INTRODUCTION
With the exception of the ovaries, metastases to the female genital tract from extragenital cancers are uncommon (1, 2).
Uterine metastases are very rare and comprise less than 10% of metastases to the female genital tract (3). Extragenital cancers that can metastasize to the female genital tract include cancers of the breast, gastrointestinal tract, ovary, skin and kidney (1-3).
Although a few pathologic series (1, 3-7) describe metastases to the uterus, to our knowledge, the description of the imaging is limited to only a few studies and a case report in English liter- ature (2). We report and describe the imaging features of endo- metrial metastasis from colonic adenocarcinoma.
CASE REPORT
A 40-year-old woman with recurred colon cancer was fol- lowed. The patient was first admitted in November 2010 be-
cause of melena and intermittent abdominal pain. Initially, im- aging did not demonstrate any evidence of metastasis. She underwent a laparoscopic right hemicolectomy for transverse colon cancer, which proved to be a stage pT3N1M0 moderately differentiated adenocarcinoma. She received twelve cycles of ad- juvant chemotherapy using the FOLFOX regimen (5-fluoroura- cil, leucovorin and oxaliplatin). Follow-up studies were negative for recurrence or metastasis until July 2011.
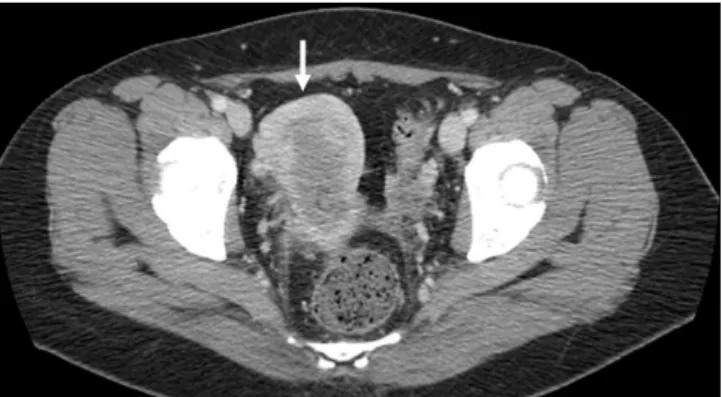
Contrast-enhanced abdomen and pelvis CT and whole-body positron emission tomography-CT (PET-CT) scans in February 2012 revealed multiple hepatic metastases. Whole-body PET-CT scan also showed a hypermetabolic lesion in the uterus [maximal standardized uptake value (max-SUV): 13.2]; however, the uter- ine lesion was thought to result from a menstrual physiologic up- take rather than a true lesion (Fig. 1). The patient subsequently received twelve cycles of chemotherapy using the FOLFIRI regi- men (5-fluorouracil, leucovorin and irinotecan) and after a one- month interval, a follow-up CT revealed stable disease.
J Korean Soc Radiol 2013;69(4):301-305 http://dx.doi.org/10.3348/jksr.2013.69.4.301
Received June 3, 2013; Accepted July 11, 2013 Corresponding author: Sung Bin Park, MD Department of Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, 102 Heukseok-ro, Dongjak-gu, Seoul 156-755, Korea.
Tel. 82-2-6299-3196 Fax. 82-2-6263-1557 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
Metastasis to the uterus is thought to be a very rare condition, and few imaging findings have been reported in the English literature. Here, we describe a case of endometrial metastasis from colon cancer, which was depicted using gray-scale and Doppler ultrasonography, CT and positron emission tomography-CT, to be a smoothly lobulated heterogeneous, predominantly endometrial mass in the uterus with increased vascular flow.
Index terms Uterine Metastases Uterine Mass Endometrium Colon Cancer Ultrasound
Imaging Findings of Endometrial Metastasis from Colon Cancer:
A Case Report
1결장암에서 자궁 내막 전이의 영상 소견: 증례 보고1
Nara Kim, MD
1, Sung Bin Park, MD
1, Jong Beum Lee, MD
1, Hyun Jeong Park, MD
1, Mi Kyung Kim, MD
2, In Gyu Hwang, MD
3, Ju Won Seok, MD
4Departments of 1Radiology, 2Pathology, 3Internal Medicine, 4Nuclear Medicine, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea
In October 2012, another contrast-enhanced abdomen and pelvis CT scan showed an increased in the size and number of hepatic metastases. Once again, it demonstrated a heteroge- neously enhancing, predominantly endometrial lesion in the uterus (Fig. 2). Lymph node enlargement was also noted in the left external iliac area. A whole-body PET-CT scan showed new- ly developed hypermetabolic metastatic lesions in both lungs, multiple bones, lymph nodes (paraaortic and left pelvic lymph nodes) and peritoneum as well as hepatic metastases (Fig. 3A).
The hypermetabolic lesion in the uterus was increased in size (Fig. 3B), compared to the previous PET-CT scan; therefore, the possibility of malignancy was considered.
