대한소화기학회지 2000;35:429 - 438
Helicobacter py lori 제균 및 십이지장궤양 치유를 위한 Ranitidine B is m u t h C it r a t e 와 C la r it h r om y cin 병용요법의 효능
중앙대학교 의과대학 내과학교실, 울산대학교 의과대학 내과학교실*, 고려대학교 의과대학 내과학교실†
박실무・홍원선*・김재규・김진호†
Th e E ffi c a c y o f R a n i t i d i n e B i s m u t h Ci t r a t e p lu s Cla ri t h r o m y c i n fo r t h e Eradica tion o f Helicoba cter p ylor i a nd the He a ling of Duo de n al Ulc e r
Sill-Moo Park, M.D., We on-Se on Hong, M.D.*, J ae Gyu Kim, M.D. a nd J in-Ho Kim, M.D.†
Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul;
Department of Internal Medicine, University of Ulsan College of Medicine*, Seoul;
Department of Internal Medicine, Korea University College of Medicine†, Seoul, Korea
Background/Aims: To assess the safety and the efficacy of the combined therapy of ranitidine
bismuth citrate (RBC) with clarithromycin on the eradication of Helicobacter pylori (H. pylori) and the healing of duodenal ulcer, we performed this study. The combined therapy of RBC 400 mg and clarithromycin 500 mg was indicated to be taken twice daily. Methods: Eighty-two patients with active duodenal ulcer were confirmed to haveH. pylori
infection. This was an open, non-comparative, multicentre study. After 2-weeks treatment with RBC and clarithromycin, RBC alone was administered for following 2 weeks. Ulcer status was assessed by endoscopy at the beginning and the end of treatment. H. pylori status was assessed by CLO test and histological test at the beginning and 4 weeks after the completion of treatment. At the beginning, 2 weeks and 4 weeks after the start of treatment, ulcer symptoms were recorded on a scale of absent, mild, moderate or severe. Results: Fifty-seven patients underwent an evaluable CLO test and histological test 4 weeks after the completion of treatment. The eradication rates of H. pylori was 70.2% (40/57) in the combined therapy of RBC plus clarithromycin. Ulcer healing rates at the end of treatment and 4-6 weeks after the completion of treatment were 88.2% (60/68) and 89.5% (51/57), respectively.Conclusions: The coadministration of RBC and clarithromycin is a simple, well-tolerated and effec-
tive treatment for active H. pylori-associated duodenal ulcer disease. (Kor J Gastroenterol 2000;35:429 - 438)
Key Words: H. pylori, Duodenal ulcer, Ranitidine bismuth citrate, Clarithromycin, Eradication
접수: 1999년 5월 12일, 승인: 1999년 12월 29일
연락처: 김진호, 152-050, 서울시 구로구 구로동 80, 고려의대 구로병원 내과 Tel: (02) 818-6628, Fax: (02) 854-8453
430 대한소화기학회지 : 제 35 권 제 4 호 2000
서 론
십이지장궤양 환자의 90% 이상이 Helicobacter pylori(이하 H. pylori로 약함)에 감염되어 있으며,1-5 감염이 있을 경우 궤양의 치료 경과에 중요한 영향 을 미치는 것으로 알려져 있다.6,7 십이지장궤양 환 자의 일시적인 궤양 치유는 위산분비억제제 단독 사용으로도 80% 이상에서 가능하나, H. pylori 제균 요법을 병행하지 않을 경우 재발률이 높고8 제균요 법을 시행하여 제균이 성공적으로 이루어진 경우에 는 재발률이 현저히 낮아진다.8,9 1994년 미국 국립 보건원의 합의 도출을 위한 모임과 그 이후에 개최 된 여러 회의에서 H. pylori 감염이 있는 위 십이지 장궤양 환자에게는 반드시 제균요법을 권유하였 다.10 이후 많은 항생제를 단독 또는 병합하여 투여 한 후 제균율을 검증하였으나 아직까지 제균 효과 가 완전한 치료법은 없다.11
현재까지도 효과적인 제균요법의 하나로 인정되 고 있는 복합 처방은 비스므스 염(bismuth salt) 한 가지에 한 가지 또는 두 가지의 항생제를 병용하는 방법이다.12-15 그러나 약제 복용의 순응도(compliance), 부작용 발현율,16-20 메트로니다졸에 대한 내성균 출 현율 등19,20 여러 가지 문제점이 있어 이 병용요법의 제한성이 동시에 언급되고 있다.
한편 최근에 개발되어 궤양 치료의 새로운 장을 연 proton pump inhibitor(이하 PPI로 약함) 제제 한 가지와 두 가지 항생제의 병용요법이 H. pylori 제균 에 효과적임이 보고된 이후, PPI 제제에 두 가지 또 는 경우에 따라서는 세 가지의 항생제를 병합하여 치료하는 경향이 점차 높아지고 있다. 그러나 우리 나라에서는 이들 약제의 제균 효과에 관한 전향적 인 연구가 부족하여 외국의 시험 성적을 기초로 사 용하고 있는 실정이며, 치료 비용이 고가라는 점도 문제가 되고 있다.
