대한외과학회지:제 75 권 부록 II
□ 증 례 □
Vol. 75, Suppl. II, December, 2008
451
책임저자: 김용진, 서울시 용산구 한남동 675
140-743, 순천향대학병원 외과 Tel: 02-709-9479, Fax: 02-795-1687 E-mail: [email protected]
접수일:2008년 4월 3일, 게재승인일:2008년 6월 12일
위 소매 절제 및 밴드 성형술 후 발생한 위 협착을 복강경하 하부 위 절제로 치료한 경험
순천향대학교 의과대학 외과학교실
박승완ㆍ김용진
Laparoscopic Assisted Distal Gastrectomy for Gastric Stenosis that was Caused by Laparoscopic Banded Gastroplasty in a Morbidly Obese Patient
Seung Wan Park, M.D., Yong Jin Kim, M.D.
Department of Surgery, Soonchunhyang University School of Medicine, Seoul, Korea
Banded gastroplasty to reduce food intake in patients who are morbidly obese is being increasingly applied in Korea due to its simplicity and low risk. However, the long term results of this procedure are not yet established, and the complications from the band itself are reported to be as high as twenty percent. One of the most disabling complications of banded gastroplasty is persistent vomiting, and this is associated with gastric stenosis. We at- tempted to relieve this discomfort by performing laparoscopic assisted distal gastrectomy and gastrojejunostomy, and we observed good results. (J Korean Surg Soc 2008;75:451-454)
Key Words: Morbid obesity, Vertical banded gastroplasty, Complications 중심 단어: 병적 비만, 수직형 위 밴드 성형술, 합병증
서 론
전세계적인 비만 인구의 증가와 함께, 지난 5년간 대부분 의 선진국에서 비만관련 수술이 5배 이상 증가하였다.(1) 국내의 경우도 2005년 보건 복지부 연구 결과에 따르면 만 20세 이상 성인 비만 유병률이 31.8%로 보고되어, 비만 인 구는 점차 증가 추세에 있다.(2) Sjöström 등(3)과 Adams 등 (4)은, 고도 비만 환자에서 보존요법보다 수술적 처치가 지 속적인 체중 감소와 동반된 합병증의 개선을 통해 장기적 인 사망률을 감소시켰다고 보고하여, 고도 비만의 가장 효 과적인 치료가 수술임을 입증하고 있다.
병적 비만 수술은 기본적인 원칙에 따라, 크게 음식 섭취
를 제한하는 수술과 흡수를 제한하는 수술로 나뉘어진다.
음식섭취를 제한하는 대표적인 방법으로 위 밴드 성형술이 있으며, 이 경우 수술이 간편하고 수술의 위험도가 낮다는 장점이 있으나, 장기적인 결과에서 치료 실패 혹은 합병증 으로 추가적인 처치가 50%에 이르는 문제점이 있는 것으로 알려져 있다.(5) 특히 국내의 경우는 아직 위 밴드 성형술에 대한 결과 보고가 없는 실정이며, 그 문제점에 대한 분석도 이루어 지지 않고 있다. 이에 저자들은 복강경하 위 밴드 성형술 후 위 협착으로 인해 지속적 구토와 정상적인 일상 생활에 심한 장애를 받던 환자에서 복강경하 하부 위 절제 및 위-공장 문합술을 통해 만족할 만한 결과를 얻어 이에 문헌 고찰과 함께 보고하는 바이다.
증 례
30세 여자 환자로, 2005년 4월 체질량지수 34.4 kg/m2 (체 중 88 kg, 키 160 cm)의 고도비만 진단 하에 개인병원에서
452 J Korean Surg Soc. Vol. 75, Suppl. II
Fig. 1. Schematic drawing of the operation that the patient had based on the referred doctor. The patient received lapar- scopic sleeve gastrectomy and banded gastroplasty using malex mesh.
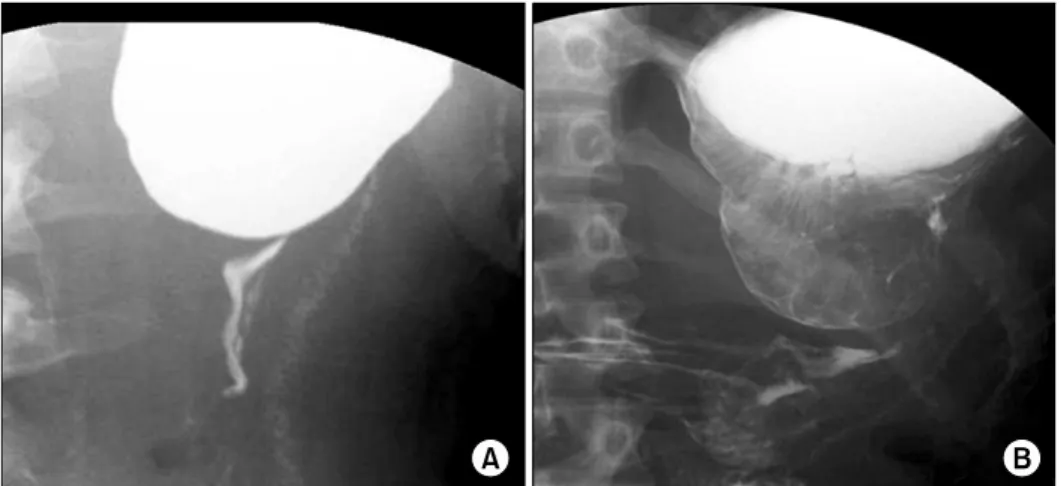
Fig. 2. Initial upper gastrointestinal series show severe stricture at distal gastric body with markedly dilatation of prox- imal portion of stomach.
