Management of Malignancies Developing in AYA
Alex WK. Leung
1,3,4, Herbert HF. Loong
2, Teresa Tse
2and Chi-kong Li
1,3,4Departments of
1Pediatrics and
2Clinical Oncology, The Chinese University of Hong Kong, Prince of Wales Hospital,
3
Department of Pediatrics and Adolescent Medicine, Hong Kong Children Hospital,
4
Hong Kong Hub of Pediatric Excellence, The Chinese University of Hong Kong, Hong Kong SAR, China
Adolescent and young adult (AYA) with cancers have distinct spectrum of cancers as compared to younger and older age groups. The definition of age limits of AYA varies among countries, from 15-25 years to 12-39 years. The differences in age definition lead to variation in report of incidence, types of cancers and survival. In younger AYA patients, hematological malignancies are leading cause of cancers. In older AYA patients, testicular cancers are common in males while breast cancers and cervical cancers are predominant types in females. There is increasing incidence of AYA can- cers worldwide in the past two decades. Overall survival and treatment outcome of AYA cancer has been improving in the last few decades. Specialized centers for AYA with cancers provide more comprehensive care and have been reported to have supe- rior outcome. About 80% of AYA with cancers survive at 5 years after diagnosis but they are higher risk of developing second malignancies. Barriers to AYA cancer treat- ment included social economic status, insurance system and accessibility to clinical trials. Survivors of AYA cancers are also at higher risk dying from cardiovascular dis- eases and respiratory diseases. Survivorship program should be in place to enhance education and surveillance.
pISSN 2233-5250 / eISSN 2233-4580 https://doi.org/10.15264/cpho.2021.28.1.1
Clin Pediatr Hematol Oncol 2021;28:1∼13Received on October 5, 2020 Revised on December 31, 2020 Accepted on January 15, 2021
Corresponding Author: Chi-kong Li Department of Pediatrics, The Chinese University of Hong Kong, 6/F, Clinical Science Building, Prince of Wales Hospital, Shatin, NT, Hong Kong SAR, China Tel: +852-35052849 Fax: +852-26497859 E-mail: [email protected] ORCID ID: orcid.org/0000-0002-2810-5758 Key Words: Adolescent, Young adult, Cancer, Outcome
Copyright ⓒ 2021 Korean Society of Pediatric Hematology-Oncology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
Introduction
Adolescence and young adulthood represents a unique period in life with many important events going on, that includes but not limit to pursuing of higher education, starting of career, getting married and becoming parents.
Severe illness like cancer during this stage of life would be a major impact to an individual. The uniqueness of adolescent and young adult (AYA) cancers has gained much attention in the last two decades. The AYA Oncol- ogy Progress Review Group (PRG) of the National Cancer Institute (NCI) and the Lance Armstrong Foundation (LAF) published a report in 2006 focusing on issues related to
AYA cancer. It concerned the lack of progress in treat-
ment and survival of AYA with cancer when compared
to younger children and older adults. It also acknowl-
edged this discrepancy in survival improvement and des-
ignated this group of patients as vulnerable. Recommen-
dations were made aiming at closing the survival gap be-
tween AYA and other age groups with cancer [1,2]. Much
work is ongoing in the research of AYA cancers and there
is now a better insight of the distinct epidemiology, biol-
ogy, therapeutic needs, patterns of long term outcome,
co-morbidities and psychosocial needs of this group of
patients.
Definition of AYA
Young people aged 15 to 19 are usually being regarded as adolescents, while age over 20 as young adults. How- ever, there is no internationally unified definition on AYA age range [3,4]. In the past, the Surveillance, Epi- demiology, End Result (SEER) program of the NCI defined 29 years as the upper limit of age for young adults. In 2005, a broader age range of 15-39 years was proposed by the PRG of the NCI and LiveStrong Foundation in the US [1]. With the extension of upper limit of age range definition, there is increase in proportion of epithelial tumors (carcinoma) including breast, liver and lung tu- mors in AYA cancer spectrum [5]. Meanwhile, the age- group definition for AYA cancer service remains incon- sistent across the world: age 15-25 years in France, 15- 29 years in Italy, 14-30 years in Spain, and 15-24 years in United Kingdom and Australia [6,7]. Recent surveys in Europe and Asia also found significant variation in per- ceived definition of age range for AYA among health care providers (HCP) [4,8].
Epidemiology
Cancer is one of the leading causes of non-accidental death among AYA subjects in high income countries (HIC) [7,9-11]. The incidence rate of cancer in AYA pop- ulation has been reported to be 4 to 8 times higher than in children age below 15 [9,12]. In the United States, nearly 70,000 AYA aged between 15-39 years are diag- nosed with cancer each year and this accounted for 5%
of all cancer cases [12,13]. Estimated at over 60,000 new patients per year, this group accounts for 2% of all in- vasive cancers in Europe [6]. A survey in Japan reported the AYA population contributes to 3.6% of all cancer cas- es in the country [11]. Globally, 1.2 million AYA aged 15-39 years were diagnosed to have cancer in 2018, with incidence of 42.2 per 100,000 person per year and this was accountable for 6.8% of all cancer diagnosis [9].
In many countries, incidence of AYA cancer is increas- ing over the last few decades [14], with an estimated in-
crease of 30% from the time period 1975-1979 to 2011-2015 and the rate is higher than that seen in younger and older individuals [9,13,15]. An increase of annual incidence rate of 0.6-2% was reported in England, Korea, the Netherlands, Latin America and in males in Australia [10].
From 2005 through 2014, incidence of AYA cancer in- creased by 0.6% to 1.4% per year in the US [9]. In Europe, during the period from 1991-2007, the annual percent change ( APC) of cancer in male and female was 0.85%
and 0.8%, respectively [6]. A recent analysis of global trend of AYA cancer found significant increase in cancer burden in 23 out of 41 countries, with the greatest in- crease observed in South Korea [14]. In South Korea, APC of cancer in AYA aged 15-39 year was 8.5% in the period from 2002-2012 [10]. This was due to a significant increase in incidence rate of thyroid cancer in female [10,14]. Diagnosis of thyroid cancer in AYA female in Korea is approximately 6 times more common than in male [10]. In another report, APC of cancer among Korea AYA aged 15-29 was 6.3% between 1999 to 2010 and it was 1.8% when thyroid cancer was excluded from analy- sis [10]. This dramatic increase in incidence of thyroid cancer is attributable to increase in surveillance and
“over-diagnosis” of indolent lesions which would not af- fect the individual if left-untreated [9,16,17].
