저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Multidrug-Resistant Hepatitis B Virus
Resulting From Sequential Monotherapy With
Lamivudine, Adefovir, and Entecavir: Clonal
Evolution During Lamivudine Plus Adefovir
Therapy
by
Soon Sun Kim
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
Multidrug-Resistant Hepatitis B Virus
Resulting From Sequential Monotherapy With
Lamivudine, Adefovir, and Entecavir: Clonal
Evolution During Lamivudine Plus Adefovir
Therapy
by
Soon Sun Kim
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements
for the Degree of
Ph.D. in Medicine
Supervised by
Sung Won Cho, M.D., Ph.D.
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
This certifies that the dissertation
of Soon Sun Kim is approved.
SUPERVISORY COMMITTEE
Sung Won Cho
Jin Hong Kim
Young Sok Lee
Byung Moo Yoo
Jae Youn Cheong
The Graduate School, Ajou University
May, 20th, 2013
ACKNOWLEDGEMENTS
“The biospecimens for this study were provided by the Ajou Human Bio-Resource Bank (AHBB), a member of the National Biobank of Korea, which is supported by the Ministry of Health and Welfare. All samples derived from the National Biobank of Korea were obtained with informed consent under institutional review board-approved protocols”
i
- ABSTRACT -
Multidrug-Resistant Hepatitis B Virus Resulting From Sequential
Monotherapy With Lamivudine, Adefovir, and Entecavir: Clonal
Evolution During Lamivudine Plus Adefovir Therapy
Background & Aims: Whether multidrug-resistant (MDR) hepatitis B virus (HBV) harbors
mutations co-located in the same HBV clones that confer reduced sensitivity to antiviral therapy remains uncertain. This study investigated the evolution of MDR HBV strains developed from sequential monotherapy with lamivudine (LAM), adefovir (ADV), and entecavir (ETV) during LAM plus ADV salvage therapy.
Methods: Sera were obtained from 6 patients who had developed sequential resistance to
LAM, ADV, and ETV before and during LAM plus ADV therapy. The HBV genomes from each patient were amplified, cloned, and sequenced.
Results: Among 6 sets of 20 clones obtained before salvage therapy, all clones harbored the
rtM204V mutation, and ETV-resistant mutations were detected with the rtM204V in 108 clones. The rtA181 mutation was not detected at baseline, but emerged in 5 patients during therapy. Among 9 sets of 20 clones obtained during salvage therapy, 39 clones harbored rtA181T/V ± rtN236T mutations, which were detected in the absence of rtM204 and ETV-resistant mutations in 37 clones (94.9%). Only 2 clones (5.1%) harbored both rtA181T/V and resistant mutations. The rtA181T/V mutation emerged after reversion from
ETV-ii
resistant mutants to wild-type HBV. Five patients achieved a partial virologic response to LAM plus ADV therapy.
Conclusions: The majority of MDR mutations existed in different genomes. Suboptimal
response to LAM plus ADV therapy may not result from the co-localization of MDR HBV mutations in the same genome, but instead the low antiviral potency of these drugs. Thus, more potent antiviral drug combinations may be an effective salvage therapy for MDR patients.
Keywords : Chronic hepatitis B, Clonal sequencing, HBV DNA, Multidrug resistance, Viral genome
iii
TABLE OF CONTENTS
ABSTRACT ··· ⅰ TABLE OF CONTENTS ··· ⅲ LIST OF FIGURES ··· ⅳ LIST OF TABLES ··· ⅴ . Ⅰ INTRODUCTION ··· 1 . Ⅱ PATIENTS AND METHODS ··· 3A. PATIENTS ··· 3
B. METHODS ··· 4
1. HBV DNA quantitation ··· 4
2. RFMP Assay ··· 4
3. Clonal sequencing analysis ··· 5
2. Statistical Analysis ··· 6 . Ⅲ RESULTS ··· 7 . Ⅳ DISCUSSION ··· 22 . Ⅴ CONCLUSION ··· 28 REFERENCES ··· 29 국문요약 ··· 33
iv
LIST OF FIGURES
Fig. 1. Flow diagram of the treatment and sera sampling protocol used for the study patients ··· 4
Fig. 2. Clinical course and evolution of antiviral-resistant mutations during lamivudine (LAM) plus adefovir (ADV) therapy in 5 patients (patients 1−4, and 6) who developed sequential resistance to LAM, ADV, and entecavir (ETV) ··· 16
Fig. 3. Clinical course and evolution of antiviral-resistant mutations in patient 5, who developed virologic breakthrough during lamivudine (LAM) plus adefovir
v
LIST OF TABLES
Table 1. Resistance mutations of antiviral drugs used in this study··· 5
Table 2. Characteristics of patients ··· 8
Table 3. Clonal analysis of samples obtained before and during LAM plus ADV therapy in 6 multi-drug resistant patients ··· 10
Table 4. Evolution of multi-drug resistant mutations during LAM plus ADV therapy in 6 Patients: analysis of 20 clones per each sample ··· 14
Table 5. Changes of hepatitis B surface antigen mutation during LAM plus ADV therapy in 6 patients with multi-drug resistance ··· 19
- 1 -
I. INTRODUCTION
Chronic hepatitis B virus (HBV) infection is an important cause of morbidity and mortality worldwide (Shepard et al., 2006). Several nucleoside/nucleotide analogues (NAs) have been developed over the past decade. The administration of NAs has been shown to suppress HBV replication and prevent progression to cirrhosis and hepatocellular carcinoma (Liver, 2009; Lok and McMahon, 2009). Five NAs (lamivudine [LAM], adefovir dipivoxil [ADV], entecavir [ETV], telbivudine, and clevudine) are currently approved in South Korea. The major drawback of long-term monotherapy with NAs is the emergence of drug resistance (Shaw et al., 2006; Zoulim and Locarnini, 2009). Furthermore, the emergence of resistance limits the efficacy of other NAs (European Association for the Study of the Liver [EASL], 2009; Lok and McMahon, 2009). Sequential monotherapy is known to increase the development of multidrug resistance (MDR). The sequential administration of ADV or ETV for LAM-resistant patients has been reported to result in dual resistance to LAM and ADV or LAM and ETV (Shaw et al., 2006; Zoulim and Locarnini, 2009). The development of a triple-drug-resistant (LAM, ADV, and ETV) HBV strain has been reported in LAM- and ADV-resistant patients after sequential ETV administration as salvage therapy (Liu et al., 2010).
MDR HBV mutations have known to co-localize to the same HBV clones that confer resistance to multiple antiviral agents with favorable cross-resistance profiles. HBV constructs with combinations of LAM and ADV mutations were reported to confer resistance to LAM and ADV combination therapy in vitro (Brunelle et al., 2005). Analysis
- 2 -
of clones from samples with MDR mutations have shown that MDR usually occurs by the sequential addition of resistance mutations in the same genome of HBV (Yim et al., 2006). However, these findings are limited and restricted to LAM and ADV double resistance. Recently, a case involving a patient with triple-drug-resistant HBV strains was reported. This case demonstrated that ETV- and ADV-resistant mutations co-localized to the same viral genome. While this MDR HBV strain could be suppressed by LAM and ADV combination therapy, the mechanism was not clarified (Liu et al., 2010).
