다전극
7
0
0
전체 글
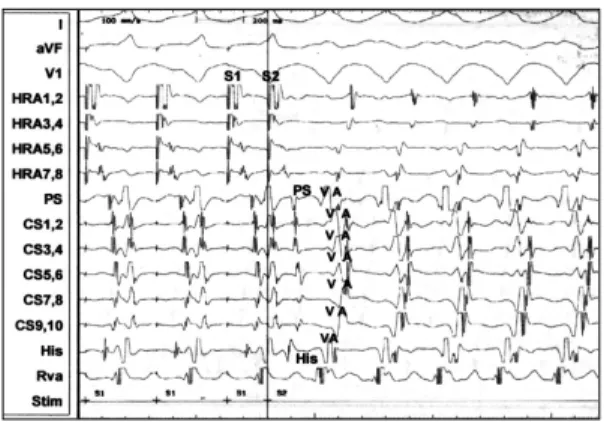
(2) AH는 83 ms, HV 36 ms, QRS 81 ms였고, 방실차단. 증. 례. 주기(AVBCL)는 300 ms, 방실결절 유효불응기(AVNERP)는 250 ms, 심방 유효불응기(AERP)는 240 ms,. 증 례 1:. 실방차단 주기(VABCL)는 350 ms, 심실 유효불응기. 환 자:정○○, 남자, 34세.. (VERP)는 220 ms였다. 심방 기외자극시 방실결절의. 주 소:6년 전부터 반복되는 발작성 심계항진.. 이중회로 전기생리는 관찰되지 않았으며, 우심실 조율. 현병력:환자는 평소 건강하던 자로 약 6년전부터. 시 역행전도의 활동순서는 His 기록부위가 117 ms로. 무거운 것을 들거나 심한 운동을 한 뒤 갑자기 유발되. 가장 빨랐으나 역행전도의 지연전도 속성은 관찰되지 않. 는 심계항진을 주소로 내원하였다. 심계항진은 일년에. 았다. 빈맥유발을 위해 isoproterenol을 정주하면서 신. 5~6회 가량 나타났으며 30분에서 길게는 3시간까지 지. 속 심방조율 및 심방 기외자극을 실시한 결과 빈맥주기. 속되었다. 심계항진이 나타날 때는 어지러움증이 동반. 270 ms의 방실회귀성 빈맥이 유발되었으며(Figs. 2. 되었으며 빈맥은 휴식을 취하는 동안 저절로 소실되기. and 3) 이때 가장 빠른 역행전도위치는 His 기록부위. 도 하였다.. (VA 간격은 68ms)였고 빈맥중 연결간격(coupling int-. 이학적 소견:특이 소견 없음.. erval) 200 ms의 심실기외자극에 의해 reset을 보였. 검사소견:혈액검사, 생화학검사, 소변검사, 흉부 방. 다(Fig. 4). 이와 같이 우심실 조율시 심실중격부위에. 사선 검사상 특이소견 없음. 심전도:정상 동성맥, 정상 QRS 소견(Fig. 1). 심초음파:특이소견 없음. 심구혈률은 65%. 다전극 basket 도자의 크기결정을 위해 하측흉골연 창에서 측 정한 우심방 크기는 종축이 39 mm, 횡축이 57 mm였다. 전기생리검사 및 도자절제:환자는 4시간 이상의 금 식상태에서 심장 전기생리검사를 시행하였다. Midazolam 4 mg을 정주하여 환자를 안정시킨 상태에서 양 측 서혜부에 2% lidocaine을 주사하여 국소 마취를 시 켰다. 우측 대퇴정맥을 Seldinger 방법으로 천자하여 7F 고주파 절제 도자를 우심방에 위치시켰고 좌측 대 퇴정맥을 통하여 6F 삼극도자와 6F 사극도자를 His 기 록위치와 우심실 심첨부에 각각 위치시켰다. 좌측 쇄골 하부에 2% lidocaine으로 국소마취후 6F 십극도자를. Fig. 2. Induction of PSVT during atrial extrastimulation test. Typical atrioventricular reciprocating tachycardia was noted and the earliest retrograde atrial activation site was at His recording area near the right interventricular septum.. 좌 쇄골하정맥을 통하여 관정맥동 내로 위치시켰다. 전 기생리검사 결과 동성맥의 주기는 807ms였으며 이때. Fig. 1. Electrocardiogram on admission showed normal sinus rhythm.. Fig. 3. Electrocardiogram during tachycardia induction showed wide QRS tachycardia with left bundle branch block pattern and left axis. There is no visible AV dissociation.. 1449.
