Comparison of Ferucarbotran-Enhanced MRI and Triple- Phase MDCT for the Detection of Hepatocellular
Carcinoma in Advanced Liver Cirrhosis
1Yong Hwan Jeon, M.D.1,2, Seung Hoon Kim, M.D., Dongil Choi, M.D., Min Ju Kim, M.D., Sam Soo Kim, M.D.2, Jiwon Lee, M.D.2, Heon Han, M.D.2, Jongmee Lee, M.D.3
1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine
2Department of Radiology, Kangwon National University College of Medicine
3Department of Radiology, Korea University Guro Hospital Received October 12, 2007 ; Accepted November 2, 2007
Address reprint requests to : Seung Hoon Kim, M.D., Department of Radiolgy, Samsung Medical Center, 50 Ilwon-dong, Kangnam-ku, Seoul 135-170, Korea
Tel. 82-2-3410-2542 Fax. 82-2-3410-2559 E-mail: [email protected]
Purpose: To compare the diagnostic performance of ferucarbotran-enhanced MRI at 1.5-T with triple-phase multidetector-row helical CT (MDCT) to detect hepatocellular carcinoma in patients with advanced liver cirrhosis.
Materials and Methods: Twenty patients with advanced liver cirrhosis (Child’s class B:C = 8:12) underwent ferucarbotran-enhanced MRI and triple-phase MDCT prior to liver transplantation. The mean time interval between the two imaging techniques was 18 days (range, 1-35 days). Three radiologists independently reviewed both im- ages on a lesion-by-lesion basis and interpreted them for comparison with the patho- logic findings of the explanted livers. As well, the sensitivity and an alternative-free re- sponse receiver operating characteristics (ROC) analysis was used to evaluate the diag- nostic performance of each technique.
Results: The mean area under the ROC curve (Az) was significantly higher for the triple-phase MDCT (0.766) compared to the ferucarbotran-enhanced MRI (0.675) (p <
0.001). Similarly, the mean sensitivity of the triple-phase MDCT (60.3%) exceeded the ferucarbotran-enhanced MRI (43.1%). The results indicate that the triple-phase MD- CT provides significantly greater mean sensitivity than the ferucarbotran-enhanced MRI (p < 0.001).
Conclusion: The triple-phase MDCT provided a better diagnostic performance and higher sensitivity than the ferucarbotran-enhanced MRI for the detection of hepatocel- lular carcinomas in patients with advanced liver cirrhosis.
Index words :Carcinoma, hepatocellular Liver cirrhosis
Magnetic resonance (MR) Tomography, spiral computed Ferumoxides
The current treatment of choice for patients with ad- vanced liver cirrhosis or unresectable hepatocellular carcinoma is a liver transplantation. Past studies have reported long-term survival in patients with a single he- patocellular carcinoma with diameters of 5 cm or less or a maximum of three tumors with diameters no more than 3 cm, having undergone a liver transplantation (1).
Consequently, an accurate surveillance of an unsuspect- ed hepatocellular carcinoma in transplantation candi- dates is vital for the diagnosis of hepatocellular carcino- ma, and to provide the appropriate treatment, thus pre- venting an ineffective transplantation (2, 3).
The multidectector-row helical CT (MDCT) is the most frequently used imaging modality to detect hepato- cellular carcinomas (4-6). Recently, the advent of the MDCT, which offers more rapid imaging, thinner slices, and better z-axis resolution, has improved the chances of detecting hepatocellular carcinoma (7-11).
Superparamagnetic iron oxide (SPIO) materials, such as ferumoxides, have been developed as liver-specific particulate magnetic resonance imaging (MRI) contrast agents. The uptake of SPIO occurs primarily in the Kupffer’s cells of the liver, resulting in decreased signal intensity for normal liver tissue because of the suscepti- bility effect of iron (12, 13). Some investigators have sug- gested that ferumoxide-enhanced MRI is more accurate than other imaging modalities, such as multiphase heli- cal CT or gadolinium-enhanced MRI, for the detection of hepatocellular carcinoma (14-17). Despite this, the authors of previous study have concluded that the de- tection of hepatocellular carcinoma in patients with liv- er cirrhosis on SPIO-enhanced MRI may be difficult be- cause of the reduced uptake of SPIO in the chronically injured liver parenchyma (18).
Another recently developed SPIO material, which has also been used in clinical practice, is ferucarbotran parti- cles coated with carboxydextran. The advantage of this material compared to ferumoxides is its practical use in dynamic studies requiring immediate performance fol- lowing a IV bolus injection (19, 20). It is however still unclear whether ferucarbotran-enhanced MRI can re- place contrast-enhanced MRI with an alternative SPIO material, such as ferumoxides.
The purpose of this study was in fact to compare the diagnostic performance of the ferucarbotran-enhanced MRI with the triple-phase MDCT for the detection of hepatocellular carcinomas in patients with advanced liv- er cirrhosis, against the pathologic findings of explanted livers as a standard.
Materials and Methods
Patients
The study population consisted of 118 consecutive pa- tients that underwent a liver transplantation for ad- vanced liver cirrhosis or radiologically proven hepato- cellular carcinoma in our institution between January 2003 and August 2004. Prior to transplantation, a triple- phase MDCT was performed on all 118 patients for the pre-transplantational surveillance of the liver. Of these patients, a ferucarbotran-enhanced MRI was performed on 25 of the 118 patients. Five of the 25 patients were excluded from our study: three patients were suspected of having hepatocellular carcinoma as well as having undergone a transarterial chemoembolization before transplantation and two patients had undergone a ra- diofrequency ablation for the same reason. In the end, a total of 20 patients (16 men and 4 women aged between 43 and 68 years; mean-52.4 years) were subjected to both imaging modalities. Each patient provided written informed consent and the study was approved by our hospital’s institutional review board.
