A comparison between two methods for tumor localization during totally laparoscopic distal gastrectomy in patients with gastric cancer
Chang Min Lee, Sungsoo Park, Seong-Heum Park, You Jin Jang, Seung-Joo Kim, Young-Jae Mok, Chong-Suk Kim, Jong-Han Kim
Department of Surgery, Korea University Medical Center, Korea University College of Medicine, Seoul, Korea
INTRODUCTION
In Korea, the prevalence of gastric cancer is decreasing.
However, it remains one of the most prevalent cancers and is the second leading cause of cancermediated death [1].
Recently, the increased use of endoscopy and greater reach of surveillance programs have enabled earlier diagnosis that has improved survival rates in patients with gastric cancer [2]. A nationwide survey conducted in 2009 revealed that early gastric cancer (EGC) constituted over half of the gastric cancer cases in Korea [1]. EGCs generally have good prognosis, and therefore
the quality of life (QoL) have been an important issue as well as oncologic outcome.
Around the same time, a new paradigm has been also de
veloped. Kitano et al. [3] first reported laparoscopyassisted distal gastrectomy (LADG) in 1994; thereafter, laparoscopic surgery has been widely accepted as a treatment option for gastric cancer in Korea. In addition, a recent multicenter study documented that laparoscopic gastrectomy is comparable to open gastrectomy with respect to longterm oncologic outcomes in gastric cancer [4]. Totally laparoscopic distal gastrectomy (TLDG) is one of the practices inheriting the paradigm, and has Purpose: The aim of this study was to compare two methods of tumor localization during totally laparoscopic distal gas- trectomy (TLDG) in patients with gastric cancer.
Methods: From March 2014 to November 2014, patients in whom TLDG had been engaged for middle third gastric cancer enrolled in this study. The patients were allocated to either the radiography or endoscopy group based on the type of tumor localization technique. Clinicopathologic outcomes were compared between the 2 groups.
Results: The accrual was suspended in November 2014 when 39 patients had been enrolled because a failed localization happened in the radiography group. The radiography and endoscopy groups included 17 (43.6 %) and 22 patients (56.4 %), respec tively. Mean length of the proximal resection margin did not differ between the radiography and endoscopy groups (4.0 ± 2.6 and 2.8 ± 1.2 cm, respectively; P = 0.077). Mean localization time was longer in the radiography group than in the endoscopy group (22.7 ± 11.4 and 6.9 ± 1.8 minutes, respectively, P < 0.001). There were no statistically significant differ- ences in the incidence of severe complications between the 2 groups (5.9% and 4.5%, respectively, P = 0.851).
Conclusion: As an intraoperative tumor localization for TLDG, radiologic method was unsafe even though other comparable parameters were not different from that of endoscopy group. Moreover, intraoperative endoscopic localization may be advantageous because it is highly accurate and contributes to reducing operation time.
[Ann Surg Treat Res 2016;91(3):112-117]
Key Words: Laparoscopy, Gastrectomy, Endoscopy, Stomach neoplasms
Reviewed January February March April May June July August September October November December
http://dx.doi.org/10.4174/astr.2016.91.3.112 Annals of Surgical Treatment and Research
Received January 11, 2016, Revised May 17, 2016, Accepted June 3, 2016 Corresponding Author: Jong-Han Kim
Department of Surgery, Korea University Medical Center Ansan Hospital, 123 Jeokgeum-ro, Danwon-gu, Ansan 15355, Korea
Tel: +82-31-412-5957, Fax: +82-31-413-4829 E-mail: [email protected]
Copyright ⓒ 2016, the Korean Surgical Society
cc Annals of Surgical Treatment and Research is an Open Access Journal. All articles are distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
shown several advantages over LADG. Its advantages include safe anastomosis independent of the location of the lesion [5], decreased wound problems [6], and feasibility in obese patients [7,8].
However, some critical issues have been raised by the surgeons performing TLDG. One of the issues is the localization of a tumor. Minilaparotomy is not performed during TLDG, and therefore the a lesion needs to be visually localized. However, as EGCs do not involve the serosal layer, the location of a tumor cannot be determined by the laparoscopic view alone.
Moreover, if the tumor is located on the relatively proximal portion of the stomach, it can be difficult to determine the range of resection; this compromises both, the oncologic safety and postoperative QoL of the patient.
In our center, the following 2 types of localization techniques have been performed during TLDG: intraoperative radiographic imaging and intraoperative endoscopy. In this study, the feasibility and safety of these 2 methods were compared.