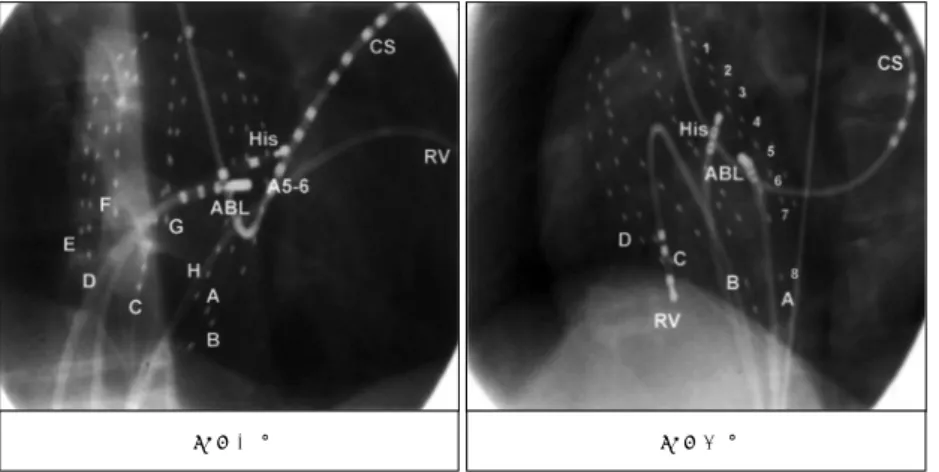
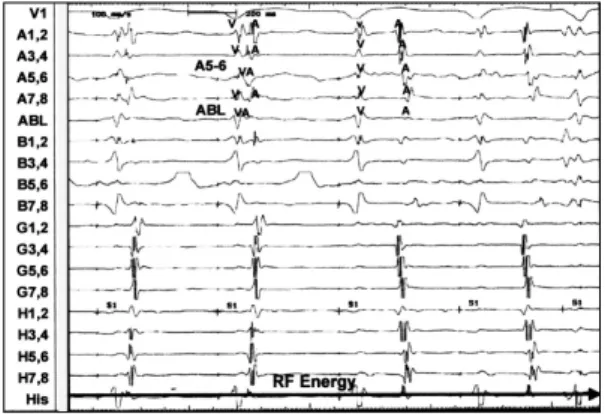
(3) 서 가장 빠른 실방전도 양상을 보이나 실방 지연전도의. 의 위치는 1에서 8까지 원위부에서 근위부쪽으로 수치. 소견을 보이지 않고 빈맥시 심실기외 자극에 의해 reset. 화하여 구별하였다(Fig. 5). 우측 대퇴정맥을 새로 천. 현상이 관찰되어 심실중격 우회로에 의한 방실회귀성. 자하여 035 유도철선을 따라 8F 전용 삽관을 삽입하였. 빈맥으로 진단하였다. 이에 불현성 우회로의 정확한 위. 고 이를 통해 방사선 투시를 하면서 basket 도자를 하. 치 도해를 위하여 다전극 basket 도자를 삽입하였다.. 대정맥과 우심방 경계부위에 위치시켰다. basket 도자. 60×40 mm 크기의 64 다전극 basket 도자(Con-. 전용삽관에는 정맥 혈전 및 색전 발생을 예방하기 위하. stellation, EPT)를 8F 전용삽관(sheath)에 넣고 생리. 여 헤파린 용액을 지속적으로 주입하였다. 8F 삽관에. 식염수에 담궈 도자를 움직이면서 도자와 삽관 사이에. 들어있는 basket 도자를 더 진행하여 도자를 우심방에. 있는 작은 공기방울을 제거하였다. 다전극 basket 도자. 완전히 펼쳐지도록 위치하였고 전극을 연결하여 가장. 는 8가닥의 유연하고 자발적으로 펼쳐지는 nitinol 선. 적절한 전극도가 기록되는 위치에 고정하였다. Basket. 에 백금-이리듐 합금으로 된 전극을 4~5 mm 간격으. 도자의 위치가 안정된 후 7F 전극절제 도자를 다시 조. 로 각각 8개씩 배열하여 총 64전극을 심내막 표면에서. 정하여 우측 중격에 위치시켰다. 일단 도자삽입이 끝난. 동시에 기록할 수 있도록 구성되었다. 8가닥의 선은 각. 뒤부터는 basket 도자의 위치는 이동하지 않았으며 마. 각 A에서 H까지 굵은 전극의 위치로 구별하였고 전극. Fig. 4. Reset of AVRT by single ventricular extrastimulus. A ventricular extrastimulus introduced from RV apex at a coupling interval of 200 ms preexcites the atrium when the His bundle is refractory, confirming the presence of functioning midseptal bypass tract.. RAO 30°. Fig. 6. Multisite recordings from right atrium during ongoing tachycardia. The earliest retrograde atrial activation was recorded at A5-6 and the distal pair of ablation catheter.. RAO 60°. Fig. 5. Fluoroscopic views of the 64 electrode basket catheter in the right atrium. Spline locations in the right atrium were as follows:splines A and B in the anteroseptum, splines C and D in the lateral wall, splines E and F in the posterior wall, and splines G and H in the posteroseptum. In RAO 30° , ablation catheter (ABL) was positioned at A56 area near the His recording catheter. But in LAO 60° , it was inferposterior side to His recording catheter.. 1450. Korean Circulation J 2000;30(11):1448-1454.