The range of time intervals between the triple-phase MDCT and ferucarbotran-enhanced MRI was 1-35 days (mean, 18 days). Furthermore, the mean interval time between the last imaging study and the liver transplan- tation was 19 days (range, 1-56 days).
The pathologically proven diagnoses for all 20 patients were cirrhosis of the liver caused by viral hepatitis type B (n = 19), and viral hepatitis type C (n = 1). No cases of alcoholic cirrhosis were observed. Furthermore, the de- gree of liver cirrhosis was categorized according to the Child-Pugh classification. No patients were categorized under Child-Pugh classification A, eight patients were under classification B, and 12 were under classification C.
Triple-Phase MDCT and Ferucarbotran-Enhanced MRI The triple-phase MDCT imaging was performed with an MDCT scanner with four (n = 6), eight (n = 7) or 16 (n = 7) detectors (Lightspeed QX/I or Lightspeed Ultra 8 or Lightspeed 16; GE Healthcare, Milwaukee, USA).
The scanning parameters were 120 kVp, 175-184 mAs, 5 mm slice thickness, with a table speed of 15.0 mm/sec (pitch, 0.75) for the four detector MDCT, and 17.5 mm/sec (pitch, 0.875) for the eight detector MDCT, and 18.76 mm/sec (pitch, 0.938) for 16 detector MDCT dur- ing a single-breath-hold helical acquisition time of 8-10
seconds. The images were obtained in the craniocaudal orientation and were reconstructed every 5 mm to pro- vide contiguous sections. With the bolus-trigger tech- nique, the arterial scanning phase began 20-35 seconds after commencing the IV injection of 120 mL of nonion- ic iodinated contrast material (Iopamiro 300; Bracco, Milan, Italy) via an antecubital vein, at 4 mL/sec. The scanning portal phase began 70 seconds after commenc- ing of the contrast material injection. The delayed scan- ning phase began 180 seconds after the commencement of the contrast material injection.
An MRI was performed with 1.5-T units (Signa Horizon; GE Healthcare, Milwaukee, U.S.A.). All im- ages were obtained in the transverse plane using a phased-array multicoil as the receiver coil. For all pulse sequences, a 6- to 8-mm thick section with a 2 mm inter- section gap and a field of view ranging from 30-32 cm was used. The saturation bands that were superior and inferior to the imaging volume were applied in all se- quences to minimize the number of motion artifacts.
The ferucarbotran (ResovistⓇ; Schering, Berlin, Germany) dose was 1.4 mL for patients with body mass- es of 60 kg or more and 0.9 mL in patients with body masses below 60 kg (range, 8.0-12.0 μmol of iron/kg).
The contrast agent was manually administered intra- venously through an in-line 5-μm specific filter with a 1 sec bolus time, followed immediately by a 10 mL saline solution flush. The entire procedure was performed in approximately 5 sec. Prior to injecting of the contrast agent, a fat-suppressed respiratory-triggered fast spin- echo sequence with two echo times (proton density- weighted and T2-weighted images) (TR range/first-echo TE, second-echo TE range, 3,333-8,571/18, 90-117;
echo train length of 10-18; two signals acquired; 256×
256 matrix; bandwidth of 120 Hz per pixel), a T2*- weighted fast multi-planar gradient-recalled echo acqui- sition in the steady state (TR/TE range 130/8.4-10.4; flip angle, 30°; bandwidth, 60 Hz per pixel), and a breath- hold in phase, T1-weighted, fast multi-planar, spoiled gradient-recalled echo sequence (TR/TE, 200/4.2; flip angle, 90°; 256×160 matrix) were acquired. After the unenhanced images were taken, enhanced images of the same sequences were taken 10 minutes after inject- ing of the contrast agent. In addition, the dynamic en- hanced T1-weighted fast multi-planar spoiled gradient- recalled echo images were also obtained with delay times of 20 sec, 1 min, 3 min, and 5 min after injecting the contrast agent.
Image Analysis
The triple-phase MDCT images and ferucarbotran-en- hanced MR images were independently analyzed by three radiologists in random order in a blind study. In addition, the radiologists were informed that only the patients with liver cirrhosis were referred for a pre- transplantational assessment of hepatocellular carcino- ma. The time interval between the reviews of the MD- CT and MRI was at least 1 month and all images were evaluated using a 2,000×2,000 picture archiving and communication system (PACS) monitor, which allowed for adjustment of the optimal window setting in each case.
For each patient, the image review was conducted on a lesion-by-lesion basis for the entire liver. Each observ- er independently recorded the presence, size (maximum diameter), and location (Couinaud segment) of all le- sions, and stated whether the observer was able to de- termine the presence of a hepatocellular carcinoma based on a five-point confidence scale: 1- definitely not a tumor, 2- probably not a tumor, 3- a possible tumor, 4- a probable tumor, and 5- a definite tumor. To prevent the misallocation of the scored lesions for each imaging modality as well as those found during surgery, we used standardized markers (1- circular ROI, 2- a shorter linear line, 3- a longer linear line, 4- a shorter arrow, and 5- a longer arrow). The observer indicated the location of each lesion and at the time of the image review, the ob- servers were aware that the sensitivity was calculated using the number of lesions allocated at a confidence level of 3, 4 or 5.