METHODS
Study design and participants
This was doublearm, openlabel, prospective study per
formed in a single institute. From March 2014, we serially enrolled the patients in whom TLDG had been engaged for gastric adenocarcinoma of middle third [9]. The planned sample size was set at 100 (50 on each arm), and planned duration of accrual was 1 year. In addition, our protocol stated that accrual should be suspended if any critical problem happens in either group.
During the study period, one surgeon performed all these operations. All enrolled patients underwent R0 resection and lymphadenectomy more than D1+. Patients whose lesion showed serosal invasion were excluded from this study.
The patients were randomized into the radiography and endoscopy groups based on the type of localization technique.
The radiography group included the patients who were engaged in radiographic imaging for intraoperative localization of lesions. The endoscopy group included the patients who were engaged in intraoperative endoscopy to localize tumors. In the endoscopy group, an assistant surgeon who was trained in endoscopic procedures performed all intraoperative endoscopic procedures during this period. In both groups, preoperative endoscopic clipping was performed by gastroenterologist. One or 2 metallic clips (HX600090L, Olympus, Tokyo, Japan) were applied immediately proximal to the lesion (Fig. 1).
Informed consent for both localization methods was obtained from every patient. This study was approved for research on human subjects by the Institutional Review Board of Korea University Medical Center Ansan Hospital (approval number:
AS15080).
Common surgical procedures
The same surgical procedures were performed in both groups, but reconstruction methods were individualized according to the location of the tumor. The patient was put under general anesthesia and placed on the bed with both legs abducted. The bed was adjusted to place the patient in the reverse Trendelenburg position. The operator stood on the right side of the patient, the assistant on the left side, and the scopist between the patient’s legs. After a pneumoperitoneum of 12–14 mmHg was established, a 12mm trochar was inserted into the supraumbilical area by Hasson’s method. A flexible scope was inserted through the supraumbilical port and four working ports were established under laparoscopic guidance.
Lymphadenectomy for curative distal gastrectomy was performed based on the Japanese Gastric Cancer Treat ment Guidelines 2010 (ver. 3) [10]. After completion of lymph ade
nectomy, the patient underwent tumor localization by either intraoperative radiographic imaging or intraoperative endo
scopy, according to the protocol for each group. The range of gastrectomy was determined according to the result of tumor localization. Billroth II or Roux en Y reconstruction was per
formed for recovery of gastrointestinal continuity.
Tumor localization
In the radiography group, the procedure after lymphadenec
tomy was performed as follows: before dividing the stomach during TLDG, fixable graspers were applied proximal and distal to the portion expected to be the tumor sites. After applying the graspers to the stomach, plain abdominal radiographs were taken. The location of the tumor was determined according to the correlation between the graspers and metallic clips in Fig. 1. Preoperative endoscopic clipping. Several metal clips were applied in the preoperative endoscopy.
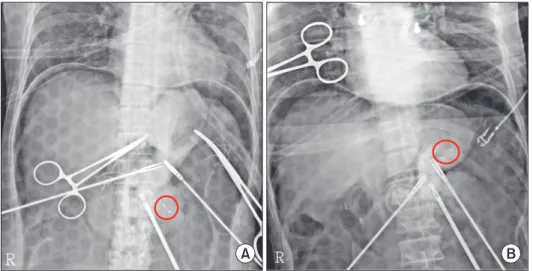
the images. When the metallic clips were located between the graspers (Fig. 2A), the stomach was resected proximally to the fixed graspers. When the clips were located proximally to both graspers (Fig. 2B), the stomach was resected at the most proximal level involving no clip; the “most proximal level” was estimated based on the radiographs.
In the endoscopy group, after lymphadenectomy was com
pleted, one surgeon performed the intraoperative endoscopy while another surgeon carefully manipulated the stomach in the laparoscopic field. Through the endoscopic view, the location of the metallic clips was compared to that of the mu
cosal protrusion formed by laparoscopic manipulation. Both surgeons discussed the location of the tumor in the laparoscopic view, while comparing the endoscopic and laparoscopic views (Fig. 3). Through this process, they determined the location of the tumor in the laparoscopic view.
Comparisons of data between 2 groups
Clinical data including the sex, age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, operation time (in minutes), tumor localization time (in minutes), postoperative hospital stay (in days), time to the first meal (in days), and postoperative complication were compared between the radiography and endoscopy groups. Postoperative complications were classified according to the ClavienDindo classification of surgical complications [11]. Tumor localization time was defined as the time from insertion of the gastro
fiberscope until determination of the tumor location in the laparoscopic view.
In addition, the length of proximal resection margin was also compared between the 2 groups.
Statistical analysis
IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA) and R ver.