Cancer in AYA is characterized by female predom- inance with incidence rate two times higher than male [3,9,18]. Top ranking cancers are breast cancer, thyroid cancer and cancer of cervix uteri (Fig. 1) [3,9,10]. Thyroid cancer has a significant sex predominance with age- standardized rate (ASR) at least 4 times higher in female than in male among young adults [3]. The sex predom- inance is not observed in younger AYAs aged between 15-24 according to reports in France and Australia [7,19].
Socio-economic development is also associated with
burden of cancer in different regions of the world. Socio-
economic development of a region can be categorized by
low, middle, high and very high according to Human
Development Index (HDI). Regions with very high HDI
have increased incidence rate of AYA cancer when com-
pared with low or medium HDI regions, with estimated
Fig. 1. Cancer diagnosis among AYA aged 15-39 years with data retrieved from the International Agency for Research on CI5plus database (http://ci5.iarc.fr/CI5plus). All except data from Japan is from year 2012 while data from Japan registry is from year 2010.
There are regional variations in spectrum of cancer across the registries, especially for melanoma which is far more common in US, UK, and Australia than in China, Japan, and Korea; while Korea has a much higher incidence of thyroid cancer. (A) Cancer diagnosis in AYA male. (B) Cancer diagnosis in AYA female. ASR, Age-standardized rate.
ASR of 64.5 vs. 46.2 cancer cases per 100,000 person per year [3]. Nevertheless, mortality rate from AYA cancer is lower in very high HDI regions than in low HDI regions [3,9]. The spectrum of cancer across the 4 HDI levels also varies, with thyroid cancer, testicular cancer and mela- noma more frequently occurring in high HDI regions.
Infection-related cancers, including those related to hepa- titis B virus, human papilloma virus (HPV), Helicobacter pylori, are relatively more prevalent in regions under transition. Nevertheless, breast cancer and cancer of cer- vix uteri are among the top five most common AYA can- cers across the four HDI categories [3].
Spectrum of AYA Cancer
It is observed that the incidence of cancer in AYA in- creases steadily with age [9,10]. Among AYA with can- cers, approximately 10% of subjects are aged 15 to 24 years and 90% are aged 25 to 39 years [11]. The spectrum of cancers in patients aged 15-39 years is distinct from that in younger and older age groups [6,20]. It also varies with age within the AYA group. In general, there is de- crease in percentage of embryonal tumors with increas- ing age, while percentage of carcinoma increases [12].
Fig. 1 depicts the spectrum of cancer diagnosis among
AYA with data retrieved from registries in North America,
Table 1. Incidence rate and common cancer types in different regions of the world Country/region Age range
(years) Study
period Annual incidence/
100,000 Most common cancer site/type
Global [3] 20-39 2012 ASR
43.4 Breast cancer, cervical cancer, thyroid cancer, leukaemia, colorectal cancer
Global [9] 15-39 2018 42.2 Breast cancer, cervical cancer, thyroid cancer Australia [7]
Australian Cancer Database
15-24 2000-2009 31.7 Melanoma, HL, testicular tumor, thyroid cancer, NHL
France [19] 15-24 2000-2008 ASR (per million)
254.1 Male
Gonadal GCT, Hodgkin disease, ALL Female
Hodgkin disease, thyroid cancer, melanoma Netherlands [69]
Netherlands Cancer Registry
15-29 2003-2009 ESR
Male: 39.1 Female: 37.1
Male
Testicular cancer, Hodgkin disease, melanoma Female
Melanoma, breast cancer, Hodgkin disease Japan [18]
Monitoring of Cancer Incidence in Japan Project
15-39 2009-2011 ASR (per million) 488.3
Male: 333 Female: 649.5
20-29 years:
Malignant germ cell gonadal tumour 30-39 years:
Female breast cancer Korea [10]
Korea Central Cancer Registry
19-29 1999-2010 ASR (per million) 279.9
Male: 196.4 Female: 367.8
Thyroid, NHL, stomach carcinoma, breast carcinoma, AML
ASR, age-standardized rate; ESR, European Standardized rate.
Europe, and Asia, in the International Agency for Re- search on Cancer’s CI5plus database (http://ci5.iarc.fr/
CI5plus).
In young adolescents aged 15-19, there is a higher percentage of cancers being hematological malignancies and brain tumors when compared with young adults aged 20-39 [13]. In younger subjects aged 15-24, hematolo- gical malignancies are the commonest type of cancers [11]. Incidence of acute lymphoblastic leukemia (ALL) is higher in younger AYA than in elder subjects [21]. Among those aged 25-39 years, testicular cancer is the most common type of cancer in male, whereas breast cancer and cancer of cervix uteri are the two most common type of cancers in female [11]. Osteosarcoma, Ewing sarcoma, gonadal germ cell tumor (GCT) and Hodgkin lymphoma are more frequent among AYA than in other age groups [9,12].
Globally in 2012, the most common cancer among young adults aged 20-39 are breast cancer, cervical can- cer, thyroid cancer, leukemia and colorectal cancer [3].
Table 1 listed incidence rate and spectrum of cancer in different parts of the world.
In view of the uniqueness of cancer spectrum in AYA, the International Classification on Childhood Cancer (ICCC) does not precisely reflect and capture the full spectrum of diseases. According to ICCC, many of the AYA cancers would fall into the category of “Other and unspecified carcinoma”, which includes carcinoma of breast, lung, gastrointestinal tract and urological system [22]. A dedicated classification scheme tailored to the circumstances and spectrum of AYA cancer is therefore proposed by Barr and Birch [23,24].
Acute Lymphoblastic Leukemia
ALL is one of the cancers which improvement is lag-
ging behind in AYA when compared with children. Most
of the survival difference between children and AYA in
Europe and the US was due to more significant improve-
ment of ALL survival in children [25]. In the last few dec-
ades, multi-institutional trials and progressive refine- ment of multi-agent protocols have resulted in sig- nificant improvement of treatment outcome for child- hood ALL. However, similar improvement was not seen in AYA ALL. 5-year event free survival of 50% to 60% is still not optimal when compared to pediatric patients [2,21,26].