For the triple-phase MDCT, a nodule showing the en- hancement and visualization of the intratumoral arteries during hepatic arterial phase, high, iso- or low attenua- tion on the portal venous phase and low attenuation on the delayed phase, and with or without capsular en- hancement, was regarded as hepatocellular carcinoma.
In addition, a nodule of mixed attenuation located at the hepatic arterial and portal venous phases displayed a low attenuation on the delayed phase. Moreover, a nod- ule size larger than 2 cm provided low attenuation on the portal venous and delayed phases, without definite enhancement on the arterial phase, and was similarly regarded as hepatocellular carcinoma (4, 6, 16).
For the ferucarbotran-enhanced MRI, any nodule seen as having high signal intensity or any prominent nodule with a diameter exceeding 2 cm despite the uptake of ferucarbotran was considered to be hepatocellular carci- noma. The high signal intensity lesions visible on a feru-
carbotran-enhanced MRI image other than hepatocellu- lar carcinoma, were diagnosed as hemangioma when they showed high signal intensity on unenhanced pro- ton density-weighted and T2-weighted MR images, and peripheral globular enhancement on ferucarbotran-en- hanced dynamic MR images. Moreover a cyst was con- firmed with typical imaging findings on unenhanced T1- and T2-weighted MR images with no enhancement of the ferucarbotran-enhanced images.
Lesion Confirmation
The explanted liver specimens were serially sectioned into 5-6 mm intervals at the transverse or coronal planes, depending on the anatomy of the liver and the location of the nodule. Any nodule with a diameter ex- ceeding 1 cm, or any bulging nodule different in color from the surrounding liver, regardless of size, was ex- amined under a microscope.
The pathologic examinations of the 20 explanted livers revealed 58 hepatocellular carcinomas in 17 patients.
The hepatocellular carcinomas ranged between 4 to 90 mm in diameter (mean, 16.7 mm). Moreover, of the 17 patients with hepatocellular carcinomas, six patients had one lesion, two had two lesions, one had three le- sions, one had four lesions, and seven had five or more
lesions.
All the lesions detected by a triple-phase MDCT or a ferucarbotran-enhanced MRI were compared with the corresponding lesions in the pathologic reports of ex- planted livers in relation to their location, size, and count. When a nodule of the triple-phase MDCT or feru- carbotran-enhanced MRI did not correlate with patho- logic findings, the pathologic reports were considered as the gold standard. The analysis of the observers’ inter- pretations was performed using the review of the com- bined MR and CT images and the pathologic reports by the study coordinator.
Statistical Analysis
Alternative-free response receiver operating character- istics (ROC) curves were generated by using a maxi- mum likelihood estimation program (ROCKIT 0.9B, Charles E. Metz) and calculated for each observer and imaging modality by plotting the true-positive fraction against the likelihood of obtaining a false-positive image at each confidence level (21). The diagnostic accuracy of each imaging modality and observer was determined by calculating the areas under each alternative-free re- sponse ROC curve (Az). The differences between imag- ing modalities, with respect to the mean Az values, were
Table 1. Az and p-values for Ferucarbotran-Enhanced MRI and Triple-Phase MDCT in Detection of Hepatocellular Carcinoma
Imaging Modality Observer 1 Observer 2 Observer 3 Mean
Ferucarbotran-enhanced MRI 0.681 ± 0.046 0.703 ± 0.045 0.641 ± 0.048 0.675 ± 0.027
Triple-phase MDCT 0.792 ± 0.041 0.789 ± 0.041 0.718 ± 0.048 0.766 ± 0.025
p < 0.001 0.021 0.044 < 0.001
Note ─ Azvalues (area under receiver operating characteristic curve) are expressed as the mean ± 1 standard deviation.
Table 2. Sensitivity of Ferucarbotran-Enhanced MRI and Triple-Phase MDCT for Diagnosis of 58 Hepatocellular Carcinomas
Imaging Modality Observer 1 Observer 2 Observer 3 Total
Ferucarbotran-enhanced MRI 39.7 (23/58) 48.2 (28/58) 41.4 (24/58) 43.1 (75/174)
Triple-phase MDCT 60.3 (35/58) 60.3 (35/58) 60.3 (35/58) 60.3 (105/174)
p < 0.001 0.039 0.001 < 0.001
Note ─ The values in parentheses represent the number of lesions assigned a score of 3, 4 or 5, divided by the total number of lesions (n
= 58) for pathologically proven hepatocellular carcinoma.
Table 3. Sensitivity of Ferucarbotran-Enhanced MRI and Triple-Phase MDCT in Detection of Hepatocellular Carcinoma according to Tumor Size
Tumor Total Number Observer 1 Observer 2 Observer 3 Total
Size (cm) of Tumors MRI CT MRI CT MRI CT MRI CT
≤ 1 19 1 (5) 06 (32) 02 (11) 06 (32) 1 (5) 06 (32) 4 (7) 18 (32)
≤ 2 28 12 (43) 18 (64) 15 (54) 18 (64) 12 (43) 18 (64) 39 (46) 54 (64)
Note ─ The values indicate the hepatocellular carcinoma counts, whereas the values in parentheses represent the percentages relative to the total number of observed tumors.
statistically analyzed using a two-tailed student’s t-test for paired data. A two-tailed p-value less than 0.05 was considered significant. The sensitivity of each imaging modality and each observer was determined by the number of lesions assigned at aconfidence level of ap- proximately 3, 4 or 5 of the 58 pathologically proven he- patocellular carcinomas. The difference in the sensitivi- ty between the MDCT and MRI was assessed with the McNemar test.
