대장암은 소아에 있어서 대단히 드물다. 점액을 분비하는 선암종이 대장암의 가장 흔한 유형인데, 그 대부분이 인환 세 포(signet ring cell) 암종이다. 성인에서는 대장암의 예후가 비 교적 양호한 반면, 소아에서는 나쁜 조직학적 특성과 진단의 어려움 때문에 예후가 상당히 불량하다 (1). 대장 선암종이 있는 소아 환자의 증상은 비특이적이어서 그 진단이 어려운 경우가 많은데 (2-4), 특히 소아 대장암이 파열되어 악성 복수 와 함께 복강 전부에 파종된 경우는 굉장히 드물 뿐만 아니라 수술전 진단도 거의 불가능하다.
저자들은 파열된 점액성 선암종으로 확진된 1예를 경험하 여 그 방사선학적 소견을 보고하고자 한다.
증례 보고
6개월 전부터 점액이 섞인 혈변과 복부 팽만이 있었으며, 내원 2일 전부터 고열, 담즙성 구토, 설사, 복통, 복부 팽만이 있는 1 4세 남아가 본원에 내원하였다. 환아의 체중은 최근 2 개월간에 2 K g이 감소되었다.
대변의 잠혈 검사는 양성이었고, 복수의 배양 검사에서 대 장균이 동정되었다. Carcinoembryonic antigen(CEA)과 a l p h a f e t o p r o t e i n은 정상 소견을 보였다.
단순 복부 촬영에서는 다량의 복수로 인해 복부 전체가 뿌 옇게 보였고 정상적인 장내 가스가 잘 관찰되지 않았다. 복부 초음파 검사에서는 복수와 함께 하행 및 S 결장 부위에서 대 장의 벽이 비후되고 그 후방 및 내측으로 경계가 불분명한 고 형 종괴가 관찰되었다 (Fig. 1). 조영 전후의 복부 전산화단층
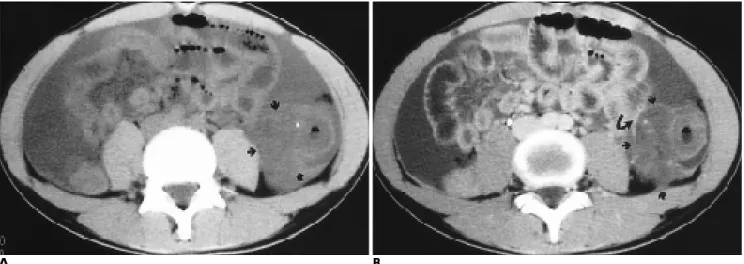
촬영(computed tomography, 이하 C T )에서는 하행 및 S자 결 장의 벽이 국소적으로 비후 되어 있었고, 그 내측과 후방에 아 주 작은 석회화를 동반하면서 불분명한 경계를 가지는 큰 종 괴가 발견되었다. 이 종양은 조영제 정맥 주입 후에 정상적인 장벽에 비해 덜 조영 증강되는 소견을 보였다. 다량의 복수와 함께 대망과 장간막 내의 지저분한 음영 및 소장벽의 유착이 있어, 악성 종양의 복강내 파종을 의심할 수 있었다 (Fig. 2).
좌측 결장 반절제술(hemicolectomy), 횡행 결장루 설치술 (transverse colostomy) 및 장 유착 분리 수술( a d h e s i o l y s i s )이 실시되었는데, 하행 및 S상 결장에 위치한 약 9cm 길이의 윤 상 종괴가 직경 약 1mm 크기의 S상 결장 천공을 동반하고 있었다. 복강 내에는 다량의 염증성 복수, 장 유착, 그리고 장
대한방사선의학회지 2 0 00;42: 6 95-6 9 7대장암은 소아에 있어서 대단히 드물고, 나쁜 조직학적 특성과 진단의 어려움 때문에 그 예후가 상당히 불량하다. 저자들은 복통, 설사, 발열로 내원한 1 4세 남아에서 발생한 하행 및 S자 결장의 점액성 선암종이 파열되어 복강 전체에 파종된 1예를 보고하고자 한다. 초음파 검사 및 전산화 단층 촬영에서 하행 및 S자 결장 벽의 비후와 석회화 및 거의 조영 증강되 지 않는 저음영 부분을 포함한 연부 조직 종괴가 다량의 복수와 함께 발견되었다. 소아의 대장 종양이 영상 소견에서 저음영 부분을 함유하고 석회화를 동반하며 공격적인 파종 양상 을 보이면 그 감별 진단에 점액성 선암종을 우선적으로 포함시켜야 하겠다.
1충남대학교의과대학진단방사선과학교실
이 논문은 1 9 9 9년 8월 1 3일 접수하여 1 9 9 9년 1 2월 1 7일에 채택되었음.
