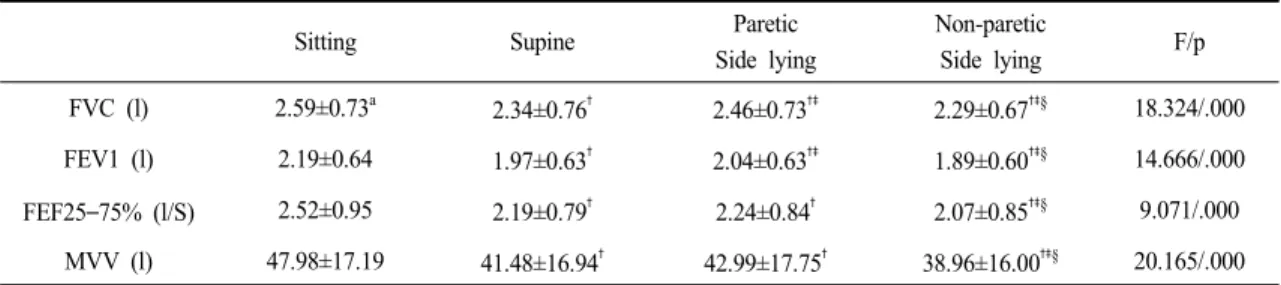
Pulmonary Function Index Comparisons Depending on Various Postures of Stroke Patients
10
0
0
전체 글
(3)
(4)
(5)
(7)
(10)
수치

관련 문서
Values of forced vital capacity, forced expiratory volume at one second, peak expiratory flow in pulmonary function tests were significant differences between
Conclusion: The total caloric intake of patients with chronic obstructive pulmonary disease showed a positive correlation with the diffusing capacity of the lung,
This study confirmed the changes in Maitland joint mobilization and diaphragmatic breathing exercises applied to the pulmonary function and chest circum- ference in patients with
The effects of trunk stabilization exercise on deep abdominal muscles thickness and pulmonary function in chronic stroke patient..
The Effects of Inspiratory Muscle Training with Chest Expansion on Pulmonary Function, Maximal Inspiratory Pressure, and Gait in Individuals with Stroke..
Conclusion : Robotic-assisted therapy in stroke patients have a positive impact on upper extremity function that could confirm that. In the future,
Values of forced vital capacity, forced expiratory volume at one second, peak expiratory flow in pulmonary function tests were significant differences between the
CONCLUSION : In this study, the experimental group showed greater improvement in pulmonary function than the control group, which indicates that the tredmill exercise is