(4) 지막 위치를 우전사 30도, 좌전사 60도 영화 방사선. 시도하였으나 빈맥은 더 이상 나타나지 않았다. 전극도. 투사로 기록하였다(Fig. 5). 심장내 전극도는 증폭하여. 자 절제후 표면 심전도상 PR 간격 연장 등의 특별한. 1000 Hz에서 계수화하여 증폭, 여과(30~500 Hz)하. 변화는 보이지 않았다(Fig. 8).. 였으며 Prucka Cardiolab System 3.1을 사용하여 광 학디스크에 저장하였다. 전기자극 및 조율은 Bloom-. 증 례 2:. DTU215A자극기를 사용하였다. 우심방 기외자극으로. 환 자:박○○, 남자, 18세.. 유발된 방실회귀성 빈맥동안 basket 도자로 기록한 활. 주 소:6개월 전부터 반복되는 발작성 심계항진.. 동순서 mapping상 역행적 실방간격의 가장 빠른 전극. 현병력:환자는 평소 건강하던 자로 99년 말부터 운. 의 위치는 우측 중중격(mid septum)에 있었다(Figs. 5. 동시 급작스럽게 나타나는 심계항진을 주소로 내원하였. and 6). 이에 고주파 절제 도자를 방사선 투시로 가장. 다. 심계항진은 한달에 3~4회 가량 나타났으며 10분. 빠른 전극 부위인 A5-6에 위치시키고 고주파 에너지. 에서 1시간 가량 지속되었다. 어지러움증과 전신쇄약감. 를 방출하였다. 500 ms 우심실 조율을 시행하면서 고. 이 동반되었으며 빈맥은 저절로 소실되었다.. 주파 에너지를 투여한 후 4초만에 VA 간격이 벌어지 면서 우회로는 성공적으로 절제되었다(Fig. 7). 전극도 자 절제후 심실 조율시 전도는 중중격 우회로가 아닌. 이학적 소견:특이소견 없음. 검사소견:혈액검사, 생화학검사, 소변검사, 흉부 방 사선 검사상 특이소견 없음.. His 속으로 전도되었고 이때 실방차단 주기는 600 ms. 심전도:V1~2유도에서 R/S<1, II, III, aVF유도에서. 였다. 다시 isoproterenol 정주를 하면서 빈맥유발을. 양성 델타파를 보여 우측 전벽 우회로에 의한WPW 증 후군에 합당한 소견을 보였다(Fig. 9). 심장초음파:심구혈률 70%으로 정상이었으며, 다전 극 basket 도자의 크기결정을 위해 하측흉골연 창에서 측정한 우심방의 크기는 종축이 47 mm, 횡축이 39 mm 였다. 전기생리검사 및 도자절제:전술한 증례와 동일한 방법으로 50×40 mm 다전극 basket 도자를 방사선 투 시하에 우심방 내에 완전히 펼쳐지도록 위치시키고 가 장 적절한 전극도가 기록되는 위치에서 고정하였다. 다 전극 basket 도자의 위치가 안정된 후 우측 대퇴정맥. Fig. 7. Multisite recordings from right atrium showed abrupt block of retrograde conduction in the bypass tract 4 seconds after the onset of 28 watts of RF energy.. 을 통해서 7F 전극절제 도자를 삽입하여 우측 전중격에 위치시켰고, 좌측 대퇴정맥을 통하여 6F 사전극 도자를 우심첨부에, 6F His 도자를 His 속 기록부위에 각각 위치. Fig. 8. Electrocardiogram after successful RF ablation was not different from that at baseline.. Fig. 9. Electrocardiogram on admission showed short PR interval, positive delta waves in lead Ⅰ, Ⅱ, Ⅲ, and aVF, and R/S ratio less than 1 in V1-2, indicates typical WPW syndrome with right anteroseptal bypass tract.. 1451.