Combination therapy with LAM and ADV was ineffective in suppressing HBV in patients who developed sequential resistance to LAM and ADV; however, approximately 20% of these patients had either a partial or complete virologic response to LAM plus ADV treatment (Heo et al., 2010). These findings suggest that LAM and ADV combination therapy is effective in suppressing resistant mutants in a small population of MDR patients. The mechanism by which MDR HBV strains in the same viral genome affect the antiviral effectiveness of therapy with NAs remains to be clarified. Furthermore, the evolution of MDR mutations should to be investigated in a large number of patients.
The present study evaluated whether MDR mutations were present in the same genome of HBV, and observed the evolution of the triple-drug-resistant mutations to LAM, ADV, and ETV during combination salvage therapy with LAM and ADV.
- 3 -
II. PATIENTS AND METHODS
A. PATIENTS
This study included 6 chronic hepatitis B patients with triple-drug resistance who were treated with LAM plus ADV combination therapy. All patients had a history of virological breakthrough induced by LAM resistance, and developed resistance to ADV after sequential ADV monotherapy. Virological breakthrough was defined as an increase in the level of HBV DNA of at least 1 log10 IU/mL from the lowest point during therapy with genotype analysis of the rtM204, rtA181, and rtN236 sequences. All cases of viral resistance were confirmed by the restriction fragment mass polymorphism (RFMP) assay. The patients received ETV monotherapy for the treatment of ADV resistance, and sequentially developed ETV resistance combined with virological breakthrough. After development of ETV resistance, all patients were switched to LAM and ADV combination therapy as a rescue therapy. Serial serum samples were obtained before (at the time of ETV resistance) and during LAM and ADV combination therapy for molecular analysis. Samples from these 6 patients were obtained just before combination therapy with LAM and ADV for baseline clonal analysis. Samples obtained after 12 months of LAM plus ADV therapy were cloned from each patient. Additional samples obtained from 3 patients during combination therapy were also cloned (Fig. 1). HBV DNA levels were tested at baseline and every 3 months thereafter during LAM and ADV combination therapy. A partial virologic response was defined as a decrease in HBV DNA of more than 1 log10 IU/mL but detectable HBV DNA,
- 4 -
according to the EASL guideline (EASL, 2009). This study was approved by the Institutional Review Board and all patients provided informed consent.
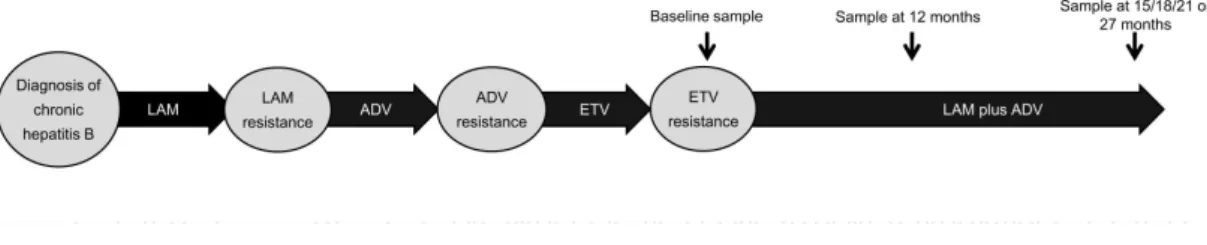
Fig. 1. Flow diagram of the treatment and sera sampling protocol used for the study patients. Baseline samples were obtained just prior to switching to lamivudine (LAM) plus
adefovir (ADV) combination therapy, and additional samples were obtained during therapy at 12 months, and 15, 18, 21 or 27 months on a case-by-case basis.
B. METHODS
1. HBV DNA Quantitation
HBV DNA levels were quantitated by real-time polymerase chain reaction (PCR) using the COBAS TaqManTM HBV test (Roche Diagnostics, Branchburg, NJ, USA), which had a lower detection limit of 20 IU/mL.
2. RFMP Assay
The RFMP assay was performed to detect LAM-resistant mutations (rt180, rt181, and rt204), ADV-resistant mutations (rt181 and rt236), and ETV-resistant mutations (rt169, rt184, rt202, and rt250 plus rt204) (Table 1) (Hong et al., 2004; Cho et al., 2010).
- 5 -
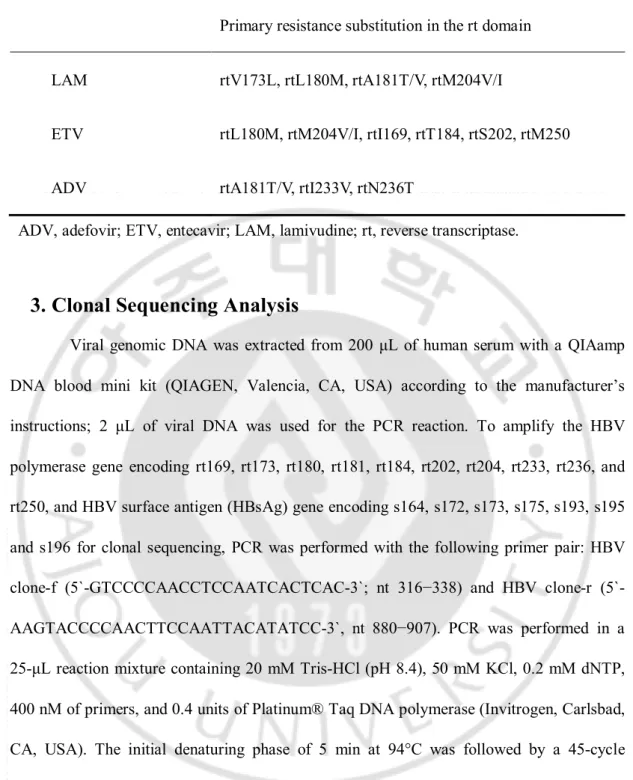
Table 1. Resistance mutations of antiviral drugs used in this study
ADV, adefovir; ETV, entecavir; LAM, lamivudine; rt, reverse transcriptase.
