□ 원 저 □
Vol. 14. No. 2, 2011
91
하복부 수술의 과거력이 있는 환자들에게 시행한 복강경 전복막외접근 탈장교정술의 초기 경험
경희대학교 의과대학 외과학교실, 1강동경희대학교병원 외과
조대현ㆍ김범수
1ㆍ최성일1ㆍ주선형1ㆍ이상목Laparoscopic Totally Extraperitoneal Hernia Repair in Patients with Previous Lower Abdominal Surgery-Early Experience
Dae Hyun Cho, M.D., Bum Soo Kim, M.D., Ph.D.
1, Sung Il Choi, M.D., Ph.D.1,Sung Hyung Joo, M.D., Ph.D.
1, Sang Mok Lee, M.D., Ph.D.Department of Surgery, Kyung Hee University School of Medicine at
1Gangdong Hospital, Seoul, Korea
Purpose: Recently, laparoscopic totally extraperitoneal (TEP)
inguinal hernia repair has established itself as a safe and effective treatment for inguinal hernia. Nevertheless, there are difficulties in learning the technique. In particular, patients with a medical history of having undergone lower abdominal surgery are generally excluded from laparoscopic hernia repair due to the technical difficulty of the procedure. This study evaluated the early surgical outcome and examined the feasibility of techniques for laparoscopic TEP inguinal hernia repair in patients who had previously undergone lower abdominal surgery.Methods: Ten cases of laparoscopic TEP inguinal hernia repair in patients with a prior history of lower abdominal surgery between November 2006 and January 2010 were reviewed. All cases were treated by a single highly experienced laparoscopic surgeon.
Results: Previous operations included 5 cases of radical prostatectomies for prostate cancer, 2 cases of open supra- pubic prostatectomies for benign prostate hypertrophy, 2 cases of radical cystectomies for bladder cancer and 1 case of laparoscopic low anterior resection for rectal cancer. In all 10 cases, the patients were male with 9 cases involving an
indirect hernia and 1 case involving a direct hernia. The mean operation time was 136.5±33.7 minutes, and in 1 case, the surgical method was converted to the transabdominal preperi- toneal approach. Postoperatively, there were 3 cases of urinary retention, and the administration of analgesics were required 1.0±0.6 times on average. The mean length of hospitalization was 1.2±0.8 days. During the mean 18 month (1∼36 months) follow-up period, there was no recurrence and chronic pain but 1 case of mesh infection was encountered 6 months after TEP repair.
Conclusion: Although the laparoscopic TEP inguinal hernia
repair can be carried out safely on patients with previous lower abdominal surgery, it needs to be carried out by fully trained surgeons with sufficient experience in the TEP technique.Nevertheless, more extensive experience and a longer follow-up period will be needed to evaluate the feasibility and efficiency of the TEP approach.
Key words: Laparoscopic surgery, Totally extraperitoneal,
Lower abdominal surgery, Inguinal hernia 중심단어: 복강경, 전복막접근, 하복부 수술, 서혜부 탈장※ 통신저자:이상목, 서울시 동대문구 경희대로 23 우편번호:130-702
경희대학교 의과대학 외과학교실 Tel:02-958-8241, Fax:02-966-9366 E-mail:[email protected]
서 론
탈장은 외과의가 접할 수 있는 가장 흔한 질환 중 하나이 며 수술적 교정을 위한 다양한 방법들이 개발되어 왔다.1 서 혜부 탈장의 수술법은 1887년 Bassini에 의해 high ligation과 posterior wall reconstruction을 원칙으로 하는 수술이 확립된 이후 1989년 Lichtenstein과 Shore가 polypropylene과 polye- thylene으로 만들어진 Marlex 그물막을 이용한 무긴장 탈장
교정술을 시행하고 우수한 결과를 발표하여 Bassini이후 가 장 획기적인 변화가 있었다.2,3 1990년 Ger 등4에 의해 개를 이용한 복강경 탈장복원술 실험 이후, 1992년 Arregui 등5이 시행한 경복강전복막(transabdominal preperitoneal, TAPP)접 근 탈장교정술과 1993년 McKernan과 Laws6가 시행한 전복 막외(total extraperitoneal, TEP)접근 복강경 탈장교정술을 보 편적으로 시행하고 있다.