2.15.2 (R Foundation for Statistical Computing, Vienna, Austria;
http://www.rproject.org/) were used for statistical analyses.
Chisquare test and Student ttest for independent samples were used for comparisons between the radiography and endoscopy groups. For all data analyses, P < 0.05 was considered stati sti
cally significant.
RESULTS
The actual enrollment started in March 2014. However, the accrual was suspended in November 2014 when 39 patients had been enrolled because a failed localization happened in the radiography group. Therefore, from March 2014 to November 2014, a total of 39 patients were enrolled in this study.
Patient demographics
Patient demographics can be seen in Table 1. Of the 39 patients enrolled in this study, 17 (43.6 %) were in the radio
graphy group and 22 (56.4 %) in the endoscopy group. The 2 groups show no significant difference in the mean age (P = Fig. 2. Radiographs showing the lo ca tion of metallic clips. (A) Clips were located between the gra s pers (Red circle indicates the pre operative applied clips.). (B) Clips were located proximal to the graspers (Red circle indicates the preoperative applied clips.).
A B
Fig. 3. Tumor localization by intraoperative endoscopy. Two surgeons determined the location of tumor in the lapar
oscopic view, as they compared the endoscopic and lapar
oscopic view.
0.173), sex ratio (P = 0.358), mean BMI (P = 0.509), and ASA score (P = 0.417).
Comparison of clinicopathologic outcomes
The mean tumor localization time was significantly longer in the radiography than endoscopy group (P < 0.001). However, the 2 groups show no statistically significant difference in the mean operation time (P = 0.080), mean hospital stay (P = 0.096), and mean time to the first meal (P = 0.971) (Table 2).
In addition, the mean length of the proximal resection margin did not differ between the radiography and endoscopy groups (P = 0.077) (Table 2).
Comparison of postoperative complications
Postoperative complications occurred in 9 cases (20.5%), including 4 (23.5%) in the radiography group and 4 (18.2%) in the endoscopy group. Severe complications, defined as more severe than grade II by the ClavienDindo classification of surgical complications, occurred in 2 patients, including 1 (5.9%) in the radiography group and 1 (4.5%) in the endoscopy group.
However, there were no statistically significant differences between the 2 groups in terms of morbidity (P = 0.682) and severe morbidity (P = 0.851) (Table 2).
In addition, there was no mortality in either group (Table 2).
DISCUSSION
Recently, several solutions have been proposed for intra
operative tumor localization during TLDG. Ohdaira and Nagai [12] reported the use of a magnetic marking clipdetecting system (MMCDS). In this technique, tumor is localized by MMCDS probe that responds to magnetic clips attached during preoperative endoscopy. Kim et al. [13] applied portable abdominal radiographs for intraoperative localization during TLDG for EGC. In addition, several localization methods have been designed using endoscopy [1416]. Of these diverse me
thods, one is selected according to the preferences of the
surgeons, since there has not been evidence that a specific method is superior to the others. Also, it has been difficult to compare the localization methods because most surgeons tend to adopt the only procedure they are accustomed to. However, two different methods have been used for tumor localization during TLDG in our center, and therefore we could accomplish a comparative analysis with the prospectively collected data.
To our knowledge, this is the first study to compare different methods for intraoperative tumor localization during TLDG.
Although the small sample size was a limitation of this study, the demographic data were not statistically different between the patients who underwent radiographic and endoscopic localization during TLDG. We compared the clinicopathologic outcomes between the 2 groups, and endoscopic localization resulted in a shorter tumor localization time than radiographic localization. Moreover, the 2 methods did not differ in the morbidity rate, although several complications may be caused by endoscopy [1719].
Radiographic localization is widely accepted as an easy way to localize a tumor. Not using a similar protocol as ours but confirming the location of preoperatively attached clip would be helpful for determination of the tumor site. However, there are several problems with radiographic localization. First, it takes considerable time to acquire an intraoperative image. Although we exclude the time spent awaiting the arrival of a radiographer, significant time is required to produce the radiographic image.
Moreover, if the radiographer errs in focusing the metallic clips, more time will be needed to get a wellfocused image. In the radiography group, this problem resulted in a tumor localization time of about 1 hour. In these cases, the prolongation of the tumor localization time was related to the long operation time.
In addition, because the stomach is composed of 3dimen
Table 1. Patient demographics Demographic Radiography
group (n = 17) Endoscopy
group (n = 22) Pvalue
Age (yr) 52.5 ± 14.0 58.1 ± 11.0 0.173
Sex, male:female 11:6 11:11 0.358
Body mass index (kg/m2) 23.7 ± 3.5 24.6 ± 4.2 0.509
ASA score 0.417
1 6 (35.3) 6 (27.3)
2 11 (64.7) 14 (63.6)
3 0 (0) 2 (9.1)
Values are presented as mean ± standard deviation or number (%).