Ranitidine bismuth citrate (RBC; Tritec or Py- lorid; GlaxoWellcome Inc, Greenford, UK. 이하 파 이로리드로 약함)는 라니티딘 염과 비스므스 및 싸 이트레이트의 화합체로서 종래의 염산 라니티딘과 비스므스 싸이트레이트를 단순 혼합한 경우와는 다
른 독특한 약리작용을 지닌 새로운 약제이다.21 이 약제는 라니티딘의 위산분비 억제 효과와 비스므스 의 위, 십이지장점막 보호작용 및 H. pylori 제균 효 과를 동시에 지니고 있으며8,22 십이지장궤양 치유율 은 종래의 라니티딘제제와 흡사하나 위궤양 치유율 은 더 높은 것으로 밝혀져 있다.23,24 또 파이로리드 는 복용상의 순응도가 우수하고,23-27 체외 시험에서 메트로니다졸 또는 클래리스로마이신 내성 균주의 발생을 억제하는 효과가 있다고 알려져 있으며,28 파 이로리드와 클래리스로마이신 2제 병용요법은 H.
pylori 제균 효과가 우수하다고 보고되어 있다.29-31 저자들은 국내 환자들에서 이 병용요법의 H. pylori 제균 효과와 십이지장궤양 치유율을 검토하여 그 결과를 보고하는 바이다.
대상 및 방법
1. 대 상
내시경검사상 직경 2.0 cm 이하의 A1, A2 및 H1 형 십이지장궤양 환자 중 H. pylori 감염이 증명된 82명을 대상으로 하였으며, 남자는 66명(평균 연령 41.9세), 여자는 16명(평균 연령 46.3세)이었다. 대상 환자의 특성은 Table 1과 같다. H. pylori 감염 양성 은 위체부 및 위전정부 조직편을 이용한 CLO검사 와 조직학적 검사(modified Giemsa stain) 결과가 공 히 양성인 경우로 정의하였으며, 일반혈액검사와 혈 액화학검사상 제외 기준에 포함되지 않는 예들을 선정하였다. 18세 미만 80세 이상의 환자, 역류성 식도염, 식도정맥류, 유문 전 궤양, 유문구 궤양, 유 문 협착 또는 폐색증이 있는 환자나 기타 임상적으 로 유의한 위장 장애가 있는 환자, 내시경검사 후 5 일 이내에 투약을 시작할 수 없는 환자, 식도 수술, 위-식도괄약근 수술, 식도열공 헤르니아 치료 또는 궤양 천공 봉합을 제외한 상부위장관 수술을 받은 환자, 직경 2.0 cm 이상의 십이지장궤양 환자, 경구 스테로이드, 비스테로이드성 항염증제제, 베타히스 틴, 니코틴산 유도체 등 위, 십이지장점막에 궤양을 유발시킬 수 있는 것으로 알려진 약물을 계속 복용 해야만 하는 환자, 지난 30일 이내에 gold 요법을 받은 환자나 gold 요법을 필요로 하는 환자, 2주의
박실무 외 3인. RBC와 클래리스로마이신 병용요법 431
병용 투여 기간 동안 클래리스로마이신과 상호작용 의 가능성이 있는 약물을 계속 투여해야 하는 환자 (예; cyclosporin, digoxin, ergotamine, hexabarbital, warfarin, oral anticoagulants, phenytoin, trazolam, terfenadine, theophylline, bromocriptine, cisapride 및 carbamazepine 등), 임산부나 수유부 또는 적당한 피 임을 하지 않는 가임 여성, 상부위장 생검에서 조직 학적으로 악성종양이 의심되거나 확인된 환자, 활동 성 상부위장관 출혈, 가시성 또는 유착성 응괴가 있 는 환자, Zollinger-Ellison 증후군, 기타 병리학적 과 분비 상태에 있는 환자 및 염산결핍증 환자, 안정되 지 않고 임상적으로 유의한 신경계질환, 심혈관계질 환, 폐질환, 정신질환, 대사성질환, 또는 내분비질환 이 있는 환자, 간기능검사상 AST/ALT가 정상 범위 상한치의 2배를 넘는 환자, 신기능 장애 환자(혈청 creatinine >200 μmol/L), 처음 내시경 검사 전 30일 이내에 비스므스 함유 약물을 복용한 환자, 연구 시 작 전 30일 이내에 임상시험용 약품의 임상연구에 참여했던 환자, 연구 시작전 14일 이내에 H. pylori 에 효과적인 것으로 알려진 경구 또는 정맥주사용 항생제/항균제가 투여된 환자 또는 16일 이내에 4일 이상 연속으로 tinidazole, metronidazole, azithromy- cin, omidazole, roxithromycin, clarithromcyin, peni-
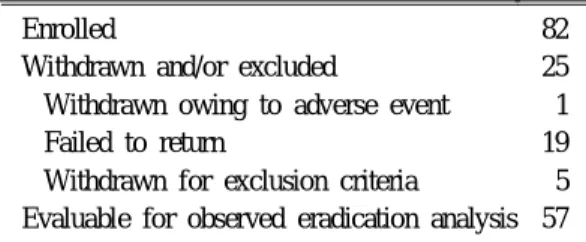
cillin, bacampicillin, oxacillin, pivampicillin, amoxi- cillin, tetracycline, erythromycin, rifaximin, cerfixime, ciprofloxacin, oflaxacin, nitrofurantoin, furazolidine 등의 항생제가 투여된 환자, 약물 또는 알코올 남용 의 기왕력이 있는 환자, H2 수용체 길항제, 비스므 스 함유 화합물 또는 macrolides에 과민반응을 보이 는 환자, 본 연구를 수행하는데 방해가 될 가능성이 있거나 환자에게 위험성이 있다고 판단되는 경우와, 본 연구를 위한 지시나 계획에 따를 수 없다고 판단 되는 환자는 연구에서 제외하였다. 모든 대상 환자 로부터 서면 동의서를 받았다. 82명의 환자 중 투약 시작 4주일 후 1차 위 내시경 추적검사가 가능하였 던 환자는 68명이었으며 치료 종료 28일 후부터 42 일 사이에 2차 추적 위내시경검사를 시행하여 H.