3. Clonal Sequencing Analysis
Viral genomic DNA was extracted from 200 μL of human serum with a QIAamp DNA blood mini kit (QIAGEN, Valencia, CA, USA) according to the manufacturer’s instructions; 2 μL of viral DNA was used for the PCR reaction. To amplify the HBV polymerase gene encoding rt169, rt173, rt180, rt181, rt184, rt202, rt204, rt233, rt236, and rt250, and HBV surface antigen (HBsAg) gene encoding s164, s172, s173, s175, s193, s195 and s196 for clonal sequencing, PCR was performed with the following primer pair: HBV clone-f GTCCCCAACCTCCAATCACTCAC-3`; nt 316−338) and HBV clone-r (5`-AAGTACCCCAACTTCCAATTACATATCC-3`, nt 880−907). PCR was performed in a 25-μL reaction mixture containing 20 mM Tris-HCl (pH 8.4), 50 mM KCl, 0.2 mM dNTP, 400 nM of primers, and 0.4 units of Platinum® Taq DNA polymerase (Invitrogen, Carlsbad, CA, USA). The initial denaturing phase of 5 min at 94°C was followed by a 45-cycle amplification phase containing a denaturation step at 94°C for 15 sec, an annealing step at 55°C for 15 sec, and an elongation step at 72°C for 15 sec, followed by termination of incubation at 72°C for 5 min. The PCR products were cloned into the pGEM® T-Easy
Primary resistance substitution in the rt domain LAM rtV173L, rtL180M, rtA181T/V, rtM204V/I
ETV rtL180M, rtM204V/I, rtI169, rtT184, rtS202, rtM250 ADV rtA181T/V, rtI233V, rtN236T
- 6 -
vector (Promega, Madison, WI, USA), and subsequently sequenced with vector-specific primers. Approximately 20 clones per serum sample were randomly selected for clonal sequencing analysis. Cloned DNAs were sequenced with the BigDye Terminator v3.1 Cycle Sequencing kit and ABI PRISM 3100 Genetic Analyzer (Applied Biosystems, Foster City, CA, USA).
4. Statistical Analysis
Statistical testing was performed using SPSS (version 13.0; SPSS, Inc., Chicago, IL, USA). Results are reported as the mean ± standard deviation (SD). The HBV DNA levels were transformed logarithmically for analyses.
- 7 -
III. RESULTS
A. Baseline Characteristics
Six ETV-resistant chronic hepatitis B patients with prior double resistance to LAM and ADV were included in the analysis. Mutation patterns for LAM and ADV are described in Table II. All 6 patients were men, with a mean age of 47.8 ± 4.07 years. The mean HBV DNA level was 6.13 ± 1.23 log10 IU/mL, and the mean alanine aminotransferase (ALT) level was 56.5 ± 39.6 U/L. Five patients were Hepatitis B e antigen-positive. At the initiation of LAM plus ADV therapy, all 6 patients had ETV-resistant mutants (rtT184L, n = 4; rtS202G, n = 1; rtT184L + rtS02G, n = 1) coupled with rtM204V + rtL180M mutants. ADV-resistant mutants were not detected at the time of initiation of LAM plus ADV combination therapy. All patients were infected with HBV genotype C (Table 2).
- 8 - Table 2. Characteristics of patients
ADV, adefovir; ALT, alanine aminotransferase; ETV, entecavir; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; LAM, lamivudine; rt, reverse transcriptase domain of polymerase. aAssessed by restriction fragment mass polymorphism
Patients 1 2 3 4 5 6
Age, year/ Gender 42/M 53/M 47/M 46/M 52/M 47/M
First antiviral therapy LAM LAM LAM LAM LAM LAM
Duration, months 24 26 35 20 52 60
Mutation pattern rtM204V/I+rtL180M rtM204V+L180M rtM204V/I+L180M rtM204V+rtL180M rtM204V+L180M rtM204V/I+rtL180M
Second antiviral therapy ADV ADV ADV ADV ADV ADV
Duration, months 24 20 21 27 23 12
Mutation patterna rtA181V rtA181V rtA181V rtA181V rtA181V rtM204I+rtL180M+rtA181V
Third antiviral therapy ETV ETV ETV ETV ETV ETV
Duration, months 12 24 18 30 18 27 Mutation patterna rtM204V+rtL180M +rtS202G rtM204V+rtL180M +rtT184L rtM204V+rtL180M +rtT184L rtM204V+rtL180M +rtT184L+rtS202G rtM204V+rtL180M +rtT184L rtM204V+rtL180M +rtT184L Rescue therapy for ETV
resistance
LAM+ADV LAM+ADV LAM+ADV LAM+ADV LAM+ADV LAM+ADV
Duration, months 15 21 15 18 27 15
HBV DNA, log10 IU/mL 5.30 4.31 6.95 5.63 7.30 7.28
ALT, U/L 69 24 52 42 129 23
- 9 -
B. Clonal analysis
The results of the clonal analysis are summarized in Table 3. Six sets of 20 clones from the baseline samples were analyzed to determine the localization of the LAM- and ETV-resistant mutations. All 120 clones contained YMDD mutations (rtM204V + rtL180M, n = 118; rtM204V + rtL180M + rtV173L, n = 1; rtM204V, n = 1), and 108 clones had resistant mutations (rtS202G, n = 31; rtT184L, n = 77). Among the 108 clones with ETV-resistant mutations, 107 had rtM204V + rtL180M mutations, and 1 had the rtM204V mutation. No clone had either the rtA181 or rtN236 mutant at baseline. One hundred eighty clones from samples obtained during LAM and ADV combination therapy were also analyzed to determine the localization of ETV- and ADV (or LAM)-resistant mutations. Among 9 sets of 20 clones from samples obtained during LAM plus ADV therapy, 39 clones had rtA181T/V ± rtN236T mutations (rtA181V, n = 32; rtA181T, n = 5; rtA181V + rtN236T, n = 1; and rtA181T + rtN236T, n = 1). The rtA181T/V or rtN236T mutations were detected in the absence of rtM204 and ETV-resistant mutations in 37 of 39 clones (94.9%). The rtA181 or rtN236 mutations were detected with LAM- and ETV-resistant mutations in the other 2 clones (5.1%). Among 9 sets of 20 clones, 115 had ETV-resistant mutations (rtT184L, n = 104; and rtS202G, n = 11). Only 2 clones (1.7%) harbored both ETV-resistant and rtA181T mutations. These results suggested that the co-localization of MDR mutations in the same genome of HBV was rare in patients with prior resistance to LAM, ADV, and ETV during LMV and ADV combination therapy.
- 10 -
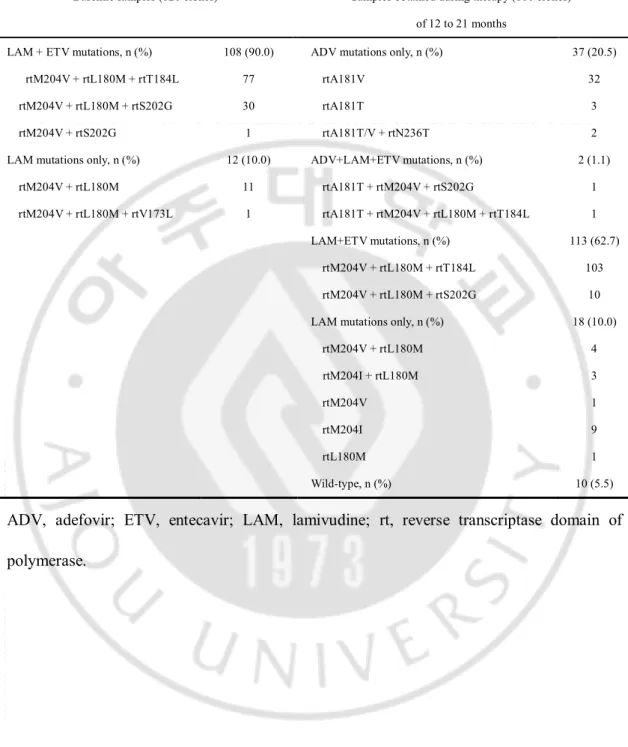
Table 3. Clonal analysis of samples obtained before and during LAM plus ADV therapy in 6 multi-drug resistant patients.