Differences in biology of disease between AYA and young children could be a contributing factor to the in- ferior outcome. Increasing age is known to be associated with poor prognostic biological features including higher presenting white cell count, T-immunophenotype, Ph chromosome positive and Ph-like ALL [13]. Treatment protocols administered, site of treatment (pediatric vs.
adult cancer treatment units), rate of enrollment on clin- ical trials, adherence to treatment and social issues in- cluding insurance coverage are all possible factors at- tributing to the worse outcome [21,27,28]. Meta-analysis of 11 comparative studies including 2,489 patients showed pediatric-inspired regimen was superior to conventional adult therapy in treating AYA ALL age 16-39, albeit none of the studies was randomized trials. Pediatric-inspired regimen was having better event-free survival, lower all- cause mortality and relapse rate [27].
A retrospective study examined the treatment response and outcome on AYAs 16-20 years old with ALL who re- ceived treatment according to either Children Cancer Group (CCG) trials or Cancer and Leukaemia Group B (CALGB) trials, which were pediatric and adult coopera- tive group trials, respectively. The CALGB trials enrolled 759 patients (aged 16-81 years) and 124 of them were aged 16-20. Seven-year event free survival and overall survival (OS) were 63% and 67%, respectively for CCG treated patients and significantly better than patients en- rolled on CALGB trials (EFS 34%; OS 46%) despite similar complete remission rate. This study suggested superior efficacy of CCG approach in treating AYA ALL. However, patients in CCG trials were younger, with 85% of them aged 16-17, when compared with CALGB trials with 80%
of them aged 18-20 year [29].
The Japan Adult Leukemia Study Group (JALSG) stud- ied the feasibility and toxicity of ALL202-U protocol, a
pediatric-based regimen, in adolescents and young adults aged 15 to 24 with Ph-negative ALL. It also demonstrated marked improvement in outcome with ALL202-U proto- col when compared with JALSG ALL97 adult protocol with 5-year OS of 73% and 45% and disease free survival of 67% and 44%, respectively, with acceptable toxicity profile [30].
The National Comprehensive Cancer Network (NCCN) clinical practice guideline on ALL strongly recommends treatment in specialized centers [31]. Studies have exam- ined whether treating at adult centers or pediatric treat- ment units would affect outcome. Retrospective com- parative studies suggested AYAs with ALL who received treatment at pediatric centers were having better out- come than at adult centers. The difference was, at least in part, related to the treatment protocol intensity in- stead of site of treatment [28]. Population-based study in Canada on 290 ALL patients age 15-19 at the time of di- agnosis found comparable outcome among patients treat- ed at pediatric and adult centers, which was probably due to early introduction of pediatric-based regimens in adult centers [28]. The CALGB10430 study, based on a pediatric regimen of Children’s Oncology Group AALL0232 protocol, also demonstrated the feasibility, safety and significant improvement in survival in treating AYA ALL patients at adult treatment centers, with 3-years EFS of 59% and OS of 73% [32]. Treating AYA ALL at either pe- diatric or adult centers with pediatric-based regimen ap- pears to be a preferred option.
Soft Tissue Sarcoma
Soft tissue sarcoma (STS) is relatively uncommon and contributes to only 1% of all adult cancers and about 8%
of all cancers in AYA [20,33,34]. Little was known about
the true epidemiology of this heterogeneous group of
disease in AYA. Comparison of data is difficult with in-
consistency in age range definition of AYA across differ-
ent studies [33-35]. Accrual in clinical trials is sub-opti-
mal and is limited by the lack of tailored trials for this
heterogeneous group of disease [35]. Its importance in
AYA, however, should not be overlooked due to worse
treatment outcome when compared with other AYA can- cers like melanoma, Hodgkin lymphoma and germ cell tumors [9]. Patients with STS need multi-disciplinary management which usually involves medical or pediatric oncologist, radiation oncologist, and orthopedic surgeon.
The value of multi-disciplinary management is best illus- trated by management of sarcoma patients. A study in France on subjects aged >15 years with sarcoma ob- served that presentation to multi-disciplinary tumor board before initiation of treatment is beneficial with 2-year local relapse free survival 76.9% compared to 65.4% in those presented after initiation of treatment [36]. Cen- tralizing treatment in specialized centers for manage- ment of STS could be beneficial and enrolling patients in clinical trials should be advocated [35,37].
A report from the European Organization for Research and Cancer Treatment (EORTC) compared prognostic factors of STS in AYA and adults, with AYA defined as aged 15-29 and adults as over 30, who were enrolled in two randomized trial for STS. In both age groups, lower histological grading and smaller tumors were favorable prognostic factors. In the younger age group, tumor in extremities was a favorable prognostic factor while ben- efit of adjuvant therapy was only seen in adults aged ≥30 years [35].
In 2019, a population-based study of the Scandinavian Sarcoma Group Central Registry on 5,000 patients with STS, including AYA aged 18-39 years and older adults age over 40, reported differences between the two groups with regard to presentation, size of tumor, histological sub-type, treatment and survival outcome. There was no difference with regard to metastatic disease at the time of presentation. Better survival outcome was seen in AYA compared with older adults (Median survival 5.36 years vs. 3.96 years) with the exception of malignant periph- eral nerve sheath tumor [33].
Breast Cancer
Breast cancer is one of the most common cancer in young adult females with increasing incidence with age.
The proportion of breast cancer increases significantly
with age, accounting for less than 1% in adolescents and 29% in those aged 30-39 years [13]. Overall, 5.6% of all invasive breast cancer patients are diagnosed in AYA fe- males younger than age of 40 [38].
The proportion of AYA breast cancer being stage II to IV disease is higher in AYA than in women aged over 40 [38]. Likewise, in comparison with older females, the chance of having familial cancer predisposition, more aggressive clinical course and triple negative cancer is also higher in AYA females, thus conferring to a worse outcome of AYA with breast cancer [9,38]. In the US, 5-year survival rate for age less than 30 years and 40-49 years were 80.2% and 88.9%, respectively [38,39]. Similar finding is also reported in Korea, with 5-year relative survival (RS) of 86.8% and 91% for patients aged 15-29 years and ≥40 years, respectively [10].