pylori 제균 효과 판정이 가능하였던 환자는 57명이 었다(Table 2). 이들 68명의 환자군과 57명의 환자 군을 각각 궤양 치유 효과 판정과 H. pylori 제균 효 능 판정 분석 대상 피험자군으로 선정하였다.
2. 방 법 1) 시험 약제 투약
모든 대상 환자에서 병력 청취와 신체 진찰을 실 시하였으며, 통증, 구역, 속쓰림, 구토 등 소화성 궤 Table 1. Demography of Patients Assigned to Therapy
Number of patients Male
Age (mean±SD)(years) Female
Age (mean±SD)(years) Smoker (%)
Drinker (%)
No. of patients with a previous ulcer history (%) Yes
No
If yes, duration since first diagnosis (months) 0-12
13-24 25-60 61-120 120≤
82 66 41.9±10.9
16 46.3±11.5
62.2 53.7 43 (52.4) 39 (47.6)
4 6 15 13 5
432 The Korean Journal of Gastroenterology : Vol. 35, No. 4, 2000
양에 수반될 수 있는 증상들을 심한 정도에 따라 1) 없음 2) 경증(약간의 증상은 있으나 일상 생활에 지장이 없음) 3) 중등증(일상 생활에 다소 지장을 줌) 4) 중증(일상 생활의 유지가 불가능함)으로 분류 하여 평가하였다. 처음 2주일간 파이로리드 400 mg 1정과 클래리스로마이신 250 mg 2정을 1일 2회 식 후에 복용토록 하였으며, 투약 기간 중 궤양 치유에 영향을 미칠 수 있다고 판단되는 다른 약제의 복용 을 금지하였다.
2주일의 투약을 완료한 모든 환자에서 통증, 구 역, 속쓰림, 구토 등 기존 증상의 변화를 평가하였으 며 시험 약제 복용 순응도와 시험 약제 이외의 약제 복용 여부를 확인하였다. 시험 약제 복용의 순응도 를 검증하기 위하여 방문시 각각의 약제 포장지를 수거하여 남은 약제가 있는지와 복용 방법이 지시 대로 정확하게 실행되었는지를 확인하였다. 아울러 흑변을 비롯한 부작용의 발현 여부도 확인하였으며, 흑변이 임상적으로 위장관 출혈의 가능성을 시사한 다고 판단될 때에는 대변잠혈검사를 시행하여 진성 출혈 여부를 검증하였다. 처음 2주일간의 시험 약제 투약이 만족하게 시행된 환자에 한해서 파이로리드 400 mg 1정을 하루 2회 2주일간 추가로 투약하였다.
2) 궤양 치유 확인 및 부작용 발현 확인 투약 시작 4주일 후 방문시에 다시 기존 궤양 증 상의 변화, 약제에 대한 순응도, 시험 약제 이외의 다른 약제 복용 유무 등을 확인하고 부작용 발현 여 부를 확인하였다. 또한 일반혈액검사 및 혈액화학검 사를 재차 시행하여 자각증상의 변화뿐 아니라 객 관적인 검사상의 부작용 발현 여부도 검증하였다.
동시에 궤양 치유 확인을 위한 1차 추적 위내시경검 사를 시행하였으며, 시험 약제의 십이지장궤양 치유 율은 이 1차 추적 위내시경검사 결과로 판정하였다.
추적 위내시경검사에서 궤양이 완치되지 않은 환자 들에서는 라니티딘을 하루에 300 mg씩 4주일간 추 가로 복용하도록 하였다.
3) H . p y lori 제균 판정
모든 대상 환자에서 파이로리드 투여 종료 28일 후 부터 42일 사이에 2차 추적 위내시경검사를 시 행하였다. 2차 추적 위내시경검사시 전정부, 위체부 및 위저부로부터 점막편을 채취하여 CLO검사와 조 직학적 염색검사를 시행하여 H. pylori 제균 여부를 확인하였다. 모든 점막편의 검사 결과가 공히 음성 인 경우에 제균이 성공하였다고 판정하였다. 이 기 간 동안 시험 약제 이외에 다른 약제의 복용 유무도 재차 확인하였다.