This finings suggest gastric obstruction after laparscopic sleeve gastrectomy and banded gastroplasty.
Fig. 3. Schematic drawing of placements of trocars. A 11-mm tro- car (11) inserted through a peri-umbilical wound, and a 12-mm trocar (12) is inserted above and to the right of the umbilicus. A 5-mm trocar (5) above and to the left of the umbilicus, another two 5-mm trocars are inserted at the right and left costal margin. The distance between each tro- car should be greater than a grip to avoid interference among the trocars.
복강경하 위 소매 절제 및 밴드 성형술을 시행 받았다(Fig.
1). 병력 청취에서, 수술 당시 환자는 비만과 관련된 당뇨, 고혈압, 및 고지혈증 등의 동반질환은 없었다. 수술 후 지속 적인 체중감소가 이루어 졌으나, 지속되는 구토로 정상적 인 음식 섭취가 불가능 하였다. 밴드 성형술에 따른 위 협착 진단 하에, 같은 병원에서 2006년 9월 복강경하 밴드 제거 술을 시도했으나, 심한 유착으로 실패하였다. 이후 증상이 지속되어 2007년 12월 10일 본원 외래로 내원하였다. 내원 당시 환자의 체중은 42 kg으로 체질량 지수는 16.4 kg/m2였 으며, 위장관 조영술에서 위 중간 부분의 심한 협착과 함께 상부 위의 심한 확장 소견을 보였다(Fig. 2). 환자는 밴드에 의한 위 협착 진단 하, 2008년 1월 15일 복강경 보조 하 하
부 위 절제술 및 위-공장 문합술을 시행 받았다. 5개의 투관 침을 이용하여 수술을 진행하였다(Fig. 3). 복강경 시야에서 2개의 단위동맥이 남은 위치까지 소매 절제가 되어 있었고, 위 중앙 부위에 밴드 성형의 흔적으로 인한 섬유화를 확인 할 수 있었다. 수술 진행은 먼저 하부 위와 대장 사이의 대 망을 절단하여 간 만곡 부위로 진행하여 십이지장 내측을 노출 시킨 후 우위 대망 정맥 및 동맥을 절단하였다. 소망을 절단하여 소낭을 노출시킨 뒤 우위 정맥 및 동맥을 절단 후 위와 십이지장을 분리하였다. 위-공장 문합술을 시행할
Seung Wan Park and Yong Jin Kim:Complicated Gastric Stenosis after Laparoscopic Banded Gastroplasty 453
Fig. 5. Abdominal wound scar at 2 month postoperative date.
Black arrow indicates mini-laparotomy scar.
Fig. 4. Follow-up upper gastrointestinal series undertaken 7 days after laparoscopic assisted distal gastrectomy and gastro- jejunostomy. There is no passage disturbance without stricture.
공장을 Treitz 인대로부터 30 cm 아래에 methylene blue로 표 시한 뒤, 좌상복부 늑골연에 삽입 하였던 5 mm 투관침 부 위를 수평으로 3 cm 피부 절개를 가하여 소 개복을 시행하 였다. 소 개복 부위를 통해 먼저 위-공장 문합할 부위 30 cm 아래에 공장-공장 수기 문합술을 시행했으며 이후 소 개복을 통해 위 절단 및 위-공장 수기 문합을 시행하였다.
수술 시간은 총 230분이 소요되었다. 수술 후 제3병일에 식 이를 진행했으며, 수술 후 제5병일에 위장관 조영술을 시행 하였다(Fig. 4). 수술 후 특별한 문제없이 제8병일에 퇴원하 였으며, 현재 정상 식이 가능한 상태로 외래 추적 중이며 (Fig. 5) 수술 후 3개월이 경과한 현재 체중은 49 kg으로 회 복되었다.
고 찰
현재까지 전 세계적으로 가장 많이 시행된 음식 섭취를 제한하는 비만 수술은 위 밴드 성형술(수직형 위 밴드 성형 술 혹은 복강경하 위 밴드 성형술)과 복강경 하 조절형 위 밴드 성형술이다. 하지만 위 밴드 성형술의 경우 장기적으 로 충분한 체중감소를 유도하지 못한 채, 밴드로 인한 높은 합병증으로 더 이상 임상 적용이 이루어지고 있지 않다.(6) 본 증례도 복강경하 위 밴드 성형술 1년 5개월 후 밴드 자체 에 의한 협착으로 재 수술이 필요 했으며, 결국 위 절제술 및 위-공장 문합술로 수정이 불가피 하였다.