ASA, American Society of Anesthesiologists.
Table 2. Comparison of clinicopathologic outcomes bet
ween the radiography and endoscopy group Variable Radiography
group (n = 17) Endoscopy
group (n = 22) Pvalue Operation time (min) 308.9 ± 39.4 285.1 ± 42.2 0.080 Tumor localization time
(min) 22.7 ± 11.4 6.9 ± 1.8 <0.001
Hospital stay (day) 8.2 ± 1.1 9.1 ± 1.8 0.096 Time to the first meal
(day) 5.4 ± 1.1 5.4 ± 0.7 0.971
The length of proximal
resection margin (cm) 4.0 ± 2.6 2.8 ± 1.2 0.077
Morbidity (%) 23.5 18.2 0.682
Morbidity, CD grade
>II (%) 5.9 4.5 0.851
Values are presented as mean ± standard deviation unless other
wise indicated.
CD grade, grade by the ClavienDindo classification of surgical com plications.
sional structures, the 2dimensional view of intra operative radiography could provide incorrect information about the location of a tumor. In regard to such a discrepancy, we expe
rienced a case of failed localization; in this patient, the metallic clips were located proximal to both graspers. Despite gastric resection was performed with considering the distribution of the clips and graspers, we found that the clips were located above the resection line in the laparoscopic view. This pheno
menon was assumed to have resulted from a discrepancy bet
ween the radiographic and real distribution of the clips and graspers. This discrepancy could happen again in the radio
graphy group, if the accrual was not suspended. Since any failed localization was considered to be possibly critical in longterm outcome, we terminated the accrual of patient.
In contrast, endoscopic localization produced less discre
pancy than radiographic localization, since it provided a 3dimensional image of gastric lumen. Moreover, because the endoscopic view could be compared with laparoscopic view in real time, any localization error could be immediately identified and corrected. Therefore, intraoperative endoscopy provided more precise localization than radiography. Such an advantage is implied in Table 2. In the endoscopy group, the lengths of proximal resection margin were distributed within a narrow range.
In addition, endoscopic localization had a shorter localization time than radiographic localization. As described above, endoscopic localization does not require any separate time to build an image for tumor localization, because it is a real time procedure. Although the total operation time was not significantly different between the 2 groups in our data, the shortened localization time may contribute to reducing the total operation time in the larger population.
For these and other reasons, many institutes have introduced intraoperative endoscopy for tumor localization. Recently, Xuan et al. [15] and Jeong et al. [16] also reported their experiences regarding intraoperative endoscopy in TLDG for gastric cancer. However, with regard to endoscopic localization, our institute has maintained 2 special rules, not emphasized in other institutes. First, preoperative endoscopic clipping is obligated. Although Xuan et al. [15] questioned the need for this procedure, our intention is to guarantee the accuracy of localization. As in Fig. 4, if preoperative clipping is not done, it could difficult to localize an ambiguous and broad lesion with intraoperative endoscopy. Second, to prevent excessive gastric resection, preoperative clipping is applied immediately proximal to the tumor. Jeong et al. [16] placed endoscopic clips on the proximal 1 cm of the tumor, even though they also supported preoperative endoscopic clipping. However, most surgeons depend on the location of the clips to determine resection line, and therefore remotely located clips can result in excessive resection.
Ultimately, these rules support surgeonperforming endo
scopic localization, since preoperative clipping is a guidance for the surgeon who performs intraoperative endoscopy in our institute. Is there any reason for why we hold to surgeon
performing endoscopic localization? If surgeons perform the intraoperative endoscopy as in our institute, the advantages of endoscopic localization will be increased. Although gastro
enterologists have more experience in endoscopic proce dures, there are 2 issues of note that limit their involvement in intraoperative endoscopy. First, it is difficult for gastroen
terologists to engage in intraoperative localization, since it takes time away from other responsibilities. If it takes a long time to wait for the arrival of gastroenterologist, the overall operation time can be prolonged. Second, intraoperative endoscopy is rather different from conventional endoscopy performed in the outpatient clinic. Because the patients are in the supine position and have an endotracheal tube for ventilatior care, inexperienced gastroenterologists can have difficulty in inserting and manipulating the gastrofiberscope.
However, if gastroenterologic surgeons are sufficiently trained for intraoperative endoscopy, these issues can be solved. Recog
nizing this reality, some institutes have provided edu cation programs in which surgeons are trained for endo scopy.