결 과
1. 궤양 치유율
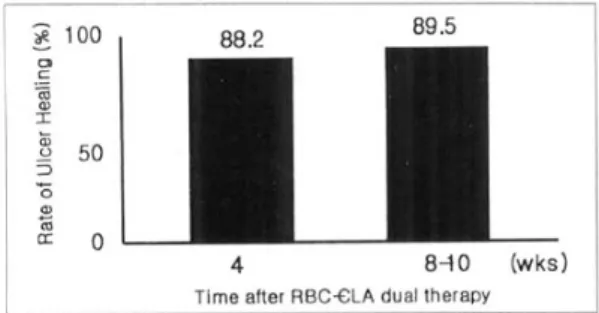
4주일 치료 후 1차 추적 위내시경검사로 궤양의 완 치 여부를 평가하였으며, 시행한 68예에서의 궤양 치 유율은 88.2% (60/68)이었다. 또한 치료 종료 28-42 일 사이에 2차 추적검사가 가능했던 57예에서의 궤양 치유율은 89.5% (51/57)이었으며 8주 이후에도 궤양 이 치유되지 않았던 환자는 1예이었다(Fig. 1).
2. 궤양 증상의 경감도
궤양 증상은 없음, 경증, 중등증, 중증으로 분류하 여 평가하였으며 4주일 치료 후 궤양의 완치 여부를 평가할 수 있었던 68명의 환자들을 대상으로 증상의 경감도를 판정하였다. 궤양 통증은 2주일 후 62명의 환자에서, 4주일 후 64명의 환자에서 소실되었으며, 구역은 2주일 후와 4주일 후에 각각 67명의 환자에 서 소실되었다. 속쓰림은 2주일 후 62명, 4주일 후 63명의 환자에서 소실되었고 구토는 2주일 후 67명, 4주일 후 68명의 환자에서 소실되었다(Table 3).
Table 2. Reasons for Withdrawal and Exclusion from Observed Eradication Analysis at 4 weeks after the End of Treatment
Enrolled
Withdrawn and/or excluded
Withdrawn owing to adverse event Failed to return
Withdrawn for exclusion criteria Evaluable for observed eradication analysis
82 25 1 19 5 57
Park, et al. The Efficacy of RBC plus Clarithromycin Treatment 433
3. H . p y lori 제균율
H. pylori 제균율은 파이로리드와 클래리스로마이 신을 2주일간 병용 투약 후 파이로리드만 2주일간 단독 투약받는, 4주일간의 시험 약제 복용을 규정에 따라 성공적으로 완료하고, 치료 약제 투약 완료 28
일 후부터 42일 사이에 2차 추적 위내시경검사를 받은 환자 57예를 대상으로 전정부, 위체부 및 위저 부의 내시경 생검 점막편을 이용한 CLO검사와 조 직학적 염색검사가 모두 음성인 경우를 제균 성공 예로 판정하여 산출하였다. 중도 탈락 환자들과 2차 추적 위내시경검사가 불가능하였던 환자들은 분석 에서 제외하였다. 제균된 환자는 총 40예로 시험 약 제의 H. pylori 제균율은 per protocol 분석에서 70.2% (40/57)였으며 intention to treat 분석에서 51.9% (40/77)이었다(Fig. 2).
4. 약제에 대한 부작용 및 순응도
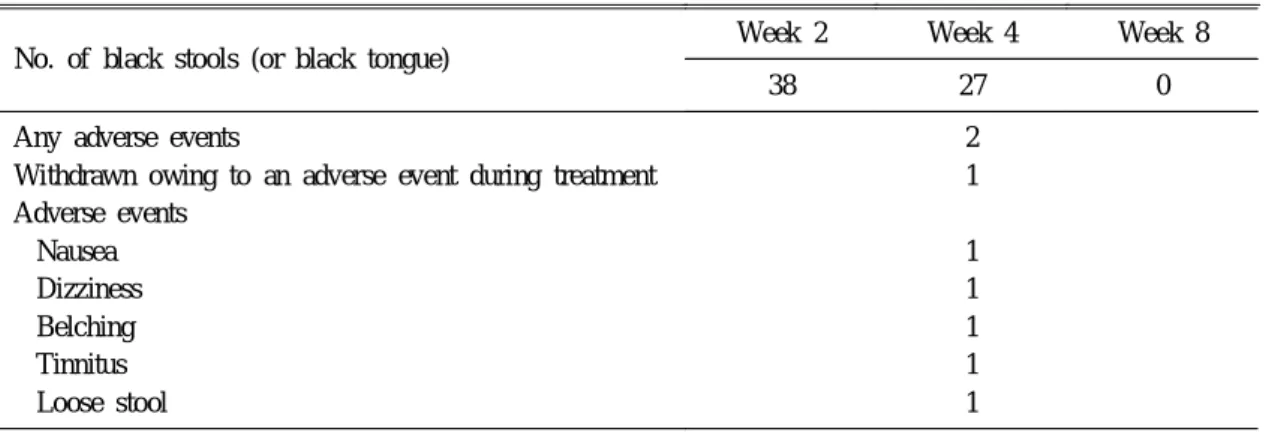
파이로리드의 부작용으로는 구역, 트림, 어지러 움, 이명, 연변 등이 관찰되었으나 투약이 중단된 환 자는 1예에 불과하였다(Table 4). 2주 이상 투약이 완료된 73명의 환자 중 1예가 구역과 어지러움으로 투약이 중단되어서 이들 환자에 있어서 약제에 대 한 순응도는 98.6% (72/73)였다.