ADV, adefovir; ETV, entecavir; LAM, lamivudine; rt, reverse transcriptase domain of polymerase.
Baseline samples (120 clones) Samples obtained during therapy (180 clones)
of 12 to 21 months
LAM + ETV mutations, n (%) 108 (90.0) ADV mutations only, n (%) 37 (20.5)
rtM204V + rtL180M + rtT184L 77 rtA181V 32
rtM204V + rtL180M + rtS202G 30 rtA181T 3
rtM204V + rtS202G 1 rtA181T/V + rtN236T 2
LAM mutations only, n (%) 12 (10.0) ADV+LAM+ETV mutations, n (%) 2 (1.1)
rtM204V + rtL180M 11 rtA181T + rtM204V + rtS202G 1
rtM204V + rtL180M + rtV173L 1 rtA181T + rtM204V + rtL180M + rtT184L 1
LAM+ETV mutations, n (%) 113 (62.7)
rtM204V + rtL180M + rtT184L 103
rtM204V + rtL180M + rtS202G 10
LAM mutations only, n (%) 18 (10.0)
rtM204V + rtL180M 4 rtM204I + rtL180M 3 rtM204V 1 rtM204I 9 rtL180M 1 Wild-type, n (%) 10 (5.5)
- 11 -
C. Evolution of resistance to LAM, ADV, and ETV during HBV
therapy
The evolution of MDR mutations was observed before and after 12 months of combination therapy with LAM and ADV in 6 patients (Table 4 and Fig. 2). RFMP analysis of sera demonstrated the emergence of rtA181 or rtN236 mutations in 3 of 6 patients after 12 months of therapy; however, clonal analysis revealed the emergence of rtA181 or rtN236 mutations in 5 patients after 12 months of therapy. The number of clones harboring rtM204V and ETV-resistant mutations decreased from 120 (100%) and 108 (90%) clones at baseline to 83 (69.1%) and 79 (65.8%) clones after 12 months of therapy, respectively.
At the start of combination therapy for patient 1, among 20 clones studied, 19 had rtS202G with LAM-resistant mutations (rtM204V ± rtL180M). LAM-resistant mutations (rtM204V + rtL180M + rtV173L) were detected only in the remaining clone. After 12 months of therapy, an ETV-resistant mutation (rtS202G) remained in 1 clone with rtM204V. Among 20 clones, the rtA181 or rtN236 mutations were detected in all of the clones tested; 17 with rtA181V, 1 with rtA181T, 1 with rtA181V + rtN236T in the absence of other mutations, and 1 clone harboring rtA181T together with the rtS202G + rtM204V mutations (Fig. 2A).
At the beginning of therapy for patient 2, analysis of 20 clones demonstrated that 13 clones had rtT184L and LAM-resistant mutations (rtM204V + rtL180M), and 7 clones had LAM-resistant mutations alone (rtM204V + rtL180M). After 12 months of treatment, the rtM204V + rtL180M + rtT184L mutations remained detectable in 11 clones. The other 7 clones had only the rtA181V mutation. After 21 months of treatment, the rtM204V +
- 12 -
rtL180M + rtT184L mutations disappeared, while the rtM204I, wild-type, and rtA181V mutations were detected in 11, 7, and 2 clones, respectively (Fig. 2B).
Clonal analysis of baseline samples from patient 3 showed that 19 clones had rtT184L and LAM-resistant mutations (rtM204V + rtL180M) and the remaining clone had only LAM-resistant mutations. After 12 months of treatment, 17 clones had rtT184L + rtM204V + rtL180M mutations. One clone had rtA181T together with ETV-resistant mutations. In the other 2 clones, only the rtM204V + rtL180M mutations were detected (Fig. 2C).
In patient 4, 12 and 5 clones had rtS202G and rtT184L mutations with LAM-resistant mutations, respectively, in the baseline samples. Three clones had only the rtM204V + rtL180M mutations. After 12 months of therapy, the rtA181V mutation was detected in 3 of 20 clones in the absence of other mutations; ETV-resistant mutations were detected in 13 clones. Another 2 clones had wild-type HBV. After 18 months of treatment, the rtA181V and ETV-resistant mutations were detected in 3 and 17 of all clones, respectively (Fig. 2D).
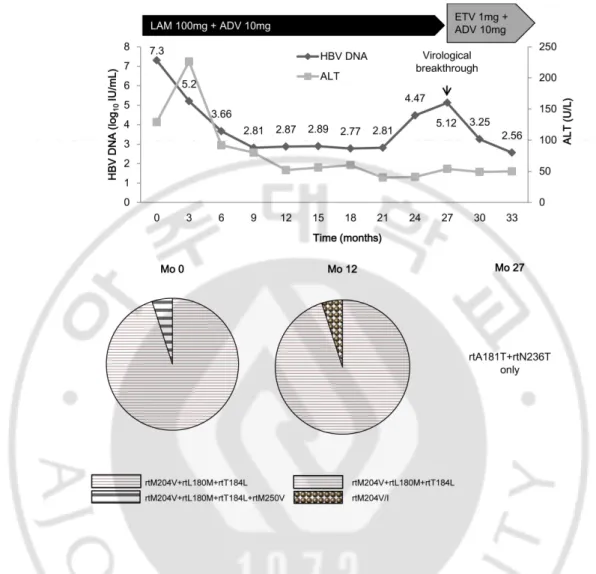
In patient 5, all 20 clones had ETV (rtT184L)- and LAM (rtM204V + rtL180M)- resistant mutations at baseline. After 12 months of treatment, 19 clones had rtT184L and rtM204V + rtL180M mutations, and 1 clone had the rtM204V mutation; rtA181 mutations were not detected. After 27 months of therapy, patient 5 developed virologic breakthrough. The genotype analysis of samples obtained at the time of virologic breakthrough showed emergence of rtA181T and rtN236T mutations in the absence of the rtL180M, rtM204V, and rtT184L mutations (Fig. 3).
- 13 -
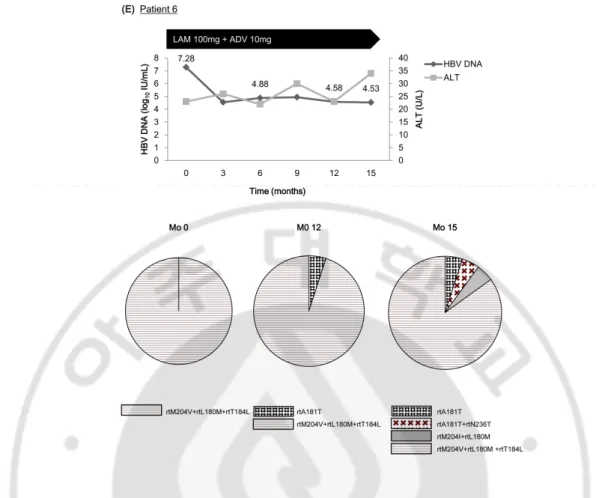
In patient 6, all 20 clones had rtT184L and rtM204V + rtL180M mutations at baseline. After 12 months of therapy, 1 clone had the rtA181T mutation without ETV-resistant mutations, and the other 19 clones had rtM204V + rtL180M + rtT184L mutations. After 15 months of treatment, the rtA181T mutation was detected in 1 clone, and rtA181T + rtN236T mutations were detected in another clone for the first time (Fig. 2E).