Colon Cancer
In contrast to decreasing trend of incidence of color- ectal cancer in older individuals, the incidence rate of colon cancer in AYA is on the rise, [40-42] with left side of colon and rectum being more frequently involved [42,43]. However, there is variation of incidence trend between countries. In 2020, Gupta et al reported cancer incidence with data from CI5plus database in the time period between 1998 to 2012. Among 41 countries, colon cancer incidence was increasing in 17 countries and sta- ble in 24 countries [14]. Australia and New Zealand have the highest incidence of CRC. In the period between 1982 to 2007, incidence of CRC among AYA aged 15-39 increased by 3% per year in Western Australia [41]. Akin to breast cancer, a higher proportion of aggressive tumor subtypes of colon cancer with associated poorer survival are found in the AYA population as opposed to adults.
This includes colon cancers with mucinous histology,
and presence of mis-match repair defect and high mi-
crosatellite instability [43]. Nevertheless, a report from
Japan on 502 AYA with stage II to III CRC, 5-year OS was
better when compared with adults aged 65-74, with OS
100% vs. 93.6% for stage II and 87.4% vs. 82.2% for stage
III disease [44]. It was also observed that among CRC pa-
tients with completely resected stage I to III disease, dis- ease specific survival of AYA and older adults aged >40 was similar and was 86% and 87%, respectively, although more AYA received adjuvant therapy. These observations suggested that early diagnosis is important in AYA CRC and education of AYA on CRC symptoms and early colo- noscopy should be emphasized.
Testicular Cancer
Testicular cancer is the commonest cancer in AYA males with peak incidence in late 20s to early 30s [45].
The incidence rate showed significant geographical var- iations, with the highest incidence in Europe with age- standardized rate of 137.4 per million and lowest in Asia with ASR of 27.1 per million [45]. Mixed malignant GCT is the most common histological type among adolescents while the proportion of seminoma increases with age and it is the most common histology in older AYA sub- jects [46].
A population based study in the US showed adoles- cents were having more frequent regional or distant metastasis compared with adults. Nevertheless, cancer spe- cific survival for adolescents and adults were comparable (95% and 94%, respectively) and the favorable outcome was probably achieved at the cost of more aggressive surgical and other adjuvant treatments in younger sub- jects [47]. Long term treatment related morbidities in- cluding ototoxicity, increase risk of cardiovascular dis- ease and second malignant neoplasms, hypogonadism, pulmonary and kidney impairment should not be over- looked [46].
Cervical Cancer
Globally, cervical cancer is among the top 10 ranking cancers in incidence and mortality and is one of the 3 most common cancer in AYA females. HPV infection, es- pecially high-risk types 16 and 18, is a well-known etio- logical factor for cervical cancer and is transmitted via sexual activity. There are wide variations in surveillance data among different regions of the world and developed
countries are having lower age-standardized incidence rate and death rate compared with developing countries [48]. Global surveillance data also revealed variations in incidence trend among AYAs in different nations, with one third of countries showing decrease in incidence while some countries are observing increase in incidence [14]. As there is a lag time of 10 to 20 years for pre- cancerous changes to evolve into cervical cancer, wide- spread adoption of screening for precancerous changes by Pap test or high risk HPV virus surveillance and early intervention reduces incidence and mortality of cervical cancer [49,50]. The US Preventive Service Task Force recommends screening of females from age 21 onwards [50]. Other preventive measures include use of condom, mutual monogamy and HPV vaccination [51]. HPV vac- cine can be given to females as early as age of 9 years.
For girls age between 9-14 years, two doses of HPV vac- cine are recommended whereas 3 doses are needed for those aged 15-26 years [50]. A study done in Taiwan, however, found only 11.5% of adolescent females were informed of HPV vaccination by HCP [51]. Appropriate and timely delivery of information to adolescent girls on prevention of HPV infection should not be under-em- phasized.
Thyroid Cancer
Thyroid cancer is one of the most common cancer
among AYA and majority of them are papillary thyroid
cancer (PTC) [52]. AYAs with differentiated thyroid can-
cer generally have favorable outcome [53] and disease
free survival and overall survival are better compared
with adults age over 40 [52]. With increase in utilization
of ultrasonography screening, many countries are ob-
serving a surge of thyroid cancers due to over diagnosis
[17]. From 1993 to 2011, incidence rate of thyroid cancer
in Korea rocketed by a factor of 15, with 40,000 cases
diagnosed in 2011, while mortality figure remained sta-
ble [17]. It is known that many PTC could remain sub-
clinical and rarely result in mortality. Significant over-
diagnosis and subsequent dramatic increase in number
of patients receiving treatment, which is mainly surgery,
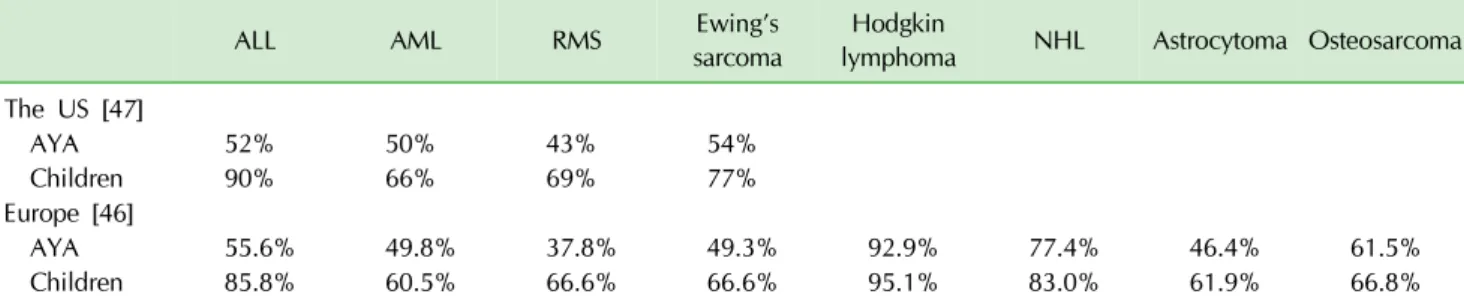
Table 2. 5-year relative survival of AYA and children with cancer common to both groups. Europe data from 27 European countries participating in EUROCARE-5 for AYA and children with cancer diagnosed in 2000-2007. US Data from NCI SEER database in the period from 2002-2006
ALL AML RMS Ewing’s
sarcoma Hodgkin
lymphoma NHL Astrocytoma Osteosarcoma The US [47]
AYA 52% 50% 43% 54%
Children 90% 66% 69% 77%
Europe [46]
AYA 55.6% 49.8% 37.8% 49.3% 92.9% 77.4% 46.4% 61.5%
Children 85.8% 60.5% 66.6% 66.6% 95.1% 83.0% 61.9% 66.8%
ALL, acute lymphoblastic leukaemia; AML, acute myeloid leukaemia; RMS, rhabdomyosarcoma; NHL, Non-Hodgkin lymphoma.
should prompt reconsidering the role of screening for thyroid cancer [17].
