Skin appendageal tumors are generally diagnosed ac- cording to their histology, and imaging examinations are not routinely performed. However, when a large soft tis- sue mass exists and malignancy is suspected, then imag- ing may be helpful to scrutinize the nature of the tumor.
Malignant nodular hidradenoma is a rare aggressive ma- lignant tumor of the eccrine sweat glands.
Approximately 50 cases had been documented up to the year 2004 in the English literature, and most cases have been reported in the pathology literature with only lim- ited clinical and radiological information (1). We present here the radiological findings of a malignant nodular hidradenoma of the upper arm in a 71-year-old woman.
Case Report
A 71-year-old woman presented with a recurrent tu- mor of the left upper arm. The lesion was first noted 50 years earlier as a small, bean-sized, cutaneous nodule, and it had been stable for 46 years. About 4 years before
Malignant Nodular Hidradenoma: A Case Report1
Jin Hwan Kwon, M.D., Jin Do Huh, M.D., Kyung Soon Jeong, M.D., Mi Hee Jung, M.D., Ji Ho Ko, M.D., Jae Do Kim, M.D.2, Bong Kwon Chun, M.D.3, Seon-Joo Lee, M.D.4
1Department of Diagnostic Radiology, Gospel Hospital, College of Medicine, Kosin University
2Department of Orthopedic Surgery, Gospel Hospital, College of Medicine, Kosin University
3Department of Pathology, Gospel Hospital, College of Medicine, Kosin University
4Department of Diagnostic Radiology, Busan Paik Hospital, College of Medicine, Inje University
Received March 9, 2007 ; Accepted April 18, 2007
Address reprint requests to : Jin Do Huh, M.D., Department of Diagnostic Radiology, Gospel Hospital, College of Medicine, Kosin University, 34 Amnam-dong, Seo-Gu, Busan 602-702, Korea
Tel. 82-51-990-6341 Fax. 82-51-255-2764 E-mail: [email protected]
Malignant nodular hidradenoma is a rare skin appendageal tumor, and its imaging findings have not been previously described. We experienced the case of a large malig- nant nodular hidradenoma of the left upper arm in a 71-year-old woman. MRI re- vealed a large, lobular, poorly circumscribed, soft tissue mass at the left upper arm, and the mass showed homogeneous enhancement. 18F-FDG PET/CT showed hyper- metabolic activity in the left upper arm mass with a maximal standard uptake value of 19.
Index words :Skin, neoplasms Skin, MR
Skin, radionuclide studies
Fig. 1. A 71-year-old woman with malignant nodular hidrade- noma. A photograph of the malignant nodular hidradenoma showed a 12×10×4 cm sized ulcerated fungating mass that involve the left upper arm.
was then performed and the diagnosis of benign sweat gland tumor was made. Two years later, the nodule be- gan to rapidly enlarge with ulceration and hemorrhagic discoloration. At the time of admission, a superficial 12
×10×4 cm mass lesion was palpated on the postero-lat- eral aspect of the left upper arm (Fig. 1). The tumor was elastic and firm and it was not associated with any mo- tor or sensory disturbance.
Plain radiographs demonstrated a lobular soft tissue
A B C
Fig. 3. The axial T1-weighted (A) and fat-suppressed T2-weighted (B) images showed an ill defined mass (arrow) in the subcuta- neous tissue of the upper arm. The mass was hypointense to muscle on the T1-weighted image and hyperintense to muscle on the fat-suppressed T2-weighted image. The axial fat-suppressed T1-weighted image (C) after intravenous administration of gadolinium demonstrated homogeneous enhancement (arrowhead). The underlying adjacent musculature was involved.
Fig. 2. Conventional radiography showed a multilobular soft tissue mass at the distal part of the upper arm. No bony abnor- mality in the adjacent humerus was found.