The patient was premenopausal. She denied gynecologic symptoms, such as vaginal bleeding or change in menstruation.
There was no pelvic pain. Laboratory tests, including complete blood count, electrolytes and liver function tests, were all within normal range. To identify the endometrial lesion, an endovagi- nal ultrasonography (US) was performed. The US (IU 22, Phil- ips Medical Systems, Bothell, WA, USA) equipped with an end- viewing endovaginal 8-MHz transducer, identified a 4.0 × 1.4 cm, smoothly lobulated heterogeneous uterine mass, which was predominantly located in the endometrium. The mass was ex- tended from the uterine fundus to the endocervical canal (Fig.
4A). On Doppler US, increased vascular flow within the mass was evident (Fig. 4B).
Endometrial curettage was also performed. Histopathology results indicated that the uterine lesion was metastatic from co- lonic adenocarcinoma, identified from the previous hemicolec- tomy specimen. Immunohistochemical profiling also confirmed the presence of colonic adenocarcinoma (Fig. 5). Therefore, the findings established the diagnosis of uterine metastasis from co- lonic adenocarcinoma predominantly in the endometrium.
Two cycles of chemotherapy using a palliative third-line regi- men (bevacizumab and capecitabine) were administrated. A fol- low-up contrast-enhanced abdomen and a pelvis CT scan revealed that the uterine and hepatic lesions as well as lymphadenopathies regressed with a partial response.
DISCUSSION
The most common mode of secondary tumor involvement of the uterus is through a contiguous spread or direct extension, Fig. 1. Axial image of PET-CT shows a hypermetabolic lesion in the
uterus (arrow, max-SUV: 13.2). The uterine lesion was thought to be due to a menstrual physiologic uptake, rather than true lesion.
Note.-max-SUV = maximal standardized uptake value, PET-CT = pos- itron emission tomography-CT
Fig. 2. Axial image of contrast-enhanced abdomen and pelvis CT scan shows heterogeneously enhancing lesion in the uterus (arrow). Lymph node enlargement is also noted in left external iliac area (not shown).
Fig. 3. Follow-up PET-CT scan after eight months.
A. After eight months follow-up, whole-body PET-CT scan shows multiple hepatic metastases with newly developed hypermetabolic metastatic lesions in both lungs, multiple bones, lymph nodes (para- aortic and left pelvic lymph nodes), and peritoneum.
B. Follow-up axial image of PET-CT shows the increased size of the hypermetabolic lesion in the uterus (arrow, max-SUV: 10.9), compared with previous PET-CT (Fig. 1).
Note.-max-SUV = maximal standardized uptake value, PET-CT = pos- itron emission tomography-CT
B A
most often from a colorectal or bladder tumor (2). On the other hand, noncontiguous spread, such as metastasis to the uterus, is an infrequent clinical event (1-3). Although the reason for the rarity of this occurrence remains unclear, several possible causes have been postulated, including the centrifugal drainage of lym- phatics from the uterus, the fibrous nature of cervical stroma and underestimation of the incidence of such metastasis due to the lack of routine microscopic examination of the uterus at au- topsy (2, 6). The diagnosis of a direct tumor extension is often easily made because of a direct visualization of the adjacent in- vading tumor on imaging. However, metastasis to the uterus poses a more diagnostic challenge; imaging features include a diffuse, heterogeneously enhancing infiltrative process with preservation of the normal uterine shape (2). On T2-weighted MR imaging, uterine involvement displayed a partial or total loss of the hypointense signal in the cervical stroma or myome- trial junctional zone, depending on the location of involvement;
uterine involvement showed heterogeneous enhancement on contrast-enhanced MR images (2).
To the best our knowledge, this is the first case describing the sonographic features of the uterine metastasis in the English lit- erature. In this case, a smoothly lobulated heterogeneous uterine mass, which was predominantly located in the endometrium with extension into the endocervical canal, was noted on US with preservation of the uterine shape. The image showed a pol- ypoid mass rather than that of an infiltrative nature. Thus, pri- mary endometrial polyp, hyperplasia or malignancy may be the first choice. Considering the increased size of uterine lesions and other metastatic lesions at the follow-up, the metastasis should be differentiated.
Metastasis to the uterus occurs; however, the myometrium is generally thought to be more commonly involved rather than the endometrium (3). Furthermore, metastases to the endome- trium of the uterus from colon adenocarcinoma are extremely rare (1, 8). Mazur et al. (1) reported that the endometrium was the metastatic site for colon and rectum carcinoma in only 3.6%
of the 56 cases in their study.