Survival Outcome
Five-year OS of AYA with cancer was 71% in mid- 1970s [13]. Overall survival and treatment outcome of cancer has been improving in the last few decades.
However, in 2006, the SEER and COG published an epi- demiology report on AYA with cancer and high-lighted a relative lack of progress in AYA cancer survival in the last quarter of the twentieth century when compared with younger and older individuals [12,54]. In retrospect, this lack of improvement could be explained by the hu- man immunodeficiency virus/acquired immunodeficien- cy syndrome (HIV/AIDS) epidemic during the 1980s to 1990s, which resulted in a surge of HIV related Kaposi sarcoma and lymphoma with poorer survival outcome, before the development of effective treatment for HIV infection [55].
Five-year RS of AYA with cancers diagnosed in the pe- riod 2002-2006 was 82.5%, with 14 cancer types having improvement in outcome when compared with results in 1992 [56]. In Europe, among AYA with cancer diagnosed during the period 2000-2007, 81% were alive at 5 years after diagnosis [6]. For those diagnosed in the period from 2008 through 2014, 5-year OS was 86% [13]. World- wide, 5-year RS of AYA with cancer is now in the range of 79% to 89% [9]. Survival outcome varies between dif- ferent regions of the world, partly because of the differ-
ence in age range on defining AYA, the inclusion of be- nign tumors in the analysis and the variation in incidence of types of cancer. Not to mention variations in socio- economic status (SES) which significantly impact on out- come, with mortality to incidence ratio (MIR) being 3 to 4 times higher in very low HDI regions when compared to countries with HDI [9].
Despite the outcome of AYA with cancer is now slight- ly better than children younger than 15, treatment out- come remains inferior in some cancers occurring in chil- dren and AYA in both Europe and the US (Table 2) [9,25,56,57].
Keegan at al. reported data form SEER in the period 2002-2006, 5-years RS of melanoma, non-Hodgkin lym- phoma, thyroid cancer, testicular cancer and breast can- cer were over 80%. Thyroid cancer was having the best survival outcome among all cancer types in AYA (5-year RS of 99.7%), followed by testicular cancer (96.1%) and melanoma (95.5%) [56]. On the contrary, AYAs with acute myeloid leukemia, rhabdomyosarcoma, high grade as- trocytoma, carcinoma of lung, liver, pancreas and stom- ach had 5-year RS below 50%. AYAs with liver carcino- mas had the lowest 5-year RS of 25.2% [56].
In the presence of distant metastatic disease at the time of diagnosis, AYAs have better survival outcome compared with older adults. 5-years RS was 80.8%, 44%
and 17.9% for children age below 15, AYAs and older
adults (≥40 years), respectively [56].
Barriers to AYA Cancer Treatment
Across the world, there is significant variation of health care system, degree of socio-economic development, private and public insurance coverage, culture and even social norms which all could potentially influence treat- ment of AYA with cancer.
However, difficulty for AYA with cancer to access spe- cialized treatment center is not an uncommon problem across the world [4,8]. Centralized and multidisciplinary treatment centers with tailored therapy for AYA cancers are essential components for improving treatment out- come [9]. A report based on Los Angeles cancer registry studied the impact of treatment in designated Compre- hensive Cancer Center (CCC)/Children’s Oncology Group (COG) versus non-CCG/COG sites on survival outcomes of ALL and AML in AYA aged 15-39 years. Proportion of patients being treated at CCC/COG site decreased with age, 50.5% of those age 15-21 received treatment in CCC/COG sites whereas it dropped to 12.3% among age 22-39. Patients treated in non CCG/COG centers had in- ferior outcome and lack of private insurance and African American/Hispanic race/ethnicity were barriers against seeking treatment in specialized centers [2].
SES and financial issues also affect AYA in accessing specialized centers for treatment and completing therapy.
In the US, studies have examined the relationship be- tween SES and insurance coverage. It is estimated that 9% of people in the US did not have insurance coverage [58]. AYA aged 18-24 was the least insured age group with more than 30% not having health insurance [12].
Study in adults in the US revealed that patient having Medicaid coverage/no insurance were more likely to present with metastatic disease, less likely to receive sur- gery/radiotherapy and having a higher chance of death compared to those with non-Medicaid insurance [59].
AYA with cancer is no exception and insurance status is an independent factor associated with distant meta- stasis at the time of diagnosis [60]. A study in California shown that, during 1991 to 2014, among AYA with pub- lic/no insurance, the chance of having treatment in spe-
cialized centers was lower than those with private in- surance [61]. Two studies in the US looked into the issue of insurance disparities in 40,000 young adults in the time period 2007-2009 and 66,556 AYA from 2007 through 2014. Among those with public or no insurance, there were higher chance of metastatic disease at the time of presentation, lower proportion received definitive treat- ment and having poorer survival outcome [22,62].
An analysis of a cohort of AYA patients in the Health Outcome and Patient Experience (HOPE) study found in- surance coverage extending beyond AYA cancer diag- nosis decreases with time and was lower for the elder age and lower educational level group. A quarter of AYA pa- tients would have certain time period without insurance coverage in the 3 years after cancer diagnosis [63]. Al- though the importance of insurance coverage in seeking medical treatment is not the same across different health care systems, it reflects the potential obstacles for AYA patients in seeking appropriate medical treatments.
Under-representation in clinical trials due to lack of tailored trials for AYA and lack of access to centers par- ticipating in AYA clinical trials were postulated to be the cause of lack of improvement in AYA cancer. In the US and Europe, majority of children with cancer age less than 15 are enrolled in clinical trials; whereas the pro- portion decrease to 10% for those aged 15-19 in the US with a further drop to 1 to 2% for young adults [12].