고 찰
1994년 미국 국립보건원의 합의 도출을 위한 모 임에서 권유된 사항은 H. pylori에 감염이 확인된 십 이지장궤양 환자에서는 반드시 H. pylori 제균요법 을 시행하는 것이다.10 한편 1990년 세계 소화기학 회가 주관한 H. pylori 연구 소위원회가 공식적으로 제시한 최초의 H. pylori 제균요법은 비스므스 염, 메트로니다졸, 및 테트라싸이클린의 3가지 약제를 2 주일간 병용 투여하는 것이었으나, 메트로니다졸 제 제에 대한 약제 내성균의 출현이 많을 뿐 아니라 복 용 순응도가 좋지 않다는 것이 밝혀졌기 때문에 이 3제요법은 가격이 비교적 저렴함에도 불구하고 근 래에는 거의 사용되지 않고 있다. 그 후 PPI를 기초 로 하는 제균요법의 우수한 결과가 보고됨에 따라, 지금은 PPI를 기본 약제로 하는 3제요법이 근간을 이루고 있다. 그러나 1997년 2월 미국의 식품의약청 (FDA)이 인정한 H. pylori 제균요법은 세 가지 종류 로 PPI와 클래리스로마이신 병용요법, 파이로리드 와 클래리스로마이신 병용요법, 비스므스 염, 메트로 니다졸, 테트라싸이클린 및 H2 수용체 길항제 4제병 Fig. 1. Rate of ulcer healing according to time period. At
4 weeks, the ulcer was healed completely in 60 of 68 patients (88.2%). At 8-10 weeks, the ulcer was healed completely in 51 of 57 patients (89.5%). RBC, ranitidine bismuth citrate; CLA, clarythromycin.
Table 3. Comparison of Ulcer Symptoms at Week 0, Week 2 and Week 4 (N=68)
Type of symptom
No. of patients Week 0 Week 2 Week 4 Ulcer pain
Absent Mild Moderate Severe Nausea
Absent Mild Moderate Severe Heart burn
Absent Mild Moderate Severe Vomiting
Absent Present
12 25 21 10 55 7 5 1 26 21 18 3 64 4
62 6 0 0 67 1 0 0 62 6 0 0 67 1
64 4 0 0 67 1 0 0 63 4 1 0 68 0
434 대한소화기학회지 : 제 35 권 제 4 호 2000
Table 4. Patients Experiencing an Adverse Events and Black Stools (or Black Tongue)
No. of black stools (or black tongue)
Week 2 Week 4 Week 8
38 27 0
Any adverse events
Withdrawn owing to an adverse event during treatment Adverse events
Nausea Dizziness Belching Tinnitus Loose stool
2 1 1 1 1 1 1 Fig. 2. Rate of H. pylori eradication. Five of 82 patients were withdrawn owing to exclusion criteria. The eradication rate of intention to treat (ITT) analysis was 51.9% (40/77) and that of per protocol (PP) analysis was 70.2% (40/57).
Table 5. Dose, Frequency, and Duration of FDA-Approved Regimens for H. pylori Eradication to Reduce Duodenal Ulcer Recurrence
Regimen Agent Dose Frequency Duration
1
2 3
Omeprazole (1st and 2nd wk) Omeprazole (3rd and 4th wk) Clarithromycin (1st and 2nd wk) RBC
Clarithromycin Bismuth subsalicylate Metronidazole Tetracyclin HCl H2-receptor antagonist
40 mg 20 mg 500 mg 400 mg 500 mg 525 mg 250 mg 500 mg as described
qd qd tid bid tid qid qid qid as described
2 wk 2 wk 2 wk 4 wk 2 wk 2 wk 2 wk 2 wk as described RBC, ranitidine bismuth citrate.
박실무 외 3인. RBC와 클래리스로마이신 병용요법 435
용요법 등이다(Table 5).