─ 6 9 5 ─
소아 결장의 파열된 점액성 선암종: 1예 보고1
김 종 철・신 경 숙
Fig. 1. Transverse sonogram of the left flank in prone position shows thickened wall of a portion of bowel (arrowheads) with ill-defined soft tissue mass to the medial and posterior side of it (open arrows). Note ascites (a) between the bowel loops.
간막, 대망, 전(anterior) 복벽에 파종된 백색 결절들이 있었다.
종양은 융기된 채 윤상으로 결장벽 전층과 주위의 지방 조직 까지 침범하였으며, 그 종괴의 중심 부위에는 궤양이 형성되 어 있었다 (Fig. 3). 현미경 검사에서 다량의 점액이 축적된 공간과 잘 분화된 신생 샘( g l a n d )들을 동반한 점액성 선암종 으로 확진되었다.
고 찰
대장암은 소아에서 굉장히 드물다. 대개는 1 0대 소년에서 발견되지만, 유아나 여아에서도 발견될 수도 있다 (5). 폴립증 (polyposis) 환아에서 대장암의 빈도가 높지만, 이 대장암은 흔히 성인이 될 때까지 잘 발현되지 않는다. 소아에서는 점액 성 선암종이 가장 흔한 대장암의 조직형이다. 환경적 요인, 음 식, 염색체 이상 등이 소아 대장암의 발현과 관련이 있다는
증거가 제시되고 있다 (5, 6).
청소년기 대장암은 점액성 선암종의 비율이 높고, 성인 대 장암에 비해 공격적이고 그 예후가 더 불량하여 복막, 복강, 간, 림프절 등으로 전이를 잘 한다 (7). 소아에서는 빈도가 극 히 낮은 대장암을 임상적으로 진단한다는 것이 어렵기 때문 에, 발견 당시에는 이미 그 종양이 성인 대장암 이상으로 커져 있을 가능성이 높다. 점액성 선암종은 젊고 어린 환자에서 흔 하고 또 인환 세포의 특징을 가질 경우가 많은데, 이 인환 세 포형은 점막하 성장으로 심각한 점막 이상을 초래하지 않으면 서도 긴 분절에 협착을 초래하는 미만성 침습형의 선암종으로 나타나기도 한다 (1). 저자들의 증례에서는 종양 내에 인환 세 포가 발견되지 않았지만 하행 및 S 결장에 걸쳐 약 9 c m의 긴 분절을 침범하였다. 그러나, 국내외의 다른 보고들과는 달리 본 증례는 점액성 선암종이 파열되어 복강 전반에 미만성으로 파종되면서 염증까지 동반한 특이한 양상을 보였다.
점액성 선암종은 종양의 50% 이상이 세포외( e x t r a c e l l u l a r ) 점액으로 구성될 때 병리학적으로 진단될 수 있다 (1). 점액이 고여 있는 부분은 석회화를 동반할 수 있어서, 방사선 영상에 서도 이 석회화가 발견되면 점액성 선암종일 것이라는 조직학 적 진단이 어느 정도 가능해진다. 이 점상의(punctate) 석회화 는 점액성 선암종의 원발 부위뿐만 아니라 전이 부위에도 존 재할 수 있다 (1, 6). 저자들의 증례에서도 소량의 점상 석회화 가 하행 및 S자 결장에 발생한 종괴 내에서 발견되었다.
점액성 선암종 내에는 세포에서 분비하는 점액이 풍부할 수 있기 때문에, 점액이 다량 축적된 종양 부분은 C T에서 수액과 비슷한 저음영으로 조영 증강이 잘 안 된다 (1). 그러므로 C T 에서 수액과 비슷한 저음영의 종괴가 위, 대장, 직장 등에서 관찰되면 점액성 선암종을 감별진단에 포함시켜야 할 것이다.
저자들의 증례에서도 종양의 대부분이 저음영으로서 일부분 을 제외하고는 전체적으로 조영 증강이 잘 되지 않았다.
김종철 외 : 소아 결장의 파열된 점액성 선암종
─ 6 9 6 ─
Fig. 2. A .Precontrast CT scan shows massive ascites and a large soft tissue mass with small calcification in the descending colon (arrows).
B . Postcontrast CT scan reveal an ill-defined poorly enhancing mass (arrows) with tiny calcified foci. Note the indistinct borders of the medial and posterior aspects of the tumor and the adjacent small bowel loop (curved arrow), suggesting adhesion between them. Conglomeration of small bowel loops, dirty mesenteric fat, and ascites suggest carcinomatosa peritonei.
A B
Fig. 3. The gross appearance of the surgical specimen reveals thickened and ulcerated colonic wall, resulting in luminal nar- rowing (arrows).