복강경 탈장교정술의 장점으로는 수술 후 통증이 적고, 회복기간이 빨라 조기에 일상생활로의 복귀가 가능하며 한 번의 시술로 양측성 탈장을 교정할 수 있으며, 탈장낭의 최 고위 결찰이 가능하며, 미용상 좋다는 점을 들 수 있다.7,8 그러나 전신마취가 필요하며, 보고에 따라 그 결과는 다르 나 개복 탈장교정술에 비하여 수술비용, 수술 후 요저류의
발생률이 높게 보고되고 있다.9-11 또한 익숙하지 않은 복잡 한 서혜부의 해부학적 구조 때문에 수술 술기를 습득하는 데 어려움이 있고, 특히 하복부 수술의 과거력이 있는 환자 들의 경우에는 복직근(rectus abdominis muscle)의 근막과 복 막을 비롯해 서혜부의 복막외공간의 유착으로 인하여 전복 막외 접근 복강경 탈장교정술은 상대적 금기증으로 알려져
있다.12,13 그러나 하복부 수술의 과거력이 있는 서혜부 탈장
환자에서 복막외 접근법이 임상적으로 안전하고 유용한 접 근법이라는 보고도 있다.14 저자들은 전복막외 접근법으로 탈장교정술을 시행하는 과정에서 수술에 큰 어려움이 없었 던 충수절제술을 제외하고, 하복부 수술의 과거력이 있는 환자들에게서 시행한 전복막외 접근 복강경 탈장교정술의 초기 경험을 보고하고자 한다.
대상 및 방법 1) 대상
2006년 11월부터 2009년 12월까지 경희대학교병원 외과 에서 서혜부 탈장으로 진단하고, 전신마취가 가능한 모든 환자에게 시행한 전복막외 접근 복강경 탈장교정술 190예 중 충수절제술을 제외한 하복부 수술의 과거력이 있는 10 예(5.3%)를 대상으로 하여 임상양상, 수술시간, 수술 후 입 원기간, 진통제 투여량, 합병증 등을 후향적으로 조사하였 다. 충수절제술은 전복막외 접근법으로 수술하는데 큰 어 려움이 없어 대상에서 제외하였다. 수술은 1,000예 이상의 복강경 담낭절제술의 경험을 가진 한 명의 외과의가 시행 하였다.
2) 수술방법
환자는 전신마취를 하고 바로 누운 자세에서 배꼽의 직하 방에 종으로 15 mm정도의 피부절개를 하고, 복직근(rectus abdominis muscle)의 전초를 열고 근육과 후초 사이의 공간 에 검지를 삽입하여 골반부 쪽으로 중앙선을 따라 손가락이 완전히 들어갈 정도까지 충분히 박리한 다음 팽창풍선 (peritoneal distension balloon, Autosuture, Norwalk, USA)을 사 용하여 복막외 공간을 확보하였다. 하지만 유착으로 인하여 팽창풍선을 충분히 팽창시키기가 어려운 경우가 많아, 모니 터를 보면서 복막의 손상이 오지 않을 정도까지만 팽창시키 면서 풍선을 유착이 없는 쪽으로 외부에서 밀면서 최대한 팽창을 하였다. 팽창이 충분하게 되었다고 판단이 되면 팽 창풍선을 제거하고 10 mm 풍선투관침(balloon trocar, Auto- suture, Norwalk, USA)을 삽입하고 가스가 새지 않도록 풍선 에 공기를 25 cc 가량 넣은 후, CO2 가스를 12 mmHg까지 넣고 공간을 확보하였다. 카메라를 삽입한 후 화면을 보면 서 치골결합 직상방에 5 mm 투관침을 삽입하고 배꼽과 치 골상부 투관침의 중간 부위에 또 다른 5 mm 투관침을 삽입 하였다. 유착으로 인하여 치골결합 직상방에 투관침을 삽입