(5) RAO 30°. RAO 60°. Fig. 10. Fluoroscopic views of the 64 electrode basket catheter in the right atrium. Spline locations in the right atrium were as follows:splines A and B in the anteroseptum, splines C and D in the lateral wall, splines E and F in the posterior wall, and splines G and H in the posteroseptum. In RAO 30° , ablation catheter (ABL) was positioned at B3-4 area near the His recording catheter. But in LAO 60° , it was anterior side to His recording catheter.. Fig. 11. A sinus complex with preexcitation over an anteroseptal bypass tract demonstrates the earliest ventricular activation preceeding delta wave in the B3-4.. Fig. 13. Multisite recordings from the right atrium during RF (28w) ablation of anteroseptal bypass tract. RF energy is delivered during sinus rhythm. AV intervals are suddenly prolonged and prexicitation is lost.. 시켰다. 일단 도자삽입이 끝난 뒤부터는 basket 도자 의 위치는 이동하지 않았으며 마지막 위치를 우전사 30도, 좌전사 60도 영화 방사선 투사로 기록하였다(Fig. 10). 동성맥, 또는 우심실 조율을 하면서 관찰한 가장 빠 른 전극의 위치는 우측 전중격에 있었으며(Figs. 11 and 12) 고주파 절제 도자를 방사선 투시로 basket 도자의 가장 빠른 전극 부위(B 3, 4)에 위치시켜 고주파 에너 지를 투여하였으며 4초 이내에 우회로가 성공적으로 절 제되었다(Fig. 13). 이때 표면 심전도에서 델타파가 소 Fig. 12. Multisite recordings from right atrium during right ventricular pacing. Earliest retrograde atrial activation was recorded at B3-4 and the distal pair of ablation catheter (ABLdist).. 1452. 실 되었다(Fig. 14). 전극도자 절제후 심실-심방차단 주기는 550 ms으로서 절제전 220 ms에 비하여 연장 되었다. 총 방사선 투시 시간은 37.3분 이었다.. Korean Circulation J 2000;30(11):1448-1454.
(6) 상을 전산 시뮬레이션으로 관찰할 수 있게 되었다.14) 다전극 basket 도자 삽입시 초래될 수 있는 합병증으 로는 공기 또는 혈전성 색전, 심장파열과 같은 기계적 합 병증 등이 있다. 동물실험 결과에 의하면, 다전극 basket도자로 인하여 상대정맥, 하대정맥, 우심방-상대 정맥 연결부위, 우심방 부속기 기저부, 삼첨판의 심방 쪽 판막부위에 찰과상을 남길 수 있으며15) 만성적으로 는 경미한 심내막 섬유화를 상처부위에 남겨서16) 무리 Fig. 14. Electrocardiogram after successful RF ablation. There was no delta wave and PR interval returned to normal.. 한 도자조작에 주의해야 함을 시사하였다. 최근 개발되어 임상에서 이용되고 있는 고해상도 mapping 시스템으로는 비접촉 심내막 mapping법(non-. 고. 안. contact endocardial mapping),17)18) 비X선 투시형 3 차원적(non-fluoroscopic 3 dimensional) 또는 전기해. 