Kappa statistics were used to measure for the interob- server agreement in the detection of hepatocellular car- cinoma for each imaging modality. The degree of agree- ment was categorized as follows: Kappa values of 0.41- 0.60, moderate agreement; 0.61-0.80, good agreement;
and 0.81-1.00, excellent agreement. The statistical analyses were calculated using SPSS version 12.0 (Chicago, Illinois, U.S.A.).
Results
Overall, a total of 269 lesions were identified for both the imaging modalities by all three observers. For the 58 pathologically proven hepatocellular carcinomas, the calculated Az values of each observer and each imaging modality along the standard of reference was compared to the pathologic findings of explanted livers (Table 1).
The diagnostic accuracy of hepatocellular carcinoma was higher for all three observers with the triple-phase MDCT, as compared to the ferucarbotran-enhanced MRI. Moreover, the mean Az for MDCT (0.766) was sig- nifcantly greater than the Az for the MRI (0.675) (p <
0.001).
Hence, our data suggests that the sensitivity of the triple-phase MDCT was higher in the ferucarbotran-en- hanced MRI. In addition, the mean sensitivity of the
A B
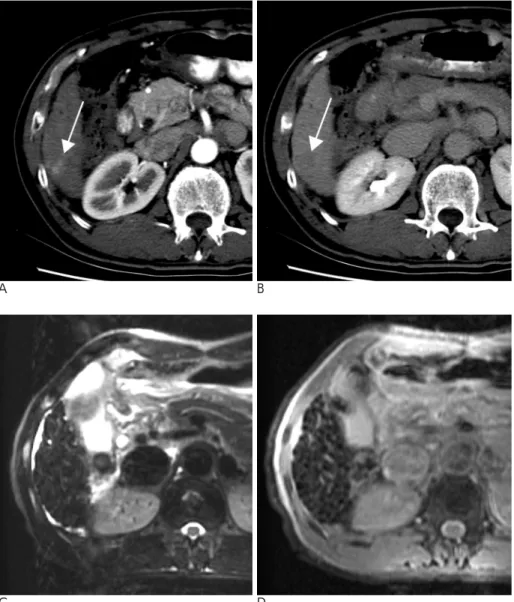
Fig. 1. A 60-year-old-man with a pathologically proven hepatocellular carcinoma in liver segment VI.
A. An arterial phase MDCT image shows an enhancing nodule (arrow).
B. A delayed phase MDCT image at the same level as A shows a low atten- uated nodule (arrow). All three ob- servers interpreted this nodule as he- patocellular carcinoma.
C, D. The ferucarbotran-enhanced MR images from fat-suppressed, respirato- ry-triggered T2-weighted fast spin- echo (C) and from T2*-weighted fast multi-planar gradient-recalled echo ac- quisition in steady state (D) reveal no high signal intensity nodule.
C D
triple-phase MDCT images (60.3%) was significantly greater than the ferucarbotran-enhanced MRI (43.1%) (p
< 0.001) (Table 2).
In the detection of hepatocellular carcinoma equal to or less than 1 cm, both imaging modalities showed low sensitivities (7% in MRI, 32% in MDCT) compared to the sensitivities observed for the larger hepatocellular carcinomas (Table 3). Despite this finding, all observers detected all of the 11 hepatocellular carcinomas greater than 2 cm in diameter for both imaging modalities.
Seven small (range, 6-13 mm; mean, 10.6) lesions which were not detected by all observers on the feru- carbotran-enhanced MRI were detected using the triple- phase MDCT for all observers (Fig. 1). However, two (8- and 14-mm) lesions were not detected by any of the ob- servers via the triple-phase MDCT, but were detected by the ferucarbotran-enhanced MRI by all observers (Fig. 2). A retrospective analysis revealed that five of the seven undetected lesions on the ferucarbotran-en- hanced MRI revealed a decreased signal intensity for
A B
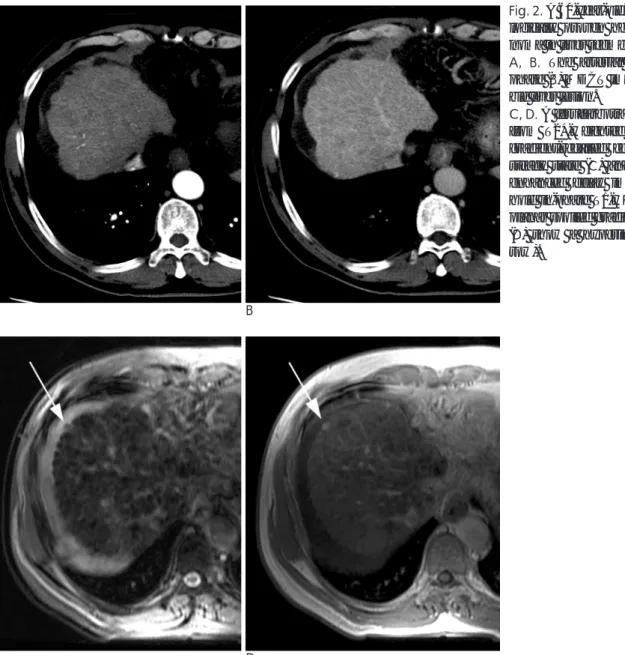
Fig. 2. A 60-year-old-man with a patho- logically proven hepatocellular carci- noma in liver segment VIII.