Fig. 4. The fused PET-CT image showed an area of hyperme- tabolism (arrow, Standard Uptake Value=19) corresponding to the soft tissue mass in the left upper arm.
mass with no internal calcification. No definite change such as erosion, periosteal reaction or invasion was not- ed in the adjacent bone (Fig. 2). The MR images showed a soft tissue mass in the subcutaneous layer of the lateral epitrochlear region, and the mass extended to the adja- cent muscular layer. The tumor’s margin was poorly de- fined and the lesion was nearly homogenous in appear- ance. The mass showed an intermediate to low signal in- tensity on the T1-weighted images, and near uniform in- termediate to high signal intensity on the fat-suppressed T2-weighted images. On the fat-suppressed T1-weighted MR images with contrast enhancement, the mass demonstrated diffuse enhancement without any areas of necrosis (Fig. 3). The fused PET-CT showed hyperme- tabolic activity in the mass with a maximal standard up- take value of 19. This finding was suggestive of a malig- nant lesion. No other sites of abnormal focal FDG up- take were apparent on the whole-body PET-CT scan (Fig. 4).
The patient underwent an excisional biopsy and split- thickness skin grafting. The histopathologic study showed an ill-defined, epithelial neoformation that was formed by lobules of clear polygonal cells at both the deep dermis and the subcutaneous tissue. There was a second group of smaller cells that had a basaloid aspect, and a few of them showed slight atypia (Fig. 5). The fi- nal pathologic analysis confirmed the diagnosis of malig- nant nodular hidradenoma. No evidence of lymph node metastases or distant metastases was found.
Discussion
Malignant nodular hidradenoma is a rare aggressive malignant tumor of the eccrine sweat glands. Several synonyms for malignant nodular hidradenoma have ap- peared in the literature: clear-cell hidradenocarcinoma, malignant clear-cell hidradenoma, solid-cystic adenocar- cinoma, malignant acrospiroma, malignant clear-cell myoepithelioma and clear-cell eccrine carcinoma (1).
This tumor’s incidence has been reported to be 6% of all the eccrine gland carcinomas (2). The tumor usually pre- sents as a solitary painless papule or nodule, with a slow growing course, on the head, trunk or distal extremities, and sometimes there are multiple tumors (3). The usual age of occurrence is older than 50 years with an equal sex distribution. The prognosis for the 5-year survival af- ter excision is less than 30% (1, 3). Malignancy can oc- cur de novo in normal skin or it can develop within a pre-existing benign eccrine tumor (4-6). Considering the very long history of our patient, we believe the tu- mor started as a benign tumor and it then turned into a malignant one.
Histopathogically, the tumor cells usually have char- acteristic vacuolated cytoplasm (clear-cell change) ow- ing primarily to glycogen accumulation; however, an- other possibility is that such cells are expressing my- oephithelial differentiation, based on the focal coexpres- sion of keratin and actin in some tumor cells (1, 3).
Another characteristic feature of malignant nodular
A B
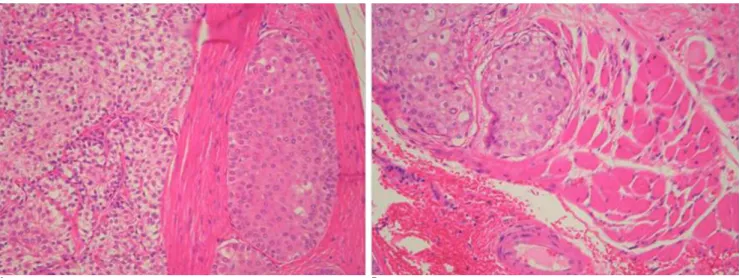
Fig. 5. A. Microscopic examination of the tumor revealed proliferation of two types of cells, basoloid or squamoid cells and clear cells, and they formed a lobular pattern and also solid sheets (hematoxylin and eosin stain, magnification ×200).
B. A hidroadenoma with areas of malignant transformation was observed. Note the dispersed growth pattern with local invasion (hematoxylin and eosin stain, magnification ×200).
tures are histolgically analogous to the eccrine sweat duct (1).