우측 우회로를 동반한 조기흥분 증후군이나 불현성. 부학적(electroanatomic) mapping 법19)20) 등이 있으. 우회로의 경우, 좌측 우회로에 비해 방실 상도(AV gro-. 나 이들은 대체로 매우 고가의 장비로서 경제적인 한계. ove)의 원주길이가 길고, 삼첨판막과 삼첨륜의 각도가. 점들이 따른다. 다전극 basket 도자는 비교적 단순하. 직각에 가까워 mapping이 어려우며, 관정맥동과 같은. 면서도 경제적인 시스템 중의 하나로서 우리나라 실정. 전극도자를 고정할 수 있는 해부학적 구조물이 없는 점. 에서 통상적인 mapping 방법으로 접근하기가 어려운. 등으로 인해 활동순서 mapping 및 고주파를 이용한. 방실 회귀성 빈맥이나 심방빈맥,13) 심실빈맥11)12)등의. 전극도자 절제에 시간이 많이 걸리고 성공률이 낮으며. 복잡한 부정맥의 경우에 시도해 볼 수 있는 방법의 하. 1-4). 재발률이 높은 것으로 알려져 있다.. 특히 우측 중격. 나로 생각된다.. 또는 전중격 우회로의 경우에는 mapping이 어려울 뿐. 요. 아니라 방실결절과 매우 인접하여 전극도자 절제시 주. 약. 의를 요한다. 때문에 본 증례에서는 이러한 전통적 활동 순서 mapping의 제한점을 극복하기 위해 다전극 basket. 저자들은 우측 중격 우회로를 동반하는 방실 회귀성. 도자를 이용하여 우측 중격 부위의 우회로를 정확하고. 빈맥 2례를 다전극 basket 도자로 mapping하여 손쉽. 신속하게 mapping하여 절제한 예를 경험하였다.. 게 성공적으로 절제한 예를 경험하였기에 보고하는 바. 시간이 많이 소모되고 재현성이 낮으며 기술적인 어 려움이 따르는 부정맥 절제술에 있어서 전통적인 활동 순서 mapping 방법의 한계를 극복하기위한 시도의 하. 이다.. 중심 단어:다전극 basket 도자・우중격 우회로.. 나로 이용되고 있는 것이 다전극 basket 도자로서 최. REFERENCES. 근 몇몇 보고를 통하여 복잡한 부정맥, 특히 수술후 심. 1) Leather RA, Leitch HW, Klein GJ. Radiofrequency catheter. 방빈맥 및 심실빈맥 등의 진단과 치료에 있어 통상적인. ablation of accessory pathways: a learning experience. Am J Cardiol 1991;68:1651-55. 2) Lesh MD, Van Hare GF, Schamp DJ. Curative percutanneous catheter ablation using radiofrequency energy for accessory pathways in all locations: results in 100 consecutive patients. J Am Coll Cardiol 1992;19:1303-9. 3) Chen SA, Chiang CE, Chiou CW. Serial electrophysiological studies in the late outcome of radiofrequeny ablation for accessory atrioventricular mediated tachyarrhythmias. Eur Heart J 1993;14:734-43. 4) Kay GN, Epstein AE, Dailey SM. Role of radiofrequency ablation in the management of supraventricular arrhythmias: experience in 760 consecutive patients. J Cardio-. 방법으로는 어렵거나 재발시 한번 시도해 볼만한 대체 법으로 인정되고 있다.5)6) 우심방 전체의 전극도를 동 시에 얻을 수 있으면서 심박조율도 가능하여 복잡한 빈 맥의 편승(entrainemnt) mapping을 할 수 있다는 장점 도 있다.13) 최근에는 다전극 basket 도자의 양극성 전 극도와 계수화(digitized)된 이면성 방사선 투시의 공 간적 기준점들을 전산 재조합하여 3차원적으로 볼 수 있는 시스템도 개발되어 복잡한 부정맥의 활동순서 양. 1453.