A, B. The arterial (A) and delayed phase (B) MDCT images show no visi- ble liver lesion.
C, D. A ferucarbotran-enhanced image from T2*-weighted fast multi-planar gradient-recalled echo acquisition in steady state (C) and a ferucarbotran- enhanced delay image from breath- hold in-phase T1-weighted fast multi- planar spoiled gradient-echo sequence (D) show a hyperintense nodule (ar- row).
C D
Table 4. Interobserver Agreement Regarding Presence of Hepatocellular Carcinoma
Imaging Technique Observer 1 vs. Observer 2 Observer 2 vs. Observer 3 Observer 1 vs. Observer 3
Ferucarbotran-enhanced MRI 0.759 0.626 0.674
Triple-phase MDCT 0.859 0.677 0.683
Note ─ Data are κvalues.
the ferucarbotran uptake, whereas, other lesions were misdiagnosed as vessels. A triple-phase MDCT resulted in two missed lesions by all observers, and showed no significant differences for the attenuation of surround- ing liver parenchyma, which was later substantiated up- on examining the explanted liver specimen.
The sum of all false-positive lesions (range, 4-24 mm;
mean, 11.2 mm) recorded by the triple-phase MDCT images was 39, as opposed to 27 (range, 5-20 mm;
mean 10.6 mm) for the ferucarbotran-enhanced MRI.
For the triple-phase MDCT, the major cause of false- positive lesions was an arterioportal shunt (Fig. 3). Due to the ferucarbotran-enhanced MRI, false positive re- sults were primarily due to misinterpretating the overly- ing vascular structures, such as branches of the hepatic or portal vein (Fig. 4).
The kappa values among the three observers showed good and excellent agreement for both imaging modali- ties (Table 4).
A B
Fig. 4. A 58-year-old man with a false- positive lesion on MRI.
A. A ferucarbotran-enhanced MR im- age from fat-suppressed, respiratory triggered T2-weighted fast spin-echo shows a subtle high signal intensity le- sion with an irregular margin (arrow).
Two of the three observers considered this lesion to be hepatocellular carci- noma.
B. The portal venous phase MDCT im- age shows a branch of segment VIII portal vein (arrow) at the same level as A.
A B
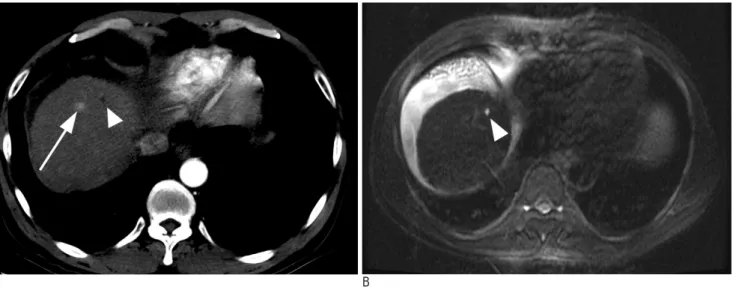
Fig. 3. A 48-year-old-woman with a false-positive lesion on MDCT.
A. An arterial phase MDCT image shows a small low density lesion (arrowhead) and another small enhancing nodule (arrow) in segment VIII. Two of the three observers considered the enhancing nodule to be hepatocellular carcinoma.
B. A ferucarbotran-enhanced image from fat-suppressed, respiratory triggered T2-weighted fast spin-echo MRI shows no visible nodule at the same level as A. A small high signal intensity lesion (arrowhead) in segment VIII was proven to be a hepatic cyst.
Discussion
Liver transplantations are widely accepted as an effec- tive therapeutic modality for a variety of irreversible acute and chronic liver diseases when no other satisfac- tory therapy is available. The selection of appropriate patients for transplantation is important because of high morbidity and mortality during and after surgery, and particularly following the shortage of donor livers. Thus, it is important to screen hepatocellular carcinomas to determine their eligibility for transplantation in liver transplant candidates.
Many investigators have compared the detection rates of hepatic tumors, particularly hepatocellular carcino- ma, using a variety of imaging modalities, such as CT during arterial portography (CTAP), contrast-enhanced CT, gadolinium-enhanced MRI, ferumoxide-enhanced MRI, and PET (13-17, 19, 22-30). Moreover, several investigators reported that ferumoxide-enhanced MRI appeared to be superior to CTAP and dual- or triple- phase helical CT to detect hepatocellular carcinoma (16, 22, 23). In addition, Reimer et al. reported that the feru- carbotran-enhanced MRI appeared to be superior to the dual- or triple-phase helical CT images for the detection of hepatic lesions (20).
In this study, the comparison of the triple-phase MD- CT and the ferucarbotran-enhanced MRI in the detec- tion of hepatocellular carcinomas was performed in pa- tients with advanced liver cirrhosis, rather than patients whose liver function was relatively good and able to en- dure surgery. In advanced or end-stage liver cirrhosis, the detection of hepatocellular carcinoma is difficult, be- cause the cirrhotic liver parenchyma contains fibrosis, regenerative nodules, fatty infiltration and parenchymal necrosis, as well as a variety of hemodynamic changes, such as collateral flow due to portal hypertension and a transient attenuation difference, including an arteriopor- tal shunt. Several investigators reported that the detec- tion rates of hepatocellular carcinomas for explanted liv- er pathology, with advanced or end-stage liver cirrhosis were 50-80% for contrast-enhanced CT and MRI (27- 29). Our results for each imaging modality for the detec- tion of hepatocellular carcinoma in advanced stages liv- er cirrhosis were consistent with these reports.