These results suggested that the replication of ETV-resistant mutants decreased during LAM plus ADV therapy, and rtA181 or rtN236 mutations emerged after reversion from ETV-resistant mutants to wild-type HBV.
D. Changes of HBsAg Mutation During the LAM and ADV
combination therapy
The antiviral drug resistance associated changes to the HBsAg were observed at each clone before and during the treatment (Table 5). The sW172* mutation was not detected at baseline samples obtained from 6 patients. However, the sW172* mutation was detected in 3 patients of 6 patients after 12 months of LAM plus ADV combination therapy. The sW172* mutation was detected in 2, 1, and 1 clone obtained from patient 1, 3, and 6, respectively.
- 14 -
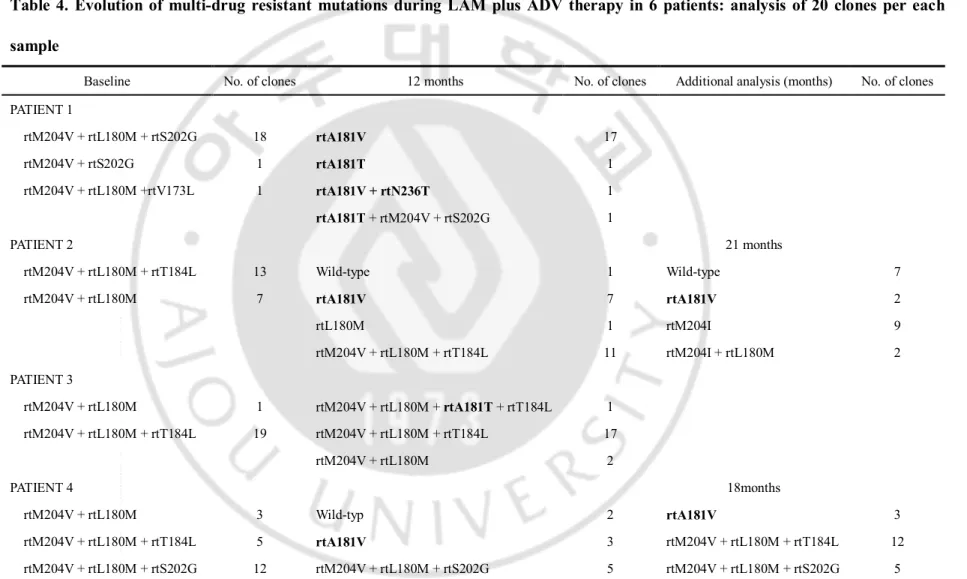
Table 4. Evolution of multi-drug resistant mutations during LAM plus ADV therapy in 6 patients: analysis of 20 clones per each sample
Baseline No. of clones 12 months No. of clones Additional analysis (months) No. of clones
PATIENT 1 rtM204V + rtL180M + rtS202G 18 rtA181V 17 rtM204V + rtS202G 1 rtA181T 1 rtM204V + rtL180M +rtV173L 1 rtA181V + rtN236T 1 rtA181T + rtM204V + rtS202G 1 PATIENT 2 21 months rtM204V + rtL180M + rtT184L 13 Wild-type 1 Wild-type 7 rtM204V + rtL180M 7 rtA181V 7 rtA181V 2 rtL180M 1 rtM204I 9 rtM204V + rtL180M + rtT184L 11 rtM204I + rtL180M 2 PATIENT 3 rtM204V + rtL180M 1 rtM204V + rtL180M + rtA181T + rtT184L 1 rtM204V + rtL180M + rtT184L 19 rtM204V + rtL180M + rtT184L 17 rtM204V + rtL180M 2 PATIENT 4 18months rtM204V + rtL180M 3 Wild-typ 2 rtA181V 3 rtM204V + rtL180M + rtT184L 5 rtA181V 3 rtM204V + rtL180M + rtT184L 12 rtM204V + rtL180M + rtS202G 12 rtM204V + rtL180M + rtS202G 5 rtM204V + rtL180M + rtS202G 5
- 15 -
NOTE. rtA181T/V and rtN236T are in bold
ADV, adefovir; LAM, lamivudine; rt, reverse transcriptase domain of polymerase.
rtM204V + rtL180M + rtT184L 8 rtM204V + rtL180M 2 PATIENT 5 rtM204V + rtL180M + rtT184L 19 rtM204V + rtL180M + rtT184L 19 rtM204V + rtL180M + rtT184L + rtM250V 1 rtM204V 1 PATIENT 6 15months rtM204V + rtL180M + rtT184L 20 rtA181T 1 rtA181T 1 rtM204V + rtL180M + rtT184L 19 rtA181T + rtN236T 1 rtM204V + rtL180M + rtT184L 17 rtM204I + rtL180M 1
- 18 -
Fig. 2. Clinical course and evolution of antiviral-resistant mutations during lamivudine (LAM) plus adefovir (ADV) therapy in 5 patients (patients 1−4, and 6) who developed sequential resistance to LAM, ADV, and entecavir (ETV). ETV-resistant mutations were
detected in the presence of LAM-resistant mutations (rtM204V + rtL180M) at the initiation of LAM plus ADV therapy, and the rtA181T/V mutations re-emerged within 12 months of therapy in all 5 patients.
- 19 -
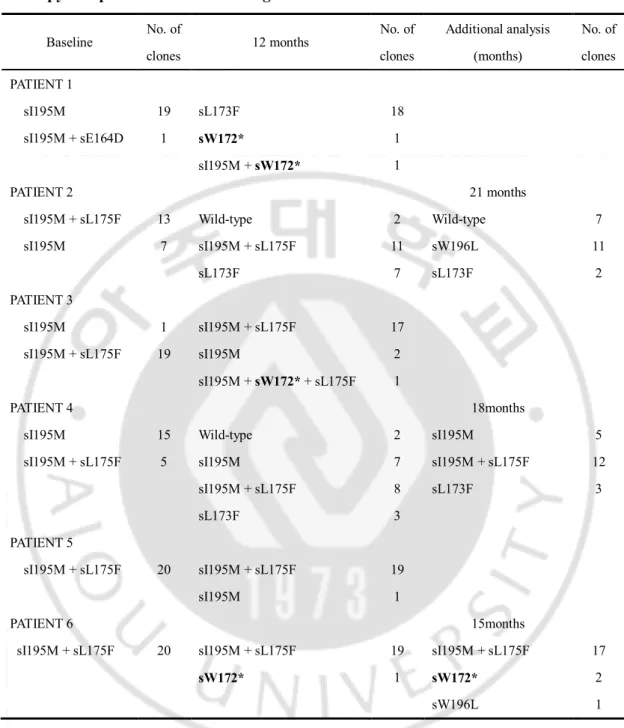
Table 5. Changes of hepatitis B surface antigen mutation during LAM plus ADV therapy in 6 patients with multi-drug resistance.