결론적으로 소아 환아의 방사선학적 검사에서 대장의 점막 종괴(mucosal mass)가 관찰되면 비록 그 빈도는 희박하더라 도 대장암의 가능성도 고려해야 할 것이다. 특히 소아의 대장 종양이 C T에서 수액과 비슷한 저음영을 보이고 석회화를 동 반하며 공격적인 파종 양상을 보이면 점액성 선암종을 감별 진단에 우선적으로 포함해야 할 것이다.
참 고 문 헌
1 . Buetow PC, Buck JL, Carr NJ, Pantongrag-Brown L, Colorectal adenocarcinoma: radiologic pathologic correlation. R a d i o G r a p h i c s 1 9 9 5 ; 1 5 : 1 2 7 - 1 4 6
2 . Gupta SK, Caballes RL. Adenocarcinoma of colon in a child.
J Pediatr Gastroenterol Nutr 1986;5:973-6
3 . 윤치호, 이경애, 유정모, 최순희, 조규근. 소아의원발성대장암 1 예. 소아과학회지1 9 8 5 ; 2 8 : 8 0 - 8 4
4 . 김경남, 이원익, 손성철, 이풍만. 소아의원발성결장교양암 1예.
소아과학회지1 9 8 3 ; 2 6 : 3 9 7 - 4 0 1
5 . Silverman FN, Kuhn JP. The colon. In C a f f e y’s pediatric X-ray diag- n o s i s, 9th ed. St Louis: Mosby, 1993:1117-1118
6 . Fuchs CS, Giovannucci EL, Cloditz GA, Hunter DJ, Speizer FE, Willett WC. A prospective study of family history and the risk of colorectal cancer. N Eng J Med 1 9 9 4 ; 3 3 1 : 1 6 6 9 - 7 4
7 . Wilson RE, Donohue JH. Neoplasia of the colorectum. In Philips SF, Pemberton JH, Shorter RG, eds. The large intestine: physiology, pathophysiology, and disease. New York, NY: Raven, 1991:521-547 대한방사선의학회지 2 0 00;42: 6 95-6 9 7
─ 6 9 7 ─
J Korean Radiol Soc 2000;42:6 95- 6 9 7
Ru p t u red Mucinous Ad e n o c a rcinoma of the Colon in a Child: A Case Re p o rt1
Jong Chul Kim, M.D., Kyung Sook Shin, M.D.
1Department of Diagnostic Radiology, Chungnam National University School of Medicine
Carcinoma of the colon is extremely rare in pediatric patients, and due to the preponderance of poor histo- logical characteristics and the difficulty of diagnosis, the prognosis in children is quite unfavorable. We de- scribe a case of ruptured and disseminated mucinous adenocarcinoma of the descending and sigmoid colon in a 14-year-old boy with abdominal pain, diarrhea and fever. Ultrasonography and computed tomography re- vealed a large soft tissue mass containing tiny calcifications and poorly enhanced hypodense portions in the thickened descending and sigmoid colon, as well as abundant ascites. Where images reveal a mass with low at- tenuation, calcifications, and aggressive dissemination, mucinous adenocarcinoma may be preferentially in- cluded in the differential diagnosis of a pedriatic colon tumor.
Index words :
Children, gastrointestinal tract Colon, neoplasms
Colon, CT
Address reprint requests to : Jong Chul Kim, M.D., Department of Diagnostic Radiology, Chungnam National University School of Medicine 640, Daesa-dong, Jung-ku, Taejeon 301-040, Korea.
Tel. 82-42-2220-7835 Fax. 82-42-2253-0061 E-mail: [email protected]
─ 698 ─
국외 개최 학술대회[ 1 ]
■ 3RD INTERVENTIONAL MRI SYMPOSIUM (2000년5월12-13일)
v e n u e : Renaissance Hotel, Leipzig, Germany.
c o n t a c t : Dr. J.P. Schneider, Kl. &Polikl.f.Diagn.Radiologie, Univ. Leipzig, Liebigstrasse 20A, D-4103 leipzig, G e r m a n y .
(tel: 49-341-9718100; fax: 49-341-9618135;
E-mail: [email protected])
■ RADIOLOGICAL ULTRASOUND COURSE (2000년 5월 15-19일)
v e n u e : Winston-Salem, NC, USA.
c o n t a c t : Wake Forest Univ. Sch.. of Med., Center for Medical Ultrasound, Medical Center Boulevard, Winston-Salem, NC 27157-1039, USA.
(tel: 1-336-7164505; fax: 1-336-7164204 E-mail: [email protected])
■ 2000 MEETING OF THE AMERICAN COLLEGE OF MEDICAL PHYSICS (2000년 5월 15-20일)
v e n u e : Whistler, BC, Canada.
c o n t a c t : Am. coll. of Medical Physics, 1891 Preston White Drive, Reston, VA 22091, USA.