Kim et al. reported that the preoperative detection of hepatocellular carcinoma revealed a mean Az value for the triple-phase MDCT (0.949), which was slightly high- er than the observed Az value in the ferucarbotran-en-
hanced MRI (0.947); however, the difference was not statistically significant (30). Conversely, our study demonstrated that the diagnostic performance of the triple-phase MDCT (mean Az, 0.766) was significantly greater than the observed ferucarbotran-enhanced MRI (mean Az, 0.675). This conflicting finding may be due to our study population being skewed for patients with ad- vanced liver cirrhosis, whereas the Kim et al. study was primarily performed on patients with the ability to en- dure hepatic resection surgery.
In this study, both imaging modalities showed low sensitivities (7% for MRI, 32% for MDCT) for the detec- tion of hepatocellular carcinoma, equal to or less than 1 cm. Furthermore, the overall sensitivity of ferucarbo- tran-enhanced MRI (43.1%) was lower than that of triple-phase MDCT (60.3%). Several factors may con- tribute to the low sensitivity of ferucarbotran-enhanced MRI for detecting hepatocellular carcinoma. First, a well-differentiated hepatocellular carcinoma may result in the active uptake of ferucarbotran particles, which re- sults in iso- or hypointensity on ferucarbotran-enhanced images. Previous studies (16, 19) have pointed out that a variety of hepatic tumors, such as focal nodular hyper- plasia, regenerative nodule, hepatic adenoma, dysplastic nodule, and well-differentiated hepatocellular carcino- mas can display a variable uptake of SPIO, since these tumors contain a variable number of Kupffer’s cells.
Therefore, it may be difficult to distinguish well-differ- entiated hepatocellular carcinoma from other benign he- patic tumors. Second, advanced cirrhotic livers show poor liver enhancement due to decreased activity of Kupffer’s cells, which in turn affects the uptake SPIO particles. Furthermore, the poor liver enhancement is intensified by portal hypertension, which leads to SPIO redistribution to the spleen through increased uptake ac- tivity (31). Tang et al. reported a decrease in lesion de- tectability for ferumoxide-enhanced MRI images for Child-Pugh class C patients with severe portal hyperten- sion (25). Third, the reticular fibrosis and combined as- cites of advanced liver cirrhosis shows a high signal in- tensity, which can obscure small hepatocellular carcino- mas in certain situations.
Several factors may cause false-positive results.
Namely, it is possible that small hepatocellular carcino- mas could be difficult to differentiate from the presence of overlaying portal or hepatic veins in ferucarbotran- enhanced MRI images and the arterioportal shunt in triple-phase MDCT images. The high signal intensity of the overlaying vascular structures was the most fre-
quent cause of false-positive results for the ferucarbo- tran-enhanced MRI relative to the signal intensity of the liver parenchyma. On the other hand, MDCT images could distinguish peripheral hepatic vessels from small hepatocellular carcinomas because of a lower slice thickness and a higher MDCT resolution.
Small arterioportal shunts were commonly detected in MDCT images; however, were seldom observed in feru- carbotran-enhanced MRI. Small arterioportal shunts hardly influenced the change in the signal intensity for the ferucarbotran-enhanced MRI because they have lit- tle influence on the number of and activity level of Kupffer’s cells. Some nodules, such as regenerative or dysplastic nodules, as well as possibly hepatic adenoma may show a predominant hypoattenuation during portal venous or delayed phases for the contrast-enhanced CT images (6, 16), which may not be distinguished from hy- povascular hepatocellular carcinoma.
Ferucarbotran can be used to perform a dynamic study with a rapid IV bolus injection, which cannot be performed with ferumoxides. Reimer et al. reported that the ferucarbotran-enhanced dynamic study improved the differentiation of benign and malignant focal liver le- sions (19). In this study, the ferucarbotran-enhanced dy- namic study usually did not improve the detection of he- patocellular carcinoma itself, because of the low con- trast between the tumor and the surrounding cirrhotic liver. In addition, the different enhancement patterns of hepatocellular carcinomas for the cirrhosis of ferucarbo- tran-enhanced dynamic T1-weighted images were com- pared to those observed on gadolinium-enhanced dy- namic imaging (32). The benign lesions, such as heman- giomas or cysts can be diagnosed via dynamic studies.
Therefore, the ferucarbotran-enhanced dynamic study may be effective for the differentiation and characteriza- tion of benign and malignant hepatic tumors, rather than the detection of hepatocellular carcinomas in ad- vanced cirrhosis patients.
Despite the results of this study, several limitations should be taken into consideration. First, the sample size was relatively small. Second, a retrospective patho- logic correlation analyzed on a lesion-by-lesion analysis could not be performed because only the largest lesions were documented in detail for the pathologic reports of patients with four or more lesions. Nonetheless, an ob- jective assessment may be performed by determining the presence or absence of hepatocellular carcinomas via MDCT images or MRI without any information on the pathologic findings of the explanted livers and by
correlating on a one-to-one basis for each nodule for the MDCT or MR images with pathologic findings. Third, we selected 56 days as the longest time interval between the imaging study and transplantation because in screening the radiologic tests, including CT images or sonography, which were performed every 3 months at our institution. With this relatively long interval, could result in an underestimation of sensitivity due to incor- rect false-negative diagnoses of hepatocellular carcino- mas, because the shortest volume doubling time of a tu- mor is estimated to range between 27-41 days (33).