In 2016, the European Society for Medical Oncology (ESMO)/the European Society for Pediatric Oncology (SIOPE) conducted an online survey on HCP with interest in AYA cancer. Two-third of respondents reported that their patients were not able to access specialized services and the problem was more severe in Eastern and South- Eastern Europe. It was alarming that more than two-third said they were not aware of any research activities on AYA cancer [4].
A similar survey was carried out by the ESMO/SIOPE
and the Asian continental branch of International Society
of Pediatric Oncology in Asia in 2018. It also identified
similar difficulty in accessing specialized AYA cancer
services and lack of awareness of research activities
among HCP. This survey had additional questions look-
ing into funding of cancer treatment and issue of non- compliance and non-adherence to treatment. In about two-third of the respondents, they acknowledged funding source being government-based social insurance and pa- tient self-financed, at least partially. About half of their patients had private insurance while a quarter of them experienced difficulties in terms of insurance. Seventy percent of respondents reckoned financial and insurance issues being the reasons behind abandoning and non-ad- herence to treatment, which is worrying; while one-out- of-four respondents replied that religious belief would play a role in non-adherence and an equal proportion of respondents regarded gender inequality a problem af- fecting decision on treatment [8].
Training and education of HCP is also an important is- sue that should not be over-emphasized. However, sur- veys in Europe and Asia both revealed that only a minor- ity of HCP were able to access education and training re- lated to AYA cancers [4,8]. This is sub-optimal and ef- forts should be made to improve the situation.
Long Term Outcome,
Survivorship Health and Late Sequelae
Majority of AYA with cancer would be cured and given the relatively young age at diagnosis, there are decades of life ahead for these survivors. Taking good care of the long-term health issues of these survivors should not be neglected.
There is a long-term increase risk of death in survivors of AYA with cancers. In 2020, a report on the long-term outcome of AYA cancer survivors registered in the Uni- versity of Texas MD Anderson Cancer Tumor Registry was published. The cohort was comprised of 16,728 AYA cancer survivors and OS was estimated to be 86%, 74%
and 68% at 10-year, 20-year and 25-year after initial di- agnosis, respectively. The survival probability was lower than that of matched-cohort of general population at all time points [64].
Long term co-mobilities including cardiovascular and respiratory diseases and second malignant neoplasm (SMN) are potential threats to cancer survivors. A study
investigated the risk of SMN among 2-year survivors of AYA cancer in Southern California from 1990 to 2012.
The risk of SMN is estimated to be 12.5% at 20 years after initial diagnosis and resulted in 7-fold increase in mor- tality compared with survivors without SMN [65]. In an- other large cohort of 200,945 AYA cancer survivors in the Teenage and Young Adult Cancer Survivor Study (TYACSS) in England and Wales, there were 12,321 SMN at a median follow up of 16.8 years. AYA with history of breast cancer, cervical cancer, testicular cancer or Hodgkin lymphoma were particularly at risk of SMN [66].
In regard to cardiovascular and respiratory co-mor- bidities, AYA cancer survivors are also at increased risk when compared with general population. The Kaiser Permanente Cancer Survivor Study shown that, among 5,671 AYA cancer survivors, the risk of having car- diovascular diseases (CVD) including heart failure, coro- nary artery disease and stroke is at least 2 times higher than that of matched subjects without cancer. Chance of dying from the CVD is also significantly elevated, esti- mated at 11 times higher, when compared with general population [67]. In the TYACSS, there were 1,079 respi- ratory deaths in the cohort of 200,945 AYA cancer survi- vors with a mean follow up of 19.3 years. It was observed that the risk of dying from respiratory diseases was 70%
higher when compared with general population, with standardized mortality ratio highest for pneumonitis and pneumonia. Cancer survivors of lung cancer, leukemia, head and neck cancer and central nervous system tumor carried the greatest excess risk of death [68].
In summary, AYA with cancer is distinct from younger
children and older adults in terms of spectrum of disease,
biology and treatment outcome even for the same cancer
and the incidence is rising. Despite favorable survival
outcome is observed for the whole AYA group, survival
in AYA is still inferior for many cancer types common to
both children and AYA. Treatment in centralized centers
and promotion of accrual to clinical trials should be
strongly advocated. Risk of long-term co-morbidities,
risk of SMN and mortality should be properly addressed.
Conflict of Interest Statement
The authors have no conflict of interest to declare.
References
1. Adolescents and Young Adults Oncology Review Group.
Closing the gap: research and care imperatives for adoles- cents and young adults with cancer. Bethesda: NIH pub- lication, 2006.
2. Wolfson J, Sun CL, Wyatt L, Stock W, Bhatia S. Adolescents and young adults with acute lymphoblastic leukemia and acute myeloid leukemia: impact of care at specialized cancer centers on survival outcome. Cancer Epidemiol Biomarkers Prev 2017;26:312-20.
3. Fidler MM, Gupta S, Soerjomataram I, Ferlay J, Steliarova- Foucher E, Bray F. Cancer incidence and mortality among young adults aged 20-39 years worldwide in 2012: a pop- ulation-based study. Lancet Oncol 2017;18:1579-89.
4. Li CK, Dalvi R, Yonemori K, et al. Care of adolescents and young adults with cancer in Asia: results of an ESMO/SIOPE/
SIOP Asia survey. ESMO Open 2019;4:e000467.
5. Barr RD, Ferrari A, Ries L, Whelan J, Bleyer WA. Cancer in adolescents and young adults: a narrative review of the cur- rent status and a view of the future. JAMA Pediatr 2016;170:
495-501.
6. Desandes E, Stark DP. Epidemiology of adolescents and young adults with cancer in europe. Prog Tumor Res 2016;43:1-15.
7. Roder DM, Warr A, Patterson P, Allison KR. Australian ado- lescents and young adults-trends in cancer incidence, mor- tality, and survival over three decades. J Adolesc Young Adult Oncol 2018;7:326-38.
8. Li CK, Dalvi R, Yonemori K, et al. Care of adolescents and young adults with cancer in Asia: results of an ESMO/SIOPE/
SIOP Asia survey. ESMO Open 2019;4:e000467.