하기 힘든 경우 치골과 배꼽사이에 투관침을 먼저 삽입한 다음, 갈고리형의 전기소작기을 이용하여 중앙선을 조심스 럽게 박리하여 치골결합부까지 박리한 다음 투관침을 삽입 하였다. 유착으로 인하여 화면으로 어디까지 박리가 되었는 지 확인이 곤란한 경우에는 외부에서 치골을 손으로 만지면 서 위치를 확인하였다. 이후 비절개박리(blunt dissection)를 시행하여 내측으로는 중앙선과 치골결합부, 외측으로는 전 상장골극(anterior superior iliac spine), 아래쪽은 Cooper씨 인 대 아래쪽에서 요근(psoas muscle)까지, 앞쪽은 복직근이 충 분히 노출될 정도의 공간을 확보하였다. 이때에도 유착으로 인하여 복직근과 방광, 복막, 탈장낭, 정삭(spermatic cord)은 구분이 힘들고 해부학적 위치가 변하기 때문에 유착에도 위 치가 변하지 않는 Cooper씨 인대를 기준으로 주변의 구조물 들을 박리하였고, 내측에 유착이 심하면 유착이 심하지 않 은 외측에서 먼저 박리를 시행하여 충분한 공간을 확보하면 서 수술을 하였다. 탈장낭을 확인하고 정복한 후 폴리에스 터 메쉬(ParietexⓇ, Sofradim, Formans, France)를 사용하여 후 벽을 강화하였다. 수술 중 복막이 많이 찢어지면 클립이나 봉합사로 봉합하였고 심하게 찢어진 1예에서는 경복강전복 막 접근법으로 전환하였고, 정관이나 혈관이 복막과 유착이 심하여 복막과 분리가 되지 않는 경우에는 복막을 정관이나 혈관에 일부 남기고 복막을 박리하고 찢어진 복막은 봉합하 였으며 복막의 상태를 확인하기 위해서 복강 내에 카메라를 삽입한 경우도 2예 있었다. 탈장낭은 전 예에서 정복하였으 며 직접탈장의 경우 탈장낭을 정복한 후 복횡근막(trans- versalis fascia)을 Cooper씨 인대에 TackerⓇ (Autosuture, Nor- walk, USA)로 고정하였다. 메쉬는 전 예에서 외측 전복벽에 1개, Cooper씨 인대에 2개를 TackerⓇ를 사용한 Tack으로 고 정하였다. 메쉬를 고정한 후 CO2 가스를 차단하고, 치골 상 부의 투관침을 통하여 가스를 천천히 방출시키면서 메쉬가 제대로 펼쳐진 상태가 유지되는 것을 확인하면서 수술을 마 쳤다.
결 과
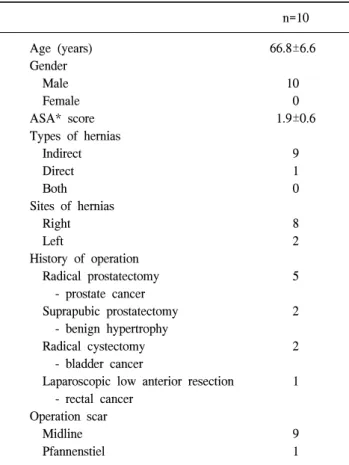
환자는 10명, 모두 남자였으며 평균나이는 66.8세였다. 간 접탈장이 9예, 직접탈장이 1예였고 우측이 8예, 좌측이 2예 였다. 수술의 종류는 전립선암으로 근치적 전립선절제술 5 예, 전립선 비대증으로 개복 전립선절제술 2예, 방광암으로 근치적 방광절제술 2예, 직장암으로 복강경 저위전방절제 술(laparoscopic low anterior resection) 1예 였고, Pfannenstiel 반흔이 있는 직장 암 1예를 제외한 9예가 하부 정중선의 수 술 반흔이 있었다(Table 1). 전립선암 5예 중 1예는 복강경 로봇수술을 시행하다 개복수술로 전환한 경우였고 방광암 2예 중 1예는 근치적 절제술 후 방사선 치료를 받았다.