In conclusion, as an intraoperative tumor localization for TLDG, endoscopic method is comparable to radiographic method in terms of several clinical outcomes. However, based on our experience of failed localization, radiologic method was unsafe even though other comparable parameters were not different from that of endoscopy group. Moreover, intra
operative endoscopic localization may be advantageous because it is highly accurate and contributes to reducing operation time.
Fig. 4. Necessity of preoperative endoscopic clipping. With
out preoperative clipping, it is difficult to determine the range of an ambiguous and broad lesion (Yellow arrowhead indi
cates the preoperatively applied clips.).
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer 2011;11:6977.
2. Hochwald SN, Brennan MF, Klimstra DS, Kim S, Karpeh MS. Is lymphadenectomy necessary for early gastric cancer? Ann Surg Oncol 1999;6:66470.
3. Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopyassisted Billroth I gastrec
tomy. Surg Laparosc Endosc 1994;4:1468.
4. Kim HH, Han SU, Kim MC, Hyung WJ, Kim W, Lee HJ, et al. Longterm results of laparoscopic gastrectomy for gastric can
cer: a largescale casecontrol and case
mat ched Korean multicenter study. J Clin Oncol 2014;32:62733.
5. Ikeda O, Sakaguchi Y, Aoki Y, Harimoto N, Taomoto J, Masuda T, et al. Advantages of totally laparoscopic distal gastrectomy over laparoscopically assisted distal gas
trec tomy for gastric cancer. Surg Endosc 2009;23:23749.
6. Oki E, Sakaguchi Y, Ohgaki K, Saeki H, Chinen Y, Minami K, et al. The impact of obesity on the use of a totally laparoscopic distal gastrectomy in patients with gastric cancer. J Gastric Cancer 2012;12:10812.
7. Kim MG, Kawada H, Kim BS, Kim TH, Kim KC, Yook JH, et al. A totally lapar
os copic distal gastrectomy with gas tro
duodenostomy (TLDG) for improvement of the early surgical outcomes in high BMI patients. Surg Endosc 2011;25:1076
82.
8. Kim MG, Kim KC, Kim BS, Kim TH, Kim HS, Yook JH, et al. A totally laparoscopic distal gastrectomy can be an effective way of performing laparoscopic gastrectomy in obese patients (body mass index≥30).
World J Surg 2011;35:132732.
9. Japanese Gastric Cancer Association. Japa
nese classification of gastric carcinoma:
3rd English edition. Gastric Cancer 2011;
14:10112.
10. Japanese Gastric Cancer Association. Japa
nese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer 2011;14:113
23.
11. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al.
The ClavienDindo classification of sur
gical complications: fiveyear expe rience.
Ann Surg 2009;250:18796.
12. Ohdaira T, Nagai H. Intraoperative lo cali
zation of earlystage upper gastro intes
tinal tumors using a magnetic marking clipdetecting system. Surg Endosc 2007;
21:8105.
13. Kim HI, Hyung WJ, Lee CR, Lim JS, An JY, Cheong JH, et al. Intraoperative por table abdominal radiograph for tumor locali
za tion: a simple and accurate method for lapar oscopic gastrectomy. Surg Endosc
2011;25:95863.
14. Jeong O, Cho SB, Joo YE, Ryu SY, Park YK.
Novel technique for intraoperative tumor locali zation during totally laparoscopic dis tal gastrectomy: endoscopic auto lo gous blood tattooing. Surg Endosc 2012;26:
177883.
15. Xuan Y, Hur H, Byun CS, Han SU, Cho YK.
Efficacy of intraoperative gastroscopy for tumor localization in totally laparoscopic distal gastrectomy for cancer in the mid
dle third of the stomach. Surg Endosc 2013;27:436470.
16. Jeong SH, Bae K, Ha CY, Lee YJ, Lee OJ, Jung WT, et al. Effectiveness of endoscopic clipping and computed tomography gas
tro scopy for the preoperative localiza tion of gastric cancer. J Korean Surg Soc 2013;
84:807.
17. Zubarik R, Eisen G, Mastropietro C, Lopez J, Carroll J, Benjamin S, et al. Prospective analysis of complications 30 days after out patient upper endoscopy. Am J Gas tro
enterol 1999;94:153945.
18. Kavic SM, Basson MD. Complications of endoscopy. Am J Surg 2001;181:31932.
19. Geraci G, Pisello F, Modica G, Li Volsi F, Arnone E, Sciume C. Complications of elective esophagogastroduodenoscopy (EGDS). Personal experience and literature review. G Chir 2009;30:5026.