9. Trama A, Botta L, Steliarova-Foucher E. Cancer burden in adolescents and young adults: a review of epidemiological evidence. Cancer J 2018;24:256-66.
10. Moon EK, Park HJ, Oh CM, et al. Cancer incidence and sur- vival among adolescents and young adults in Korea. PLoS One 2014;9:e96088.
11. Ohara A, Furui T, Shimizu C, et al. Current situation of can- cer among adolescents and young adults in Japan. Int J Clin Oncol 2018;23:1201-11.
12. Burke ME, Albritton K, Marina N. Challenges in the recruit- ment of adolescents and young adults to cancer clinical trials.
Cancer 2007;110:2385-93.
13. Close AG, Dreyzin A, Miller KD, Seynnaeve BKN, Rapkin LB.
Adolescent and young adult oncology-past, present, and future.
CA Cancer J Clin 2019;69:485-96.
14. Gupta S, Harper A, Ruan Y, et al. International trends in the incidence of cancer among adolescents and young adults. J Natl Cancer Inst 2020;112:1105-17.
15. Nomellini PF, Curado MP, Oliveira MM. Cancer incidence in adolescents and young adults in 24 selected populations of Latin America. J Adolesc Young Adult Oncol 2018;7:164-73.
16. Bleyer A, Ferrari A, Whelan J, Barr RD. Global assessment of cancer incidence and survival in adolescents and young adults. Pediatr Blood Cancer 2017;64.
17. Ahn HS, Kim HJ, Welch HG. Korea’s thyroid-cancer “epi- demic”--screening and overdiagnosis. N Engl J Med 2014;
371:1765-7.
18. Katanoda K, Shibata A, Matsuda T, et al. Childhood, adoles- cent and young adult cancer incidence in Japan in 2009- 2011. Jpn J Clin Oncol 2017;47:762-71.
19. Desandes E, Lacour B, Belot A, et al. Cancer incidence and survival in adolescents and young adults in France, 2000-2008.
Pediatr Hematol Oncol 2013;30:291-306.
20. Bleyer A, Barr R, Hayes-Lattin B, et al. The distinctive biology of cancer in adolescents and young adults. Nat Rev Cancer 2008;8:288-98.
21. Rytting ME, Jabbour EJ, O’Brien SM, Kantarjian HM. Acute lymphoblastic leukemia in adolescents and young adults.
Cancer 2017;123:2398-403.
22. Colton MD, Goulding D, Beltrami A, et al. A U.S. population- based study of insurance disparities in cancer survival among adolescents and young adults. Cancer Med 2019;8:4867-74.
23. Barr RD, Holowaty EJ, Birch JM. Classification schemes for tumors diagnosed in adolescents and young adults. Cancer 2006;106:1425-30.
24. Birch JM, Alston RD, Kelsey AM, Quinn MJ, Babb P, McNally RJ. Classification and incidence of cancers in adolescents and young adults in England 1979-1997. Br J Cancer 2002;
87:1267-74.
25. Trama A, Bernasconi A, McCabe MG, et al. Is the cancer sur- vival improvement in European and American adolescent and young adults still lagging behind that in children? Pediatr Blood Cancer 2019;66:e27407.
26. Ramanujachar R, Richards S, Hann I, et al. Adolescents with acute lymphoblastic leukaemia: outcome on UK national paediatric (ALL97) and adult (UKALLXII/E2993) trials. Pediatr Blood Cancer 2007;48:254-61.
27. Ram R, Wolach O, Vidal L, Gafter-Gvili A, Shpilberg O, Raanani P. Adolescents and young adults with acute lymphoblastic leukemia have a better outcome when treated with pedia- tric-inspired regimens: systematic review and meta-analysis.
Am J Hematol 2012;87:472-8.
28. Pole JD, Alibhai SM, Ethier MC, et al. Adolescents with acute lymphoblastic leukemia treated at pediatric versus adult hospitals. Ann Oncol 2013;24:801-6.
29. Stock W, La M, Sanford B, et al. What determines the out- comes for adolescents and young adults with acute lympho- blastic leukemia treated on cooperative group protocols? A comparison of Children’s Cancer Group and Cancer and Leukemia Group B studies. Blood 2008;112:1646-54.
30. Hayakawa F, Sakara T, Yujiri T, et al. Markedly improved outcomes and acceptable toxicity in adolescents and young adults with acute lymphoblastic leukemia following treatment with a pediatric protocol: a phase II study by the Japan Adult Leukemia Study Group. Blood Cancer J 2014;4:e252.
31. Alvarnas JC, Brown PA, Aoun P, et al. Acute lymphoblastic leukemia, version 2.2015. J Natl Compr Canc Netw 2015;13:
1240-79.
32. Stock W, Luger SM, Advani AS, et al. A pediatric regimen for older adolescents and young adults with acute lymphoblastic leukemia: results of CALGB 10403. Blood 2019;133:1548-59.
33. Papworth KE, Arroyo VM, Styring E, Zaikova O, Melin BS, Lupo PJ. Soft-tissue sarcoma in adolescents and young adults compared with older adults: a report among 5000 patients from the Scandinavian Sarcoma Group Central Register. Cancer 2019;125:3595-602.
34. Herzog CE. Overview of sarcomas in the adolescent and young adult population. J Pediatr Hematol Oncol 2005;27:215- 8.
35. Kasper B, Ouali M, van Glabbeke M, et al. Prognostic factors in adolescents and young adults (AYA) with high risk soft tis- sue sarcoma (STS) treated by adjuvant chemotherapy: a study based on pooled European Organisation for Research and Treatment of Cancer (EORTC) clinical trials 62771 and 62931.
Eur J Cancer 2013;49:449-56.
36. Blay JY, Soibinet P, Penel N, et al. Improved survival using specialized multidisciplinary board in sarcoma patients. Ann Oncol 2017;28:2852-9.
37. Loong HH, Blay JY, Munhoz RR. International collaborations and regional challenges in providing specialist multidiscipli- nary sarcoma care. Am Soc Clin Oncol Educ Book 2019:616- 23.
38. Johnson RH, Anders CK, Litton JK, Ruddy KJ, Bleyer A. Breast cancer in adolescents and young adults. Pediatr Blood Cancer 2018;65:e27397.