Any reported MRI findings of benign hidradenoma are extremely rare, and only a few cases have been re- ported on. Reier et al. (7) reported on a plantar eccrine acrospiroma that was 1 cm in diameter, and this re- vealed a solid enhancing nodule. Maldjian et al. (8) re- ported that clear cell hidradenoma showed a complex cystic appearance with fluid levels that suggested hem- orrhage and there were enhancing mural soft tissue nod- ules. Tsurumaru et al. (9) reported that clear cell hidradenoma showed a solid and cystic appearance with fluid levels and an enhancing solid component. To the best of our knowledge, the MRI appearance of ma- lignant nodular hidradenoma has not been previously described. The tumor in our case was revealed to be a large sized, multilobular and poorly circumscribed mass with homogeneous enhancement. The cut surface of the resected specimens showed solid nests of neoplastic cells that featured basoloid and clear cells along with with higher cellularity, and this corresponded to the ho- mogenous enhancement on the contrast-enhanced MR images.
The value of the MR in this case was therefore similar to that in most soft tissue tumors, that is, to help define the extent of the tumor and to aid in the planning of surgery rather than providing a specific preoperative di- agnosis of the tumor. In our case, PET-CT has been shown to be useful in differentiating malignant from be- nign lesions and for excluding distant metastasis.
The best treatment to achieve cure is wide and deep excision. Recurrence is common after incomplete exci- sion. Metastases typically appear first in the regional lymph nodes, lung and bone. Radiotherapy is not effec-
metastatic disease, although its value has not been con- firmed (1, 3, 6).
In summary, malignant nodular hidradenoma typical- ly affects adult patients as a painless mass of the extrem- ities at the time of presentation. Malignant nodular hidradenoma may manifest on MR images as a multi- lobular and poorly circumscribed mass with homoge- nous enhancement that involves the adjacent muscle.
Despite the relative rarity of this tumor, it should be in- cluded in the differential diagnosis when finding subcu- taneous masses in the extremities of adult patients.
References
1. Ohta M, Hiramoto M, Fujii M. Nodular hidradenocarcinoma on the scalp of a young woman: case report and review of literature.
Dermatol Surg 2004;30:1265-1268
2. Wu H, Elenitsas R. Malignant nodular hidradenoma in a patient with neurofibromatosis type 1: a case report and review of the lit- erature. Cutis 2001;68:273-278
3. Waxtein L, Vega E, Cortes R, Hojyo T, Dominguez-Soto L.
Malignant nodular hidradenoma. Int J Dermatol 1998;37:225-228 4. Galadari E, Mehragam AH, Lee KC. Malignant transformation of
eccrine tumours. J Cutan Pathol 1987;14:15-22
5. Lim SC, Lee MJ, Lee MS, Kee KH, Suh CH. Giant hidradenocarci- noma: a report of malignant transformation from nodular hidrade- noma. Pathol Int 1998;48:818-823
6. Khalil HMB, Yusuf H, Kaddour HS. Malignant eccrine hidradeno- ma of neck causing acute heart failure. Auris Nasus Larynx 2003;30:307-310
7. Reier AR, Farooki S, Ashman CJ, Miles L. MR imaging appearance of plantar eccrine acrospiroma (sweat gland tumor). AJR Am J Roentgenol 2002;179:1079-1080
8. Maldjian C, Adam R, Bonakdarpour A, Robinson TM, Shienbaum AJ. MRI appearance of clear cell hidradenoma. Skeletal Radiol 1999;28:104-106
9. Tsurumaru D, Torii Y, Kajiwara T, Shimoda Y, Yoshikane K, Irie K, et al. MRI of clear cell hidradenoma. Radiat Med 2004;22:426- 428
대한영상의학회지 2007;56:579-583
악성 결절성 한선종: 증례 보고1
1고신대학교 복음병원 영상의학과, 2정형외과, 3해부병리과
4인제대학교 의과대학 부산백병원 영상의학과
권진환・허진도・정경순・정미희・고지호・김재도2・천봉권3・이선주4
악성 결절성 한선종은 매우 드문 피부 부속기 종양으로 알려졌다. 저자들은 71세 여자환자의 좌측 상완에 발생 한 악성 결절성 한선종 증례를 경험하였기에 영상학적 소견을 보고한다. 병변은 자기공명영상에서는 경계가 잘 그 려지지 않고 균등한 조영증강을 보이는 연부조직종양으로 관찰되었다. 18F-FDG PET/CT에서는 18F-FDG의 높 은 섭취증가를 보이며 SUV는 19로 측정되었다.