In summary, the triple-phase MDCT provided a better diagnostic performance and higher sensitivity than the ferucarbotran-enhanced MRI in the detection of HCC of patients with advanced liver cirrhosis. However, many false positive lesions resulting from nonspecific en- hancements, such as arterioportal shunts, could be the major cause for the detection of hepatocellular carcino- mas from triple-phase MDCT images.
Acknowledgements
This study was supported by the Samsung Medical Center Clinical Research Development Program grant and 2006 Research Grant from Kangwon National University.
References
1. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocel- lular carcinomas in patients with cirrhosis. N Engl J Med 1996;334:
693-699
2. Marsh JW, Dvorchik I, Subotin M, Balan V, Rakela J, Popechitelev EP, et al. The prediction of risk of recurrence and time to recur- rence of hepatocellular carcinoma after orthotopic liver transplan- tation: a pilot study. Hepatology 1997;26:444-450
3. Clavien PA. Orthotopic liver transplantation for stage III and stage IV hepatocellular carcinoma. Liver Transpl Surg 1997;3:S52-54 4. Baron RL, Oliver JH, Dodd GD, Nalesnik M, Holbert BL, Carr B.
Hepatocellular carcinoma: evaluation with biphasic, contrast-en- hanced, helical CT. Radiology 1996;199:505-511
5. Hollett MD, Jeffrey RB, Nino-Murcia M, Jorgensen MJ, Harris DP.
Dual-phase helical CT of the liver: value of arterial phase scans in the detection of small (< or = 1.5 cm) malignant hepatic neo- plasms. AJR Am J Roentgenol 1995;164:879-884
6. Jang HJ, Lim JH, Lee SJ, Park CK, Park HS, Do YS. Hepatocellular carcinoma: are combined CT during arterial portography and CT hepatic arteriography in addition to triple-phase helical CT all nec- essary for preoperative evaluation? Radiology 2000;215:373-380 7. Murakami T, Kim T, Takamura M, Hori M, Takahashi S, Federle
MP, et al. Hypervascular hepatocellular carcinoma: detection with double arterial phase multi-detector row helical CT. Radiology 2001;218:763-767
8. Kopp AF, Heuschmid M, Claussen CD. Multidetector helical CT of the liver for tumor detection and characterization. Eur Radiol
2002;12:745-752
9. Foley WD. Special focus session: multidetector CT: abdominal vis- ceral imaging. Radiographics 2002;22:701-719
10. Kawata S, Murakami T, Kim T, Hori M, Federle MP, Kumano S, et al. Multidetector CT: diagnostic impact of slice thickness on detec- tion of hypervascular hepatocellular carcinoma. AJR Am J Roentgenol 2002;179:61-66
11. Laghi A, Iannaccone R, Rossi P, Carbone I, Ferrari R, Mangiapane F, et al. Hepatocellular carcinoma: detection with triple-phase multi-detector row helical CT in patients with chronic hepatitis.
Radiology 2003;226:543-549
12. Weissleder R, Stark DD, Engelstad BL, Bacon BR, Compton CC, White DL, et al. Superparamagnetic iron oxide: pharmacokinetics and toxicity. AJR Am J Roentgenol 1989;152:167-173
13. Saini S, Stark DD, Hahn PF, Bousquet JC, Introcasso J, Wittenberg J, et al. Ferrite particles: a superparamagnetic MR contrast agent for enhanced detection of liver carcinoma. Radiology 1987;162:217- 222
14. Ward J, Naik KS, Guthrie JA, Wilson D, Robinson PJ. Hepatic le- sion detection: comparison of MR imaging after the administration of superparamagnetic iron oxide with dual-phase CT by using al- ternative-free response receiver operating characteristic analysis.
Radiology 1999;210:459-466
15. Bluemke DA, Paulson EK, Choti MA, DeSena S, Clavien PA.
Detection of hepatic lesions in candidates for surgery: comparison of ferumoxides-enhanced MR imaging and dual-phase helical CT.
AJR Am J Roentgenol 2000;175:1653-1658
16. Kang BK, Lim JH, Kim SH, Choi D, Lim HK, Lee WJ, et al.
Preoperative depiction of hepatocellular carcinoma: ferumoxides- enhanced MR imaging versus triple-phase helical CT. Radiology 2003;226:79-85
17. Vogl TJ, Hammerstingl R, Schwarz W, Mack MG, Mu¨ller PK, Pegios W, et al. Superparamagnetic iron oxide—enhanced versus gadolinium-enhanced MR imaging for differential diagnosis of fo- cal liver lesions. Radiology 1996;198:881-887
18. Elizondo G, Weissleder R, Stark DD, Guerra J, Garza J, Fretz CJ, et al. Hepatic cirrhosis and hepatitis: MR imaging enhanced with su- perparamagnetic iron oxide. Radiology 1990;174:797-801
19. Reimer P, Balzer T. Ferucarbotran (Resovist): a new clinically ap- proved RES-specific contrast agent for contrast-enhanced MRI of the liver: properties, clinical development, and applications. Eur Radiol 2003;13:1266-1276
20. Reimer P, Ja¨hnke N, Fiebich M, Schima W, Deckers F, Marx C, et al. Hepatic lesion detection and characterization: value of nonen- hanced MR imaging, superparamagnetic iron oxide-enhanced MR imaging, and spiral CT-ROC analysis. Radiology 2000;217:152-158 21. Metz CE. ROC methodology in radiologic imaging. Invest Radiol
1986;21:720-733
22. Choi D, Kim S, Lim J, Lee W, Jang H, Lee S, et al. Preoperative de-
tection of hepatocellular carcinoma: ferumoxides-enhanced MR imaging versus combined helical CT during arterial portography and CT hepatic arteriography. AJR Am J Roentgenol 2001;176:475- 482
23. Lee JM, Kim IH, Kwak HS, Youk JH, Han YM, Kim CS. Detection of small hypervascular hepatocellular carcinomas in cirrhotic pa- tients: comparison of superparamagnetic iron oxide-enhanced MR imaging with dual-phase spiral CT. Korean J Radiol 2003;4:1-8 24. Kim MJ, Kim JH, Chung JJ, Park MS, Lim JS, Oh YT. Focal hepatic
lesions: detection and characterization with combination gadolini- um- and superparamagnetic iron oxide-enhanced MR imaging.