이런 이유로 2001년 이후 복강경하 조절형 위 밴드 성형술 이 소개 되면서, 현재 음식섭취를 제한하는 비만 수술의 가 장 대표적인 방법으로 자리 잡았다. 하지만 이 역시 Roux-en Y 위-공장 우회술에 비해 체중 감소가 장기적이지 못하며, 부적절한 식이 습관을 유도하기 쉽고, 장기적인 결 과의 축적이 없고, 동시에 밴드 자체로 인한 합병증이 20%
까지 보고되고 있는 문제점이 있다.(7) 더욱이 국내의 경우, 비만 수술과 관련하여 Han과 Kim(8)이 복강경하 위 소매 절제에 대해 장단기적 결과를 보고 한 것 이외에는 다른 수술 방법에 따른 경과 및 문제점에 대한 보고가 없는 실정 이다. 따라서 시술이 간편하고 수술 전후 합병증이 낮다는 이유만으로 시행 여부를 결정하는 것보다는 장기적인 결과 에 대한 충분한 고려가 필요할 것이다.
지금까지 위 밴드 성형술의 장기적 합병증으로 알려진 것으로는, 역류성 식도염, 밴드 미란(band erosion), 밴드 소 실(band slippage) 및 위낭 혹은 식도 확장 등이 있으며,(9) 이들 대부분의 경우 재수술이 필요한 것으로 알려져 있다.
이 경우와 함께 체중감소에 실패한 경우 교정 수술은 Roux-en Y 위-공장 우회술이 장기적인 측면에서 가장 효과 적이고 안전하다고 보고하고 있다.(10) 하지만 본 증례의 경우, 교정 수술의 주된 목적이 협착을 해소하는 데 있었기 에, 우회술보다는 위 부분 절제 및 위-위 문합술을 고려하였 다. 그러나 복강경 시야에서 환자의 위 전정부위가 이미 소 매 절제로 인해 소실되어 있어 부분 절제가 불가능 하였다.
또한 하부 위 절제 후 문합 방법의 결정인자로, 현재 환자의
454 J Korean Surg Soc. Vol. 75, Suppl. II
체질량 지수는 16.4 kg/m2로 이미 충분한 체중감소가 이루 어 졌다고 판단하여, 비용문제, 수술의 안정성, 술자의 숙달 도 및 간편성 등을 고려하였으며, 그 결과로 루프형 위- 공 장 문합 및 공장-공장 문합술을 선택하였다.
비만 수술의 효과는 단순히 체중감소에만 있는 것이 아 니며, 비만과 관련된 대사질환, 심혈관계 질환, 호흡기 질 환, 근골격계 질환 및 비뇨생식기계 질환의 개선에도 뚜렷 한 장점이 있다. 국내의 경우 식생활을 포함한 생활 방식이 서구화 되면서 병적 비만 환자의 수는 꾸준히 증가하고 있 다. 물론 국내에서도 다양한 수술이 시행되고 있기는 하나 그 장단점에 대해서는 아직 만족할 만한 결과들이 보고되 고 있지 않다. 이런 현실에서 본 증례는 비록 이제 임상에서 더 이상 적용되지 않는 위 밴드 성형술의 합병증에 대한 보고이나, 국내 비만 수술에 따른 합병증에 대한 최초 보고 로 그 의의가 있을 것이며, 동시에 현재 시행되는 복강경하 조절형 위 밴드 성형술 확대에 중요한 교훈이 될 것이다.
REFERENCES
1) Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric sur- gical procedures. JAMA 2005;294:1909-17.
2) Ministry of Health & Welfar. The third Korea national health and nutrition examination survey (KNHANES III), 2005.
3) Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H, et al. Swedish obese subjects study. Effects of bari- atric surgery on mortality in Swedish obese subjects. N Engl J Med 2007;357:741-52.
4) Adams TD, Gress RE, Smith SC, Halverson RC, Simper SC, Rosamond WD, et al. Long-term mortality after gastric bypass surgery. N Engl J Med 2007;357:753-61.
5) Miller K, Pump A, Hell E. Vertical banded gastroplasty versus adjustable gastric banding: prospective long-term follow-up study. Surg Obes Relat Dis 2007;3:84-90.
6) Kendrick ML, Dakin GF. Surgical approaches to obesity.
Mayo Clin Proc 2006;81(10 Suppl):S18-24.
7) Chapman AE, Kiroff G, Game P, Foster B, O'Brien P, Ham J, et al. Laparoscopic adjustable gastric banding in the treat- ment of obesity: a systematic literature review. Surgery 2004;135:326-51.
8) Han SM, Kim WW. Laparoscopic isolated sleeve gastrectomy in morbid obesity. Korean J Obes 2004;13:270-80.
9) Gustavsson S, Westling A. Laparoscopic adjustable gastric banding: complications and side effects responsible for the poor long-term outcome. Semin Laparosc Surg 2002;9:115-24.
10) Mognol P, Chosidow D, Marmuse JP. Roux-en-Y gastric by- pass after failed vertical banded gastroplasty. Obes Surg 2007;17:1431-4.