NOTE. Stop codon is in bold. ADV, adefovir; LAM, lamivudine.
Baseline No. of clones 12 months No. of clones Additional analysis (months) No. of clones PATIENT 1 sI195M 19 sL173F 18 sI195M + sE164D 1 sW172* 1 sI195M + sW172* 1 PATIENT 2 21 months
sI195M + sL175F 13 Wild-type 2 Wild-type 7
sI195M 7 sI195M + sL175F 11 sW196L 11 sL173F 7 sL173F 2 PATIENT 3 sI195M 1 sI195M + sL175F 17 sI195M + sL175F 19 sI195M 2 sI195M + sW172* + sL175F 1 PATIENT 4 18months
sI195M 15 Wild-type 2 sI195M 5
sI195M + sL175F 5 sI195M 7 sI195M + sL175F 12
sI195M + sL175F 8 sL173F 3 sL173F 3 PATIENT 5 sI195M + sL175F 20 sI195M + sL175F 19 sI195M 1 PATIENT 6 15months
sI195M + sL175F 20 sI195M + sL175F 19 sI195M + sL175F 17
sW172* 1 sW172* 2
- 20 -
E. Virologic response to LAM plus ADV therapy
The mean reduction in serum HBV DNA was -1.72 ± 1.18 log10 IU/mL and -1.89 ± 1.47 log10 IU/mL at 6 and 12 months of therapy, respectively. Among 6 patients, 5 had a partial virologic response at 6 months, with the exception of patient 1. None of the patients had undetectable HBV DNA levels by PCR throughout the follow-up period (Figs. 2 and 3). During a mean follow-up of 18.5 ± 4.8 months, 1 patient (patient 5) experienced virologic breakthrough after 27 months of therapy, after a partial virologic response. Serum HBV DNA was 7.3 log10 IU/mL at baseline, and decreased to 2.87 log10 IU/mL at 12 months of LAM plus ADV therapy without development of the rtA181 mutation. At 27 months of therapy, serum HBV DNA increased to 5.12 log10 IU/mL and was confirmed to possess rtA181T and rtN236T mutations. HBV DNA levels decreased to 2.56 log10 IU/mL after switching to ADV plus ETV therapy (Fig. 3).
- 21 -
Fig. 3. Clinical course and evolution of antiviral-resistant mutations in patient 5, who developed virologic breakthrough during lamivudine (LAM) plus adefovir (ADV) therapy. Patient 5 initially had a favorable response to LAM plus ADV therapy, but
developed virologic breakthrough after 27 months of therapy. After switching to ADV plus entecavir (ETV) therapy, the serum hepatitis B virus DNA level decreased.
- 22 -
IV. DISCUSSION
The emergence of MDR is increasing and has raised serious concerns regarding antiviral therapy. The emergence of resistance decreases susceptibility to antiviral agents and limits the selection of appropriate antiviral therapy. Dual resistance to LAM and ADV or ETV frequently develops in LAM-resistant patients treated with ADV or ETV therapy, respectively (Brunelle et al., 2005; Yim et al., 2006; Villet et al., 2007). Analysis of clones obtained from patients with dual resistance has revealed the presence of mutations conferring resistance to both drugs located in the same viral genome, resulting in resistance to both drugs (Yim et al., 2006).
In the current study, all 6 patients sequentially received LAM, ADV, and ETV, and subsequently developed resistance to each of these drugs. LAM plus ADV was administered as salvage therapy for the treatment of viral breakthrough induced by ETV resistance. The rtA181T/V mutants re-emerged in 5 of 6 patients after 12 months of therapy. Clonal analysis of serial samples was performed to determine whether the MDR mutations were present in the same genomes of HBV. Among 9 sets of 20 clones obtained from these 6 patients, 39 contained rtA181 ± rtN236 mutations. Among these 39 clones, the rtA181 ± rtN236 mutations emerged in the genome of wild-type HBV in 37 clones (94.9%). The co-localization of MDR mutations in the same genome occurred in only 2 clones. These findings suggested that additional mutations developed in the wild-type HBV genome in the process of reversion from an ETV-resistant mutant to wild-type HBV during therapy, and co-localization of MDR mutations rarely developed in the same genome. The results of the present study are in disagreement with previous reports (Yim et al., 2006; Liu et al., 2010).
- 23 -
In a previous study, clonal analysis was performed on 3 patients with double resistance to LAM and ADV. The rtQ215S, rtP237H, and rtN238T mutations were regarded as ADV-resistant mutations and these mutations were shown to co-localize to the same genome with the rtM204V/I mutation in all 3 patients (Yim et al., 2006). However, these mutations have not been demonstrated to be responsible for ADV resistance (Pallier et al., 2009). In that report, the primary ADV resistance mutations were found in 2 patients (rtN236T, n = 1; rtA181V, n = 1), and these mutations and the rtM204V/I mutation were located in different genomes of HBV. Recently, a patient with triple-drug-resistant HBV strains was reported (Liu et al., 2010). This study showed that ETV- and ADV-resistant mutations (rtA181V and rtN236T) transiently co-localized to the same viral genome during LAM and ADV combination therapy.
In a previous study, it was observed that ADV-resistant mutations emerge after reversion to YMDD wild-type HBV in LAM-resistant patients during sequential ADV monotherapy (Kwon et al., 2009). Another study demonstrated that ADV-resistant mutants replicate less efficiently than wild-type HBV, and mutants with the addition of rtM204V + rtL180M mutations to the rtN236T mutation exhibited the lowest level of replication relative to rtM204V + rtL180M mutants and rtN236T laboratory strains in vitro (Brunelle et al., 2005). A phenotypic analysis showed that the replication capacity of the rtL180M + rtA181V + rtN236T mutants and the rtL180M + rtA181V mutants were higher than that of the rtM204V + rtL180M + rtA181V and rtM204V + rtL180M + rtA181V + rtN236T mutants in Huh-7 cells in the presence of LAM plus ADV (Villet et al., 2009). These in vitro analyses suggested that the addition of the rtM204V mutation decreased the replication
- 24 -
capacity of ADV-resistant mutants. This likely explains why the HBV strains with MDR to LAM, ETV, and ADV existed as a minor population during therapy.