(tel: 1-703-6488966)
■ MID YEAR CONFERENCE AMERICAN OSTEOPATHIC COLLEGE OF RADIOLOGY (2000년5월18-21일) v e n u e : Ritz Carlton, Dearborn, MI, USA.
c o n t a c t : Rhonda Boehner, 119 E 2nd Street, Milan, MO 63556, USA.
(tel: 1-816-2654011; fax: 1-816-2653494)
■ ANNUAL MEETING SOCIETY OF THORACIC RADIOLOGY (2000년 5월 21-23일)
v e n u e : Inter Continental Willard, Washington, DC, USA.
c o n t a c t : Ryan Gibson, P.O. Box 1925, Roswell, GA 30077-1925, USA.
(tel: 1-770-6419773)
■ ERASMUS COURSE ON MAGNETIC RESONANCE IMAGING (EMRI): ABDOMINAL MRI IN PISA (2000년5월 21- 2 4일)
v e n u e : Benedettine Congress Center, Pisa, Italy.
c o n t a c t : Prof. Dr. Bartolozzi, University of Pisa, Via Roma 67, I-56100 Pisa, Italy.
(tel: 39-050-992509; fax: 39-050-551461 E-mail: [email protected])
■ 37TH ANNUAL CONGRESS AND 23RD POSTGRADUATE COURSE OF THE EUROPEAN SOCIETY OF PAEDIATRIC RADIOLOGY (E.S.P.R) (2000년 5월 22- 2 6일)
v e n u e : Hotel Altis, Lisbon, Portugal.
c o n t a c t : Congress Secretariat, Eurocongressos, Apartado 9880, p-1911 Lisboa Codex, portugal.
(tel: 351-1-8472577; fax: 351-1-8473746 E-mail: [email protected])
■ 7TH SPECIAL TOPIC SEMINAR: NEW DEVELOPMENTS IN CONTRAST AGENT RESEARCH (2000년 5월 25- 2 6일) v e n u e : Hotel corinthia Palace, San Anton, Malta, Greece.
c o n t a c t : Mr. Paolo Bianco, Travel Concept, Neue Grosse Bergstrasse 4-6, D-22767 Hamburg, Germany.
(tel: 49-40-2794033; fax: 49-40-2799816 E-mail: [email protected])
■ 30TH ANNUAL CONFERENCE OF THE FLEISCHNER SOCIETY (2000년5월 26- 2 8일)
v e n u e : Portopia Hotel, Kobe, Japan.
c o n t a c t : Pam Waslawski, Int. Meeting Managers, Inc., 4550 Post Oak Place, Suite 342, Houston, Texas 77027, USA.
(tel: 1-713-9650566; fax: 1-713-9600488 E-mail: [email protected])
■ ERASMUS COURSE ON MAGNETIC RESONANCE IMAGING (EMRI): CENTRAL NERVOUS SYSTEM I IN TOULOUSE (2000년 5월 27- 3 1일)
v e n u e : University Paul Sabatier, Toulouse, France.
c o n t a c t : Prof. I. Berry, Dept. of Nuclear Medicine, Ho^pital Rangueil, F-31403 Toulouse Cedex 4, F r a n c e .
(tel: 33-561322870; fax: 33-561322754 E-mail: [email protected])
■ 4TH ASIAN-PACIFIC CONGRESS OF CARDIOVASCULAR AND INTERVENTIONAL RADIOLOGY
(2000년 5월 28일-6월 1일) v e n u e : Singapore, Singapore.
c o n t a c t : Prof. Lenny Tan, M.D., Dept. of Diagn. Radiology, NUH, Lower Kent Ridge Road, Singapore 119074, S i n g a p o r e .
(tel: 65-7724210; fax: 65-7730190)
■ IMAGING TOGETHER 2000: THE 54TH NORDIC RADIOLOGICAL CONGRESS/THE 14TH NORDIC CONGRESS FOR RADIOGRAPHERS
(2000년 5월 28- 3 1일)
v e n u e : Marina Congress Center, Helsinki, Finland.
c o n t a c t : Congress Team, Area Travel Agency Ltd., P.O. Box 6 (Pa¨i va¨rinnankatu 1), FIN-00251 Helsinki, Finland.
(tel: 358-9-818383; fax: 358-9-4775811 E-mail: [email protected])
■ CONFERENCE ON BREAST CANCER (2000년 6월) v e n u e : New York, NY, USA.
c o n t a c t : ESO USA, R. Boschi-Belgin,
872 madison Avenue-2B, New York, NY 10021, USA.
(tel: 1-212-6289090; fax: 1-212-5176089 E-mail: [email protected])