관련 문서
Selective fascicular involvement of median nerve in carpal tunnel syndrome (CTS) has been reported, such as predominant involvement of volar-radially located motor and
Key Words : Carpal tunnel syndrome, Hand configuration, Hand dimensions, Median nerve, Electrodi- agnositc evaluation.. Address reprint requests to Young
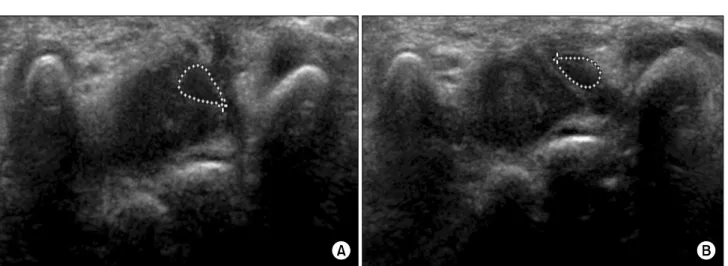
Increased signal with proximal swelling and distal flattening of the median nerve were seen in all patients of carpal tunnel syndrome.. Among the eight
Hence, we report an unusual case and surgical outcome of thrombosed persistent median artery with bifid median nerve causing acute carpal tunnel syndrome.. Informed consent
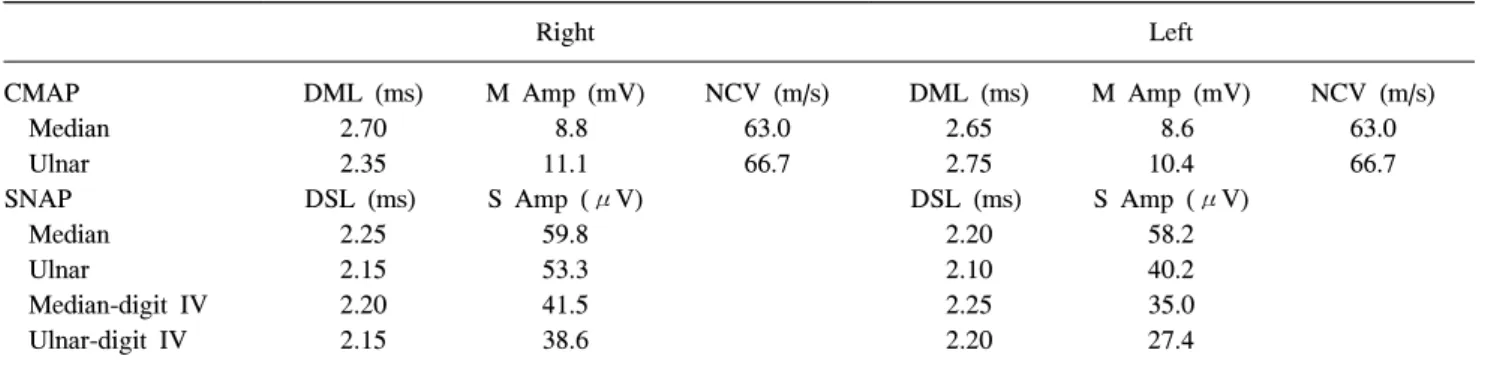
amp.: amplitude, CMAP: compound muscle action potential, CSA: cross-sectional area, CTS: carpal tunnel syndrome, CV: conduction velocity, DM: dia- betes mellitus, lat.: latency,
Box plot showing the median nerve CSAs measured using 3D ultrasonography at the carpal tunnel inlet (left) and the maximal swell- ing point (right) in patients with CTS who
Methods : 20 patients suffering from carpal tunnel syndrome were randomly divided into two groups: 10 subjects treated both with electrical therapy and median
─ CSAa = cross sectional area (CSA) of median nerve proximal to tunnel inlet, CSAb = CSA at pisiform bone level, CSAb-a = area difference between CSAb and CSAa, % area = percentage