In the current study, the HBV strains harboring LAM (rtM204V + rtL180M)- and ETV-resistant mutations reverted to wild-type strains during LAM plus ADV therapy. However, the antiviral efficacy of combination therapy was limited in patients with MDR. The rtA181 mutants were shown to re-emerge in all patients after reversion to wild-type HBV from both LAM- and ETV-resistant mutants during LAM plus ADV therapy. In contrast, the development of ADV-resistant mutations was rare in LAM-resistant patients receiving ADV add-on therapy (Lampertico et al., 2007). LAM-resistant mutants have been shown to persist in the majority of patients after 1 year of ADV add-on therapy (Rapti et al., 2007). These findings suggest that wild-type HBV may be more vulnerable to the emergence of rtA181 mutations than strains harboring rtM204 and ETV-resistant mutations. This hypothesis may explain the frequent emergence of rtA181 mutations during LAM plus ADV therapy in this group of patients.
Among the 6 patients, 1 patient (patient 5) developed virological breakthrough during LAM plus ADV therapy. This patient did not develop the rtA181 mutation at 12 months of therapy and showed the most favorable virologic response until this time. However, after 27 months of combination therapy, the patient developed virological breakthrough with the emergence of the rtA181T + rtN236T mutations. These findings suggest that rtA181T + rtN236T mutations re-emerge and sufficiently proliferate to induce virological breakthrough after disappearance of the strains containing ETV-resistant mutations during LAM plus ADV therapy. The rtN236T mutation does not significantly
- 25 -
affect sensitivity to LAM, although the rtA181T mutation confers cross-resistance to LAM as well as ADV (Zoulim and Locarnini, 2012). Switching to ETV and ADV combination therapy was effective in the suppression of ADV-resistant mutants. A previous study with small number of patients showed that ETV plus ADV therapy was superior to LAM plus ADV therapy in ETV-refractory patients who experienced LAM or ADV treatment failure (Kim et al., 2012). Another study also reported that ETV plus ADV combination therapy showed a virologic response (serum HBV DNA concentration <60 IU/mL) in 29% of patients with LAM-resistant HBV who failed to respond to LAM plus ADV combination therapy at 52 weeks (Lim et al., 2012). Accordingly, ETV plus ADV can be an effective treatment option for MDR HBV.
Tenofovir disoproxil fumarate (TDF) has been recommended for treating patients with complex resistance (Liver, 2009; Lok and McMahon, 2009), as TDF was effective in patients with resistance to NAs (Tan et al., 2008; Berg et al., 2010; van Bommel et al., 2010; Patterson et al., 2011). A previous study reported that ADV-resistant mutations persist and are further selected after switching to TDF monotherapy in ADV-resistant patients (Tan et al., 2008), suggesting that combination therapy with NAs such as emtricitabine may be a more effective rescue therapy for patients with ADV resistance. However, another recent study showed that ADV-resistant mutants were selected during combination therapy with TDF and LAM in ADV-resistant patients (Patterson et al., 2011), as was observed with ADV and LAM combination therapy in the current study. These results suggest that adding emtricitabine or LAM on TDF may not be sufficient to delay the selection for ADV-resistant
- 26 -
mutations. The combination of TDF plus ETV may be a more effective rescue therapy for patients with HBV that is resistant to LAM, ADV, and ETV.
Interestingly, the rtA181T mutation encodes a stop codon in the overlapping surface gene at amino acid 172 (sW172*) and may affect HBV virion secretion. This may result in a progressive and slow increase of viral load (Warner and Locarnini, 2008; Zoulim and Locarnini, 2012). In the present study, rtA181T/sW172* mutation was detected in 3 patients after 12 months of LAM plus ADV combination therapy.
The present study demonstrated that susceptibility to antiviral agents and viral quasi-species evolution during therapy are important factors that determine the outcome of patients with ETV- and ADV-resistant HBV. Since MDR patients may not be rescued by the currently available drugs, including TDF, these patients should be monitored by HBV DNA quantitation and genotypic assays to identify antiviral susceptibility and virologic evolution to predict the development of additional resistant mutations (Zoulim and Locarnini, 2009).
In conclusion, the present clonal sequencing data revealed that the rtA181 mutation re-emerged in the majority of patients who had developed sequential resistance to LAM, ADV, and ETV during LAM plus ADV therapy. The rtA181T/V mutation emerged after reversion to wild-type HBV from the strains harboring rtM204V + rtT184L or rtS202G during therapy, and existed in different genomes with LAM- or ETV-resistant mutations. The co-localization of MDR mutants to the same genome of virus was rare. A suboptimal response to LAM plus ADV therapy may not result from the co-localization of MDR HBV mutations to the same genome, but instead from the low antiviral potency of these drugs. Thus, NAs with a more powerful antiviral effect such as TDF plus ETV therapy might be an
- 27 -
effective combination strategy for the treatment of HBV patients with MDR to LAM, ADV, and ETV.
- 28 -
V. CONCLUSIONS
In conclusion, the present clonal sequencing data revealed that the rtA181 mutation re-emerged in the majority of patients who had developed sequential resistance to LAM, ADV, and ETV during LAM plus ADV therapy. The rtA181T/V mutation emerged after reversion to wild-type HBV from the strains harboring rtM204V + rtT184L or rtS202G during therapy, and existed in different genomes with LAM- or ETV-resistant mutations. The co-localization of MDR mutants to the same genome of virus was rare. A suboptimal response to LAM plus ADV therapy may not result from the co-localization of MDR HBV mutations to the same genome, but instead from the low antiviral potency of these drugs. Thus, NAs with a more powerful antiviral effect such as TDF plus ETV therapy might be an effective combination strategy for the treatment of HBV patients with MDR to LAM, ADV, and ETV.