유럽의 5개 의료기관에서 파이로리드와 클래리스 로마이신 병용요법의 결과를 보고하였는데 파이로 리드 1일 400 mg 또는 800 mg 1일 2회, 클래리스로 마이신 250 mg 1일 3회 또는 4회를 투여한 후의 H.
pylori 제균율은 각각 82%, 86%, 84% 및 92%이었 다. 클래리스로마이신 복용 방법을 1일 500 mg 2회 로 할 경우 제균율은 93%와 96%로 향상되었으나 파이로리드의 용량에 따른 제균율의 차이는 의미가 없었다.6,7,10,17,18 본 연구의 기본 골격은 상기한 외국 의 임상시험과 동일하였으나 연구 결과는 70.2%의 낮은 제균 효과를 보여 동일한 2제요법을 사용한 서 양의 보고와 현격한 차이를 보이고 있다. 이와 같은 차이의 기전을 정확하게 설명하기는 본 시험만으로 는 충분하지 않으나 Cag A 단백과 같은 H. pylori의 독성인자의 발현율이 국가간 또는 인종간 차이가 있으며, 지역에 따라 미생물학적 특성이 다른 균주 가 존재할 것이라는 연구 보고를32-34 참고하면 비록 본 시험에서는 시도되지 않았으나 우리 나라 환자 에서 분리된 H. pylori의 파이로리드 또는 클래리스 로마이신에 대한 감수성의 차이가 한 원인이 될 수 있을 것으로 생각된다. 미국의 FDA에서 파이로리 드와 클래리스로마이신 2제병용요법일 경우 클래리 스로마이신 용량을 1일 1,500 mg (500 mg tid)으로 권유하고 있고, 클래리스로마이신을 500 mg씩 1일 3회 복용시킨 후 제균율이 유의하게 증가되었다는 Peterson 등35의 보고를 참조하면 본 시험에서 사용 한 클래리스로마이신의 용량이 충분하지 않았을 가 능성도 있다 하겠다.
한편 투약을 중단할 정도의 심각한 부작용을 경 험한 환자는 1예에 불과하였고, 치료 전후로 시행한 신체 진찰 및 혈액학적 검사에서도 특이한 이상 소 견을 보인 환자는 없었다. 따라서 파이로리드와 클 래리스로마이신 2제요법은 그 순응도가 우수하고 안전한 것으로 판단된다.
비스므스 제제 중에는 비스므스 subgallate, 또는 비스므스 subnitrate 등 독성을 일으키는 약제가 있 고, 파이로리드를 단독 복용한 경우에 비해 파이로 리드와 클래리스로마이신을 병용한 경우 혈중 비스 므스 농도가 증가하지만 임상적으로 유의한 정도의
독성이 증명된 적은 없다.30 최근 흔히 사용되고 있 는 두 가지 또는 세 가지 종류의 항생제를 병용하는 일부 제균요법은 약제 복용의 순응도가 낮거나, 고 가라는 점도 약제 선택시 고려하여야만 한다.
현재 일반적으로 추천되고 있는 PPI와 2가지 항 생제를 병합한 3제요법의 경우는 약제의 용량과 기 간에 따른 차이는 있으나 79-96%의 박멸률을 보이 고 있으며 대개 90% 내외의 박멸률을 보이고 있 다.36-38 그러나 PPI와 1가지 항생제를 병합한 2제요 법은 초기에는 박멸률이 우수한 것으로 보였으나 추시에서 효과적인 치료법이 아님이 판정되었으며 omeprazole (40 mg/day)+clarythromycin (500 mg tid)의 경우 박멸률이 83%로 보고되었다.39 본 연구 에서 PPI-3제요법보다 다소 낮은 결과를 보인 것은 2제요법의 한계라고 판단되며 향후 RBC-3제요법과 의 비교 연구를 통하여 RBC-병합요법의 유효성을 평가하여야 할 것이다.
이상의 결과를 종합하면 국내의 십이지장궤양 환 자에서 400 mg 파이로리드 1일 2회, 클래리스로마 이신 500 mg 1일 2회 2주일간 병용 투여 후 파이로 리드 400 mg만을 1일 2회 2주일간 추가 복용하는 치료법의 H. pylori 제균율은 70.2%로 외국의 보고 에 비하여 낮은 경향을 보이나, 궤양 증상의 소실, 궤양 치유의 효율성, 약제 복용의 순응도, 처방의 간 편성 및 경미한 부작용 발생 등을 고려하면 H.
pylori에 감염된 십이지장궤양 환자 치료에 새로운 치료법의 하나로 추천할 수 있을 것으로 여겨지며 RBC-3제요법과 비교를 포함한 추가적인 연구가 필 요할 것으로 보인다.
요 약
목적: 2주간의 ranitidine bismuth citrate 400 mg 1정과 clarithromycin 250 mg 2정의 1일 2회 복용이 십이지장궤양의 치유와 H. pylori 제균에 미치는 효 과와 안정성을 조사하기 위해 본 연구를 시행하였 다. 대상 및 방법: 본 연구는 다기관, 공개, 비비교 (noncomparative)방법을 통하여 시행하였고, H.