(7) vasc Electrophysiol 1993;4:371-89.. 1998;98:2168-79.. 5) Davis M, Cooper M, Johnson DC, Uther JB, Richards DA,. 13) Schmitt C, Zrenner B, Schneider M, Karch M, Ndrepepa. Ross DL. Simultaneous 60-electrode mapping of ventricular tachycardia using percutaneous catheters. J Am Coll Cardiol 1994;24:709-14. Triedman JK, Saul JP, Weindling SN, Walsh EP. Radiofrequency ablation of intraatrial reentrant tachycardia after surgical palliation of congenital heart disease. Circulation 1995;91:707-14. El-Sherif N, Mehra R, Hough WB, Zeiler RH. Ventricular activation patterns of spontaneous and induced ventricular rhythms in canine one day old myocardial infarction: evidence for focal and reentrant mechanisms. Circ Res 1982; 51:152-66. Schoels W, Reistivo M, Caref EB, Gough WB, El-Sherif N. Circus movement atrial flutter in canine sterile pericarditis model: activation patterns during entrainment and termination of single loop reentry in vivo. Circulation 1991;83:1716-30. Dillon Sm, Allessie MA, Ursell PC, Wit AL. Influences of anisotropic tissue structure on reentrant circuits in the epicardial border zone of subacute canine infarcts. Circ Res 1988;63:182-206. Khoury DS, Taccardi B, Lux BL, Ershler PR, Rudy Y. Reconstruction of endocardial potentials and activation sequences from intracavitary probe measurements: localization of pacing sites and effects of myocardial structure. Circulation 1995;91:845-63. Greenspon AJ, Hsu SS, Datorre S. Successful radiofrequency catheter ablation of sustained ventricular tachycardia postmyocardial infarction in man guide by a multielectrode basket catheter. J Cardiovasc Electrophysiol 1997;8:565-70. Schalij MJ, Rugge PV, Siezenga M, Velde ET. Endocardial activation maping of ventricular tachycardia. Circulation. G, Deisenhofer I, et al. Clinical experience with a novel multielectrode basket catheter in right atrial tachycardias. Circulation 1999;992:414-22. Triedman JK, Jenkins KJ, Colan SD, Saul JP, Walsh EP. Intraatrial reentrant tachycardia after palliation of congenital heart disease: characterization of multiple macroreentrant circuits using fluoroscopically based three dimensional endocardial mapping. J Cardiovasc Electrophysiol 1997;8:259-70. Jenkins KJ, Walsh EP, Colan SD, Bergau DM, Saul JP, Lock JE. Multipolar endocardial mapping of the RA during cardiac catheterization: description of a new technique. J Am Coll Cardiol 1993;22:1105-10. Triedman JK, Jenkins KJ, Colan SD, Van Praagh R, Lock JE, Walsh EP. Multipolar endocardial mapping of the right heart using a basket catheter: acute and chronic animal studies. Pacing Clin Electrophysiol 1997;20:51-9. Khoury DS, Taccardi B, Lux BL, Ershler PR, Rudy Y. Reconstruction of endocardial potentials and activation sequences from intracavitary probe measurements: localization of pacing sites and effects of myocardial structure. Circulation 1995;91:845-63. Peters N, Jackman W, Schilling R, Beatty G, Davies W. Initial experience with mapping human endocardial activation using a novel non-contact catheter mapping system. Pacing Clin Electrophysiol 1996;19(ptII):600. Ben-Haim SA, Gepstein L, Hayam G, Ben-David J, Josephson ME. A nonfluoroscopic electroanatomical mapping system. Pacing Clin Electrophysiol 1996;19(ptII):709. Gepstein L, Hayam G, Ben-Haim SA. A novel method for nonfluoroscopic catheter based electroanatomical mapping of the heart: in vitro and in vivo accuracy results. Circulation 1997;95:1611-22.. 6). 7). 8). 9). 10). 11). 12). 1454. 14). 15). 16). 17). 18). 19) 20). Korean Circulation J 2000;30(11):1448-1454.
(8)
수치

관련 문서
Catheter ablation of accessory atrioventricular pathway ( Wolff-Parkinson-White syndrome ) by radiofre- quency current. Major coronary sinus abnormalities : Identification
Closed chest catheter desiccation of the atrioventricular junc- tion using radiofrequency energy: a new method of catheter ablation.. Jackman WM, Wang XZ, Friday KJ, Roman CA, Moulton
Radiofrequency catheter ablation (RFCA) as a treatment option for ventricular tachycardia (VT) is an important non- pharmacological alternative or adjunct to antiarrhythmic agents. 1)
Radiofrequency (RF) catheter ablation has become the treatment of choice for supraventricular tachycardia (SVT) in patients with Wolff-Parkinson-White (WPW) syndrome. 1)2)
Curative surgery for atrioventricular junctional ( “AV nodal” ) reentrant tachycardia. 4) Epstein LM, Scheinman MM, Langberg JJ, Chilson D, Goldberg HR, Griffin JC.
ABSTRACT Background:Although radiofrequency catheter ablation RFCA is useful in the treatment of idiopathic ventricular tachycardia, particularly in cases of right ventricular
W, Kalbfleisch S, Morady F:Radiofrequency catheter ablation of accessory atrioventricular connections in 25 0 patients : Abbreviated therapeutic approach to Wolff-
Radiofrequency Ablation of Liver Cancer Early Evaluation of Therapeutic Response with Contrast Enhanced Ultrasonography Dongil Choi, MD Hyo K Lim, MD Won Jae Lee, MD Seung Hoon Kim, MD