- 29 -
REFERENCES
1. Berg T, Marcellin P, Zoulim F, Moller B, Trinh H, Chan S, Suarez E, Lavocat F, Snow Lampart A, Frederick D, Sorbel J, Borroto-Esoda K, Oldach D, Rousseau F: Tenofovir is effective alone or with emtricitabine in adefovir-treated patients with chronic-hepatitis B virus infection. Gastroenterology 139: 1207-1217, 2010
2. Brunelle MN, Jacquard AC, Pichoud C, Durantel D, Carrouee-Durantel S, Villeneuve JP, Trepo C, Zoulim F: Susceptibility to antivirals of a human HBV strain with mutations conferring resistance to both lamivudine and adefovir. Hepatology 41: 1391-1398, 2005
3. Cho SW, Koh KH, Cheong JY, Lee MH, Hong SP, Yoo WD, Kim SO: Low efficacy of entecavir therapy in adefovir-refractory hepatitis B patients with prior lamivudine resistance. J Viral Hepat 17: 171-177, 2010
4. EASL: EASL Clinical Practice Guidelines: management of chronic hepatitis B. J
Hepatol 50: 227-242, 2009
5. Heo NY, Lim YS, Lee HC, Chung YH, Lee YS, Suh DJ: Lamivudine plus adefovir or entecavir for patients with chronic hepatitis B resistant to lamivudine and adefovir. J
Hepatol 53: 449-454, 2010
6. Hong SP, Kim NK, Hwang SG, Chung HJ, Kim S, Han JH, Kim HT, Rim KS, Kang MS, Yoo W, Kim SO: Detection of hepatitis B virus YMDD variants using mass spectrometric analysis of oligonucleotide fragments. J Hepatol 40: 837-844, 2004
- 30 -
7. Kim SS, Cheong JY, Lee DM, Lee MH, Hong SP, Kim SO, Cho SW: Adefovir-based combination therapy with entecavir or lamivudine for patients with entecavir-refractory chronic hepatitis B. J Med Virol 84: 18-25, 2012
8. Kwon HC, Cheong JY, Cho SW, Choi JM, Hong SP, Kim SO, Yoo WD: Emergence of adefovir-resistant mutants after reversion to YMDD wild-type in lamivudine-resistant patients receiving adefovir monotherapy. J Gastroenterol Hepatol 24: 49-54, 2009
9. Lampertico P, Vigano M, Manenti E, Iavarone M, Sablon E, Colombo M: Low resistance to adefovir combined with lamivudine: a 3-year study of 145 lamivudine-resistant hepatitis B patients. Gastroenterology 133: 1445-1451, 2007
10. Lim YS, Lee JY, Lee D, Shim JH, Lee HC, Lee YS, Suh DJ: Randomized Trial of Entecavir plus Adefovir in Patients with Lamivudine-Resistant Chronic Hepatitis B Who Show Suboptimal Response to Lamivudine plus Adefovir. Antimicrob Agents
Chemother 56: 2941-2947, 2012
11. Liu Y, Wang C, Zhong Y, Chen L, Li X, Ji D, Wang H, Xin S, Zoulim F, Xu D: Evolution and suppression of HBV strains with multidrug resistance to lamivudine, adefovir dipivoxil and entecavir in a patient with chronic hepatitis B. Antivir Ther 15: 1185-1190, 2010
12. Lok AS, McMahon BJ: Chronic hepatitis B: update 2009. Hepatology 50: 661-662, 2009
- 31 -
13. Pallier C, Rodriguez C, Brillet R, Nordmann P, Hezode C, Pawlotsky JM: Complex dynamics of hepatitis B virus resistance to adefovir. Hepatology 49: 50-59, 2009
14. Patterson SJ, George J, Strasser SI, Lee AU, Sievert W, Nicoll AJ, Desmond PV, Roberts SK, Locarnini S, Bowden S, Angus PW: Tenofovir disoproxil fumarate rescue therapy following failure of both lamivudine and adefovir dipivoxil in chronic hepatitis B. Gut 60: 247-254, 2011
15. Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ: Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B.
Hepatology 45: 307-313, 2007
16. Shaw T, Bartholomeusz A, Locarnini S: HBV drug resistance: mechanisms, detection and interpretation. J Hepatol 44: 593-606, 2006
17. Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP: Hepatitis B virus infection: epidemiology and vaccination. Epidemiol Rev 28: 112-125, 2006
18. Tan J, Degertekin B, Wong SN, Husain M, Oberhelman K, Lok AS: Tenofovir monotherapy is effective in hepatitis B patients with antiviral treatment failure to adefovir in the absence of adefovir-resistant mutations. J Hepatol 48: 391-398, 2008
19. van Bommel F, de Man RA, Wedemeyer H, Deterding K, Petersen J, Buggisch P, Erhardt A, Huppe D, Stein K, Trojan J, Sarrazin C, Bocher WO, Spengler U, Wasmuth HE, Reinders JG, Moller B, Rhode P, Feucht HH, Wiedenmann B, Berg T: Long-term
- 32 -
efficacy of tenofovir monotherapy for hepatitis B virus-monoinfected patients after failure of nucleoside/nucleotide analogues. Hepatology 51: 73-80, 2010
20. Villet S, Billioud G, Pichoud C, Lucifora J, Hantz O, Sureau C, Deny P, Zoulim F: In vitro characterization of viral fitness of therapy-resistant hepatitis B variants.
Gastroenterology 136: 168-176 e162, 2009
21. Villet S, Ollivet A, Pichoud C, Barraud L, Villeneuve JP, Trepo C, Zoulim F: Stepwise process for the development of entecavir resistance in a chronic hepatitis B virus infected patient. J Hepatol 46: 531-538, 2007
22. Warner N, Locarnini S: The antiviral drug selected hepatitis B virus rtA181T/sW172* mutant has a dominant negative secretion defect and alters the typical profile of viral rebound. Hepatology 48: 88-98, 2008
23. Yim HJ, Hussain M, Liu Y, Wong SN, Fung SK, Lok AS: Evolution of multi-drug resistant hepatitis B virus during sequential therapy. Hepatology 44: 703-712, 2006
24. Zoulim F, Locarnini S: Hepatitis B virus resistance to nucleos(t)ide analogues.
Gastroenterology 137: 1593-1608 e1591-1592, 2009
25. Zoulim F, Locarnini S: Management of treatment failure in chronic hepatitis B. J
- 33 - 국문요약
-라미부딘과 아데포비어 병합요법 중 다약제 내성 만성 B 형간염
바이러스의 동태
아주대학교 대학원의학과 김 순 선 (지도교수 : 조 성 원) 목적: 다약제 내성을 보이는 만성 B 형간염 바이러스는 항바이러스제에 감수성이 떨어지는 것으로 알려져 있으나, 내성 변이가 같은 바이러스의 게놈에서 발생하는지는 아직 규명되어 있지 않다. 본 연구는 라미부딘, 아데포비어, 엔테카비어로 순차적인 치료를 받으면서 다약제 내성이 발생한 만성 B 형간염 환자를 대상으로 라미부딘과 아데포비어 병합 구제요법시 내성 바이러스 동태를 clonal sequencing 방법으로 알아보고자 하였다. 방법: 모두 여섯 명의 환자를 대상으로 하였으며 병합요법 시작 전에 각 20 clone 씩 총 120 clone 을 분석하였으며, 치료 도중 180 clone 에 대해 분석을 시행하였다.결과: 병합요법 전 모든 clone 은 rtM204V 변이를 가지고 있었으며 108 개의 clone 에서 엔테카비어 내성 변이가 함께 발견되었고 rtA181 이나 rtN236 변이는 관찰되지 않았다. 병합요법 치료 중 분석한 180 clone 중 39 개의 clone 에서 rtA181T/V (± rtN236T) 변이가 발견되었으며 이중 엔테카비어
- 34 - 내성 변이가 같이 발견된 것은 2 개의 clone 뿐이었다. rtA181T/V 변이는 엔테카비어 내성변이가 야생형으로 되돌아간 후에 발생하였다. 여섯명 의 환자 중 다섯 명은 병합요법에 부분 바이러스 반응만을 보였다. 결론: 다약제 내성 변이는 대부분 다른 바이러스 게놈에 존재하며, 그러므로 병합요법이 효과적이지 않았던 이유는 여러 변이들이 같은 바이러스 게놈에 존재해서가 아니라 약제의 항바이러스 효과가 낮아서였던 것으로 생각된다. 따라서 더 강력한 항바이러스제제의 병합요법이 효과적인 구제 치료법이 될 수 있을 것으로 사료된다. 핵심어 : 만성 B 형간염, Clonal sequencing, HBV DNA, 다약제 내성, 바이러스 게놈