Radiology 2003;228:719-726
25. Tang Y, Yamashita Y, Arakawa A, Namimoto T, Mitsuzaki K, Abe Y, et al. Detection of hepatocellular carcinoma arising in cirrhotic livers: comparison of gadolinium- and ferumoxides-enhanced MR imaging. AJR Am J Roentgenol 1999;172:1547-1554
26. Pauleit D, Textor J, Bachmann R, Conrad R, Flacke S, Layer G, et al. Hepatocellular carcinoma: detection with gadolinium- and feru- moxides-enhanced MR imaging of the liver. Radiology 2002;222:
73-80
27. Teefey SA, Hildeboldt CC, Dehdashti F, Siegel BA, Peters MG, Heiken JP, et al. Detection of primary hepatic malignancy in liver transplant candidates: prospective comparison of CT, MR imag- ing, US, and PET. Radiology 2003;226:533-542
28. Peterson MS, Baron RL, Marsh JW, Oliver JH, Confer SR, Hunt LE. Pretransplantation surveillance for possible hepatocellular car- cinoma in patients with cirrhosis: epidemiology and CT-based tu- mor detection rate in 430 cases with surgical pathologic correla- tion. Radiology 2000;217:743-749
29. Krinsky GA, Lee VS, Theise ND, Weinreb JC, Rofsky NM, Diflo T, et al. Hepatocellular carcinoma and dysplastic nodules in patients with cirrhosis: prospective diagnosis with MR imaging and explan- tation correlation. Radiology 2001;219:445-454
30. Kim SH, Choi D, Kim SH, Lim JH, Lee WJ, Kim MJ, et al.
Ferucarbotran-enhanced MRI versus triple-phase MDCT for the preoperative detection of hepatocellular carcinoma. AJR Am J Roentgenol 2005;184:1069-1076
31. Clement O, Frija G, Chambon C, Schouman-Clayes E, Mosnier JF, Poupon MF, et al. Liver tumors in cirrhosis: experimental study with SPIO-enhanced MR imaging. Radiology 1991;180:31-36 32. Lutz AM, Willmann JK, Goepfert K, Marincek B, Weishaupt D.
Hepatocellular carcinoma in cirrhosis: enhancement patterns at dynamic gadolinium- and superparamagnetic iron oxide-enhanced T1-weighted MR imaging. Radiology 2005;237:520-8
33. Barbara L, Benzi G, Gaiani S, Fusconi F, Zironi G, Siringo S, et al.
Natural history of small untreated hepatocellular carcinoma in cir- rhosis: a multivariate analysis of prognostic factors of tumor growth rate and patient survival. Hepatology 1992;16:132-137
대한영상의학회지 2008;58:53-63
진행성 간경변증에서 Ferucarbotran 조영증강 MRI와 삼중시기 MDCT의 간세포암 발견에 대한 비교 연구
11성균관대학교 의과대학 삼성서울병원 영상의학과
2강원대학교 의과대학 영상의학과
3고려대학교 구로병원 영상의학과
전용환1, 2・김승훈・최동일・김민주・김삼수2・이지원2・한 헌2・이종미3
목적: 진행성 간견병증 환자에서 1.5T ferucarbotran 조영증강 MRI와 삼중시기 MDCT의 간세포암 발견에 대한 진 단 정확도를 비교하고자 하였다.
대상과 방법: 진행성 간경변증 환자 20명(Child 분류 B:C=8:12)에서 간이식술 전에 ferucarbotran 조영증강 MRI 와 삼중시기 MDCT를 시행하였다. MRI와 MDCT 간의 시행 간격은 평균 18일(1-35일) 이었다. 3명의 영상의학 의가 ferucarbotran 조영증강 MRI와 MDCT에서 발견되는 각각의 모든 병변을 독립적으로 분석하였으며 이를 적 출된 간에서 발견된 병변의 병리학적 소견과 비교하였다. ROC 분석을 통해 MRI와 MDCT의 진단 정확도를 평가 하였으며 또한 각각의 민감도를 측정하였다.
결과: 삼중시기 MDCT의 ROC 곡선하 면적(Az = 0.766)이 ferucarbotran 조영증강 MRI의 ROC 곡선하 면적(Az
= 0.675)보다 컸으며 두 수치간에 통계적으로 유의한 차이가 있었다(p < 0.001). 간세포암 발견에 있어 삼중시기 MDCT와 ferucarbotran 조영증강 MRI의 민감도는 각각 60.3%와 43.1%였고 MDCT의 민감도는 ferucarbotran 조 영증강 MRI의 민감도 보다 유의하게 높았다(p < 0.001).
결론: 진행성 간경변증 환자에서 간세포암 발견에서 삼중시기 MDCT가 ferucarbotran 조영증강 MRI에 비해 더 좋 은 진단 정확도와 높은 민감도를 보인다.