39. Gondos A, Hiripi E, Holleczek B, et al. Survival among ado- lescents and young adults with cancer in Germany and the United States: an international comparison. Int J Cancer 2013;133:2207-15.
40. O’Connell JB, Maggard MA, Liu JH, Etzioni DA, Livingston EH, Ko CY. Rates of colon and rectal cancers are increasing in young adults. Am Surg 2003;69:866-72.
41. Troeung L, Sodhi-Berry N, Martini A, et al. Increasing in- cidence of colorectal cancer in adolescents and young adults aged 15-39 years in Western Australia 1982-2007: examina- tion of colonoscopy history. Front Public Health 2017;5:179.
42. Quah HM, Joseph R, Schrag D, et al. Young age influences treatment but not outcome of colon cancer. Ann Surg Oncol 2007;14:2759-65.
43. Levine O, Zbuk K. Colorectal cancer in adolescents and young adults: defining a growing threat. Pediatr Blood Cancer 2019;66:e27941.
44. Nakayama Y, Kobayashi H, Kawamura H, et al. The long- term outcomes in adolescent and young adult patients with colorectal cancer -a multicenter large-scale cohort study. J Cancer 2020;11:3180-5.
45. Kusler KA, Poynter JN. International testicular cancer in- cidence rates in children, adolescents and young adults.
Cancer Epidemiol 2018;56:106-11.
46. Stoneham S, Murray M, Thomas B, Williamson M, Sweeney C, Frazier L. AYA testis cancer: the unmet challenge. Pediatr Blood Cancer 2019;66:e27796.
47. Amini A, Waxweiler TV, Maroni PD, et al. Survival outcomes of adolescent and adult patients with non-seminomatous tes- ticular germ-cell tumors: a population-based study. J Pediatr Urol 2016;12:405.e1-e9.
48. Musa J, Achenbach CJ, O’Dwyer LC, et al. Effect of cervical cancer education and provider recommendation for screen- ing on screening rates: a systematic review and meta-analysis.
PLoS One 2017;12:e0183924.
49. Olusola P, Banerjee HN, Philley JV, Dasgupta S. Human pap- illoma virus-associated cervical cancer and health disparities.
Cells 2019;8:622.
50. Sawaya GF, Smith-McCune K, Kuppermann M. Cervical can- cer screening: more choices in 2019. JAMA 2019;321:2018-9.
51. Lin YJ, Fan LW, Tu YC. Perceived risk of human papil- lomavirus infection and cervical cancer among adolescent women in Taiwan. Asian Nurs Res (Korean Soc Nurs Sci) 2016;10:45-50.
52. Vriens MR, Moses W, Weng J, et al. Clinical and molecular features of papillary thyroid cancer in adolescents and young adults. Cancer 2011;117:259-67.
53. Keegan THM, Grogan RH, Parsons HM, et al. Sociodemographic disparities in differentiated thyroid cancer survival among adolescents and young adults in California. Thyroid 2015;
25:635-48.
54. Bleyer A, O’Leary M, Barr R, Ries LAG. Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975-2000. Bethesda, MD: National Cancer Institute, 2006. (Accessed September 13, 2020, at https://seer.cancer.gov/archive/publications/aya/) 55. Liu L, Moke DJ, Tsai KY, et al. A reappraisal of sex-specific
cancer survival trends among adolescents and young adults in the United States. J Natl Cancer Inst 2019;111:509-18.
56. Keegan THM, Ries LAG, Barr RD, et al. Comparison of cancer survival trends in the United States of adolescents and young adults with those in children and older adults. Cancer 2016;122:1009-16.
57. Trama A, Botta L, Foschi R, et al. Survival of European ado- lescents and young adults diagnosed with cancer in 2000-07:
population-based data from EUROCARE-5. Lancet Oncol 2016;
17:896-906.
58. Kehl KL, Keating NL, Giordano SH, Schrag D. Insurance net- works and access to affordable cancer care. J Clin Oncol 2020;38:310-5.
59. Walker GV, Grant SR, Guadagnolo BA, et al. Disparities in stage at diagnosis, treatment, and survival in nonelderly adult patients with cancer according to insurance status. J Clin Oncol 2014;32:3118-25.
60. Robbins AS, Lerro CC, Barr RD. Insurance status and dis- tant-stage disease at diagnosis among adolescent and young adult patients with cancer aged 15 to 39 years: National Cancer Data Base, 2004 through 2010. Cancer 2014;120:
1212-9.
61. Alvarez E, Keegan T, Johnston EE, et al. Adolescent and young adult oncology patients: disparities in access to speci- alized cancer centers. Cancer 2017;123:2516-23.
62. Aizer AA, Falit B, Mendu ML, et al. Cancer-specific outcomes among young adults without health insurance. J Clin Oncol
2014;32:2025-30.
63. Parsons HM, Schmidt S, Harlan LC, et al. Young and un- insured: insurance patterns of recently diagnosed adolescent and young adult cancer survivors in the AYA HOPE study.
Cancer 2014;120:2352-60.
64. Berkman AM, Livingston JA, Merriman K, et al. Long-term survival among 5-year survivors of adolescent and young adult cancer. Cancer 2020;126:3708-18.
65. Chao C, Bhatia S, Xu L, et al. Incidence, risk factors, and mortality associated with second malignant neoplasms among survivors of adolescent and young adult cancer. JAMA Netw Open 2019;2:e195536.
66. Bright CJ, Reulen RC, Winter DL, et al. Risk of subsequent primary neoplasms in survivors of adolescent and young
adult cancer (Teenage and Young Adult Cancer Survivor Study): a population-based, cohort study. Lancet Oncol 2019;
20:531-45.
67. Chao C, Xu L, Bhatia S, et al. Cardiovascular disease risk profiles in survivors of adolescent and young adult (AYA) cancer: the Kaiser Permanente AYA Cancer Survivors Study.
J Clin Oncol 2016;34:1626-33.
68. Fidler MM, Reulen RC, Bright CJ, et al. Respiratory mortality of childhood, adolescent and young adult cancer survivors.
Thorax 2018;73:959-68.
69. Aben KK, van Gaal C, van Gils NA, van der Graaf WT, Zielhuis GA. Cancer in adolescents and young adults (15-29 years): a population-based study in the Netherlands 1989- 2009. Acta Oncol 2012;51:922-33.