis mus- cle. Thus, the nerve injury was thought to have been caused by a heavy load.
The mechanism of sciatic neuropathy after lying in a particular position during surgery is not clear, but two hypotheses have been proposed. One is sciatic nerve ischemia due to compression and the other is an over- stretching injury. Brown et al. and Poppi et al. reported bilateral sciatic neuropathy and gluteal compartment syndrome or piriformis syndrome due to compression in the sitting position during surgery.1,4 Gozal and Pomer- anz reported sciatic neuropathy as a consequence of tear- ing blood vessels, the epineurium, the perineurium, and intrafunicular tissue due to overstretching.5,6 Moreover, other possible risk factors for perioperative neuropathy, such as obesity, old age, smoking, alcohol, diabetes, vas- cular disease, anatomic anomalies, and long operative time have been reported.2,6-8
Overstretching of the sciatic nerve may be more sus- ceptible to positions of excess external hip rotation dur- ing a hip flexed state or excess hip flexion during the knee fully extended state because the sciatic nerve is fixed between the ischial notch and the fibular head.7In this case, the patient had a slightly flexed hip and knee position, and sciatic neuropathy occurred on the left side
even though the bilateral leg position was the same.
Moreover, the sciatic nerve injury was not extensive in this case. This is consistent with a report by Wang et al.
stating that the injury should be considerably more extensive if the sciatic nerve injury was the result of overstretching.2Therefore, overstretching is less likely in this case, which makes compression the more likely mechanism.
Compression is thought to be the mechanism for sciat- ic neuropathy in patients placed in the semi-Fowler’s position, but we emphasize that the semi-Fowler’s posi- tion, which is a less flexed position than a sitting posi- tion, can also cause sciatic neuropathy. Strategies should be considered to avoid neurological insult to the sciatic nerve, such as preventing sciatic nerve compres- sion by limiting hip flexion angle and carefully placing padding beneath the buttocks to redistribute weight from the ischial tuberosity and posterior compartment of the thigh muscle where the nerve is vulnerable to com- pression during a prolonged operation. Pre-operative management and positioning should be provided to patients who have predisposing factors, even for a short duration surgery.
REFERENCES
1. Brown JA, Braun MA, Namey TC: Piriformis syndrome in a 10-year-old boy as a complication of operation with the patient in the sitting position. Neurosurgery 1988:23:117- 119
2. Wang JC, Wong TT, Chen HH, Chang PY, Yang TF:
Bilateral sciatic neuropathy as a complication of cranioto- my performed in the sitting position: Localization of nerve injury by using magnetic resonance imaging. Childs Nerv Syst 2012:28:159-163
3. Dumitru D, Amato AA, Zwarts MJ: Lumbosacral plex- opathies and proximal mononeuropathies. In: Dumitru D, Zwarts MJ editors. Electrodiagnostic Medicine, 2nd ed, Philadelphia: Hanley & Belfus, 2002. pp871-872.
4. Poppi M, Giuliani G, Gambari PI, Acciarri N, Gaist G, Calbucci F: A hazard of craniotomy in the sitting position:
the posterior compartment syndrome of the thigh. J Neuro- surg 1989:71:618-619
5. Gozal Y, Pomeranz S: Sciatic nerve palsy as a complica- tion after acoustic neurinoma resection in the sitting posi- tion. J Neurosurg Anesthesiol 1994:6:40-42
6. Warner MA, Warner DO, Harper CM, Schroeder DR, Maxson PM: Lower extremity neuropathies associated
with lithotomy positions. Anesthesiology 2000:93:938- 942
7. Reinstein L, Eckholdt JW: Sciatic nerve compression by preexisting heterotopic ossification during general anes-
thesia in the dorsal lithotomy position. Arch Phys Med Rehabil 1983:64:65-68
8. Parks BJ: Postoperative peripheral neuropathies. Surgery 1973:74:348-357