수술시간은 136.5±33.7분, 수술 후 진통제는 1.0±0.6회 투 여 받았고 입원기간은 1.2±0.8일이였다. 1예에서 수술 중 심
Table 1. Clinical characteristics of laparoscopic totally expraperi-
toneal inguinal hernia repair in patients who had undergone previous lower abdominal surgeryn=10 Age (years)
Gender Male Female ASA* score Types of hernias Indirect Direct Both Sites of hernias Right Left
History of operation Radical prostatectomy - prostate cancer Suprapubic prostatectomy - benign hypertrophy Radical cystectomy - bladder cancer
Laparoscopic low anterior resection - rectal cancer
Operation scar Midline Pfannenstiel
66.8±6.6 10
0 1.9±0.6
9 1 0 8 2 5 2 2 1
9 1
*ASA = American Society of Anesthesiologists.
Table 2. Clinical results of laparoscopic totally expraperitoneal
inguinal hernia repair in patients who had undergone previous lower abdominal surgeryn=10 Operation time (minutes)
Postoperative stay (days) Analgesic
Conversion to TAPP* repair Urinary retention
Mean follow up (months) Mesh infection Chronic pain Recurrence
136.5±33.7 1.2±0.8 1.0±0.6
1 3 18 (1∼36)
1† 0 0
*TAPP = transabdominal preperitoneal; †6 months after hernia repair in patient with previous radical cystectomy.
한 복막파열로 경복강전복막 접근법으로 전환하였으며, 3 예에서 당일 배뇨곤란이 있었지만 특별한 치료 없이 다음 날 호전이 되었고, 평균 18개월(1∼36개월)의 추적기간 중 만성 통증이나 재발은 없었지만 1예에서 메쉬 감염이 있었 다(Table 2). 메쉬 감염이 있었던 1예는 방광암으로 근치적 방광절제술을 시행하고 회장루를 가진 환자로 수술 후 6개 월째 감염이 발생하여 18개월째 메쉬를 제거하였다.
고 찰
서혜부탈장 교정술은 외과의들이 접할 수 있는 가장 흔 한 수술 중 하나로 매년 미국에서 70만 명이 수술을 받고 있다.15
탈장교정술은 역사에 따라 진화를 거듭해왔으며 최근 복 강경수술이 외과에 도입되면서 복강경 탈장교정술도 통증 의 감소와 창상 크기의 감소, 사회로의 빠른 복귀 등의 장점 으로 인하여 보편화되고 있는 추세이다.16-20 국내의 경우 복 강경 탈장교정술은 1990년대 중반부터 시행하였지만 복강 경 수술에 대한 의료보험 급여가 되지 않아 보편화되지 못
하고 있었다. 하지만 2006년 6월부터 복강경 수술에 대한 의료보험 급여가 시작되었고 이를 계기로 복강경 탈장교정 술을 활발히 시행할 수 있는 계기가 되었다.
서혜탈장의 원인에는 여러 인자가 알려져 있지만 복부수 술의 기왕력은 탈장을 유발하는 인자의 하나로 알려져 있 다. 충수절제술만 받았다 할지라도 복벽을 약화시켜 탈장 을 유발한다는 보고가 있다.21 서혜탈장을 유발하는 가장 대 표적으로 복부수술로는 근치적 전립선절제술이 있는데, Regan 등22은 수술 후 6개월 내 서혜탈장이 잘 발생하고, Lodding 등23은 수술 후 2년 안에 서혜탈장이 잘 발생한다고 하였다. 저자들의 경우에서도 전립선절제술을 시행한 경우 가 7예(70%)로 가장 많았다. 복부수술 특히 전립선절제술 이 탈장을 유발하게 되는 원인은 복횡근막의 셔터 기전에 장애가 생겨서 myopectineal orifice에 결함이 생기기 때문이 라고 알려져 있다.24 통계적 자료에 기반을 두진 않았지만 많은 외과의사들이 하복부 수술의 기왕력, 특히 전립선 절 제술을 받은 환자들에게 있어 전복막외 접근 복강경 탈장 교정술은 수술 후 유착으로 인하여 금기시되었고 상대적으 로 고식적인 무긴장 탈장교정술이나 경복강전복막(TAPP) 접근 술식을