pylori 감염 양성인 활동성 십이지장궤양 환자 82명 을 대상으로 하여 모든 환자는 ranitidine bismuth
436 The Korean Journal of Gastroenterology : Vol. 35, No. 4, 2000
citrate와 clarithromycin으로 2주간 치료 후 2주간 ranitidine bismuth citrate를 투여받았다. 궤양 크기는 연구 시작 개시와 종료시 내시경으로 평가하였으며 H. pylori 감염 유무는 연구 개시 및 치료 종료 4-6 주 뒤 CLO검사와 조직학적 검사에 의해 평가되었 다. 궤양 증상은 연구 개시와 투약 시작 2주와 4주 에 각각 평가되었다. 결과: 치료 약제 투약 완료 4-6 주 후에 2차 추적 위내시경검사를 받은 환자 57예 의 H. pylori 제균율은 per protocol 분석에서 70.2%
(40/57)였으며 intention to treat 분석에서 51.9%
(40/77)이었다. 4주 치료 후 치유 여부의 평가가 가 능했던 68예의 궤양 치유율은 88.2% (60/88)였고, 치료 종료 4-6주후 추적검사가 가능했던 57예의 궤 양치유율은 89.5% (51/57)였다. 결론: Ranitidine bismuth citrate와 clarithromycin의 2제병합요법은 기 존의 PPI를 기본으로 하는 3제요법에 비하여 박멸 률이 다소 떨어지기는 하나 H. pylori 감염 양성 활 동성 십이지장궤양 환자의 치료에 간편하고 순응도 가 높은 치료법으로 생각된다.
색인단어: 십이지장궤양, H. pylori, Ranitidine bis- muth citrate, Clarithromycin, 제균
참 고 문 헌
1. Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulcer patients. Lancet 1984;8390:1311-1315.
2. Peterson WL, Barnett CC, Evans DJ, et al. Acid secretion and serum gastrin in normal subjects and patients with duodenal ulcer: the role of Helico- bacter pylori. Am J Gastroenterol 1993;88:2038- 2043.
3. Tytgat GNJ, Noach LA, Rauws EAJ. Helicobacter pylori infection and duodenal ulcer disease. Gastro- enterol Clin North Am 1993;22:127-139.
4. Borody TJ, George LI, Branl S, et al. Helicobacter pylori negative duodenal ulcer. Am J Gastroenterol 1991;86:1154-1157.
5. Louw JA, Falck V, van Resebburg C, et al. Distri- bution of Helicobacter pylori colonization and
associated gastric inflammatory changes: difference between patients with duodenal and gastric ulcers. J Clin Pathol 1993;46:754-756.
6. Simon B, Cremer M, Dammann HG, et al. 300 mg nizatidine at night versus 300 mg ranitidine at night in patients with duodenal ulcer: a multicentre trial in Europe. Scand J Gastroenterol 1987;22(suppl 136):61-70.
7. Pace F, Colombo E, Ferrera A, et al. Nizatidine and ranitidine in the short-term treatment of duodenal ulcer: a cooperative double-blind study of once- daily bedtime administration. Am J Gastroenterol 1988;83:643-645.
8. Hentschel E, Brandstatter G, Dragosics B, et al.
Effect of ranitidine and amoxycillin plus metroni- dazole on the eradication of Helicobacter pylori and recurrence of duodenal ulcer. N Engl J Med 1993;
328:308-312.
9. Patchett S, Beattle S, Leen E, Keane C, O' Morian C. Helicobacter pylori and duodenal ulcer recur- rence. Am J Gastroenterol 1992;87:24-27.
10. NIH Consensus Conference. Helicobacter pylori in peptic ulcer disease. JAMA 1994;272:65-69.
11. Graham DY. Treatment of peptic ulcers caused by Helicobacter pylori. N Engl J Med 1993;328:349- 350.
12. O' Riordan T, Mathai E, Tobin E, et al. Adjuvant antibiotic therapy in duodenal ulcers treated with colloidal bismuth subcitrate. Gut 1990;31:999-1002.
13. deBoer WA, Driessen WM, Potters VP, Tytgat GNJ. Randomized study comparing 1 with 2 weeks of quadruple therapy for eradicating Helicobacter pylori. Am J Gastroenterol 1994;89:1993-1997.
14. Wilhelmsen I, Weberg R, Berstad K, et al. Helico- bacter pylori eradication with bismuth subcitrate, oxytetracycline and metronidazole in patients with peptic ulcer disease. Hepatogastroenterology 1994;
41:43-47.
15. Wilhelmsen I, Berstad A. Quality of life and relapse of duodenal ulcer before and after eradi- cation of Helicobacter pylori. Scand J Gastroenterol 1994;29:874-879.
Park, et al. The Efficacy of RBC plus Clarithromycin Treatment 437
16. Bell GD, Powell K, Burridge SM, et al. Experience with triple anti-Helicobacter pylori eradication therapy side effects and the importance of testing the pre-treatment bacterial isolate for metronidazole resistance. Aliment Pharmacol Ther 1992;6:427-435.
17. Marshall BJ, Hoffman SR, McCallum RW. Inci- dence of side effects during bismuth subsalicylate and antibiotic therapy for H. pylori. Gastro- enterology 1991;100(abstr):A117.