US is the preferred initial diagnostic modality for gynecologic disease and captures the real-time images of organs and blood flow without radiation hazards (9). Additionally, US is almost always the first modality used in the radiologic work-up of en- dometrial diseases. The next steps often include sonohysterogra-
Fig. 5. Photomicrograph of a histologic specimen from endometrial curettage showing gland-forming atypical cell infiltration with neo- plastic glands adjacent to normal endometrial glands (hematoxylin- eosin, × 200). The histopathology findings were consistent with me- tastasis from colonic adenocarcinoma as identified from the previous hemicolectomy specimen. The immunohistochemical profile revealed positive staining for CK20 and negative for CK, which was strongly suggestive of colonic adenocarcinoma (not shown).
Fig. 4. Gray-scale and Doppler endovaginal US images.
A. Gray-scale endovaginal US demonstrates a 4.0 × 1.4 cm, smoothly lobulated heterogeneous mass located predominantly in the uterine en- dometrium with endocervical extension (arrow).
B. Doppler endovaginal US shows increased vascular flow within the mass (arrow).
Note.-US = ultrasonography B
A
REFERENCES
1. Mazur MT, Hsueh S, Gersell DJ. Metastases to the female genital tract. Analysis of 325 cases. Cancer 1984;53:1978- 1984
2. Metser U, Haider MA, Khalili K, Boerner S. MR imaging find- ings and patterns of spread in secondary tumor involve- ment of the uterine body and cervix. AJR Am J Roentgenol 2003;180:765-769
3. Kumar NB, Hart WR. Metastases to the uterine corpus from extragenital cancers. A clinicopathologic study of 63 cases. Cancer 1982;50:2163-2169
4. Lemoine NR, Hall PA. Epithelial tumors metastatic to the uterine cervix. A study of 33 cases and review of the liter- ature. Cancer 1986;57:2002-2005
5. Weingold AB, Boltuch SM. Extragenital metastases to the uterus. Am J Obstet Gynecol 1961;82:1267-1272
6. Daw E. Extragenital adenocarcinoma metastatic to the cervix uteri. Am J Obstet Gynecol 1972;114:1104-1105 7. Tarraza HM, Muntz HG, De Cain M, Jones MA. Cervical
metastases in advanced ovarian malignancies. Eur J Gyn- aecol Oncol 1993;14:274-278
8. Zannoni GF, Vellone VG, Fadda G, Petrillo M, Scambia G. Co- lonic carcinoma metastatic to the endometrium: the im- portance of clinical history in averting misdiagnosis as a primary endometrial carcinoma. Int J Surg Pathol 2011;19:
787-790
9. Derchi LE, Serafini G, Gandolfo N, Gandolfo NG, Martinoli C.
Ultrasound in gynecology. Eur Radiol 2001;11:2137-2155 10. Blake MA, Singh A, Setty BN, Slattery J, Kalra M, Maher
MM, et al. Pearls and pitfalls in interpretation of abdomi- nal and pelvic PET-CT. Radiographics 2006;26:1335-1353 phy and MR imaging to correlate with the US findings. If a PET-
CT scan is performed, an increased activity in the endometrium during the ovulatory and menstrual phases is often expected (10). As in this case, endometrial pathology needs to be differen- tiated from the normal prominent endometrium on the CT and PET-CT scan. Using US, a smoothly lobulated heterogeneous, predominantly endometrial uterine mass was detected and true endometrial pathology was favored. US may be the best modali- ty to analyze the endometrium and to guide further diagnostic work-up in these patients, such as endometrial biopsy.
Clinically, the most common presenting symptom of uterine metastasis is vaginal bleeding. The clinical symptoms may pre- cede the diagnosis of the primary tumor in up to 25% of these cases (2, 3). In one series, 27% of uterine metastases clinically presented as possible primary gynecologic lesions (2, 4). In gen- eral, abnormal vaginal bleeding is often a presenting symptom of pelvic malignancy, and it estimated that 10-20% of patients with vaginal bleeding have primary endometrial carcinoma (9).
Contrary to other reported cases of endometrial malignancy in- cluding metastasis, the patient in this case was asymptomatic.
US may still be a useful modality for evaluating endometrial diseases in asymptomatic patients.
In summary, we report a rare case of predominantly endome- trial metastasis in the uterus from colonic adenocarcinoma. The lesion was depicted on US, CT and PET-CT as a smoothly lobu- lated, heterogeneous and hypermetabolic mass with increased vascular flow and enhancement. In patients with other primary malignancies, the endometrial metastasis should be included in a differential diagnosis when evaluating the endometrial mass as well as endometrial polyp, endometrial hyperplasia or primary endometrial malignancy.
결장암에서 자궁 내막 전이의 영상 소견: 증례 보고1
김나라
1· 박성빈
1· 이종범
1· 박현정
1· 김미경
2· 황인규
3· 석주원
4자궁 전이는 아주 드물게 발생하며 자궁 전이의 영상 소견은 영문 문헌상으로 보고된 적이 거의 없다. 이에 저자들은 결장 암 환자의 자궁 내막 전이 증례의 영상 소견을 보고하고자 한다.
중앙대학교 의과대학 중앙대학교병원 1영상의학과, 2병리과, 3내과, 4핵의학과