18. Thijis JC, Van Zwett AA, Oey HB. Efficacy and side effects of a triple drug regimen for the era- dication of Helicobacter pylori. Scand J Gastro- enterol 1993;28:934-938
19. European Study Group on Antibiotic Susceptibiltiy of Helicobacter pylori. Results of a multicentre Eu- ropean survey in 1991 of metronidazole resistance in Helicobacter pylori. Eur J Clin Microbiol Infect Dis 1992;11:777-781.
20. Glupczynski Y, Burrette A, DeKoster E, et al.
Metronidazole resistance in Helicobacter pylori.
Lancet 1990;335:976-977.
21. McColm AA, McLaren A, Klinkert G, et al. Rani- tidine bismuth citrate: a novel anti-ulcer agent with different physico-chemical characteristics and im- proved biological activity to a bismuth citrate-rani- tidine admixture. Aliment Pharmacol Ther 1996;10:
241-250.
22. Prewett EJ, Nwokolo CN, Hudson M, Sawyerr AM, Fraser A, Pounder RE. The effect of GR122311X, a bismuth compound with H2-antagonist activity on 24-hour intragastric acidity. Aliment Pharmacol Ther 1991;5:481-490.
23. Bailey RJ, Marlicz K, Rosch W, et al. GR122311X (ranitidine bismuth citrate) a new drug for the treat- ment of gastric ulcer. Gastroenterology 1995;108(abstr):
A51.
24. Bardhan KD, Dekkers CPM, Lam SK, et al.
GR122311X (ranitidine bismuth citrate), a new drug for the treatment of duodenal ulcer. Aliment Phar- macol Ther 1995;9:497-506.
25. Wyeth JW, Pounder RE, DeKoster E, et al.
GR122311X (ranitidine bismuth citrate) with anti-
biotics for the eradication of Helicobacter pylori.
Gastroenterology 1994;106(abstr):A212.
26. Ciociola AA, Koch KM, McSorley D, Smith JTL, Dewyer MA, Webb DD. Safety and pharmacokine- tics of chronic oral dosing of GR122311X (raniti- dine bismuth citrate), a new bismuth compound with anti-secretory activity. Gastroenterology 1992;
102(abstr): A50.
27. Ciociola AA, Koch KM, McSorley D, Snell CL, Webb DD. Safety and pharmacokinetics of ascen- ding oral doses of GR122311X (ranitidine bismuth citrate), a new bismuth compound with anti-secre- tory properties. Gastroenterology 1992;102(abstr):
A51.
28. McLren A, McDowell SR. GR122311X can signi- ficantly reduce the emergence of H. pylori strains resistant to antibiotics. Gut 1995;37(suppl 1):A62.
29. Wyeth JW, Pounder RE, Duggan AE, et al. Safety and efficacy of ranitidine bismuth citrate in com- bination with antibiotics for the eradication of Helicobacter pylori. Aliment Pharmacol Ther 1996;
10:623-630.
30. Pounder RE, Wyeth JW, Duggan AE, et al. Rani- tidine bismuth citrate with clarithromycin for the eradication of Helicobacter pylori and ulcer healing.
Helicobacter 1997;2:132-139.
31. McLaren A, McDowell SR, Bagshaw JA, McColm AA. The synergistic interaction between GR122311X and clarithromycin against Helicobacter. Am J Gastroenterol 1994;89(abstr):1382.
32. Go MF, Graham DY. Presence of the cagA gene in the majority of Helicobacter pylori strains is independent of whether the individual has duodenal ulcer or asymptomatic gastritis. Helicobacter 1996;
2:107-111.
33. Miehlke S, Kim JG, Small K, Kibler K, Graham DY, Go MF. Allelic variation in Helicobacter pylori cagA gene. Gastroenterology 1996;110(abstr):
A196.
34. Park SM, Park J, Kim JG, et al. Infection with Helicobacter pylori expressing cagA gene is not associated with an increased risk of developing
438 대한소화기학회지 : 제 35 권 제 4 호 2000
peptic ulcer diseases in Korean patients. Scand J Gastroenterol 1998;33:923-927.
35. Peterson WL, Graham DY, Barshall B, et al.
Clarithromycin as monotherapy for eradication of Helicobacter pylori: a randomized, double-blind trial. Am J Gastroenterol 1993;88:1860-1864.
36. Salcedo JA, Al-Kawas F. Treatment of Helicobac- ter pylori infection. Arch Intern Med 1998;158:
842-851.
37. Lind T, Veldhuyzen van Zanten SJOV, Ungew P, et al. The MACH 1 study: optimal one week treatment for H. pylori defined? Gut 1995;37(suppl
1):A15.
38. Laine L, Estrada R, Trujillo M, Fukanaga K, Neil Gl. Randomized comparison of 7, 10, and 14 days of omeprazole, amoxicillin, and clarythromycin for treatment of H. pylori. Gastroenterology 1996;
110(abstr):A168.
39. Logan RP, Bardhan KD, Celestin LR, et al.
Eradication of Helicobacter pylori and prevention of recurrence of duodenal ulcer: a randomized, double blind, multicenter trial of omeprazole with of without clarithromycin. Aliment Pharmacol Ther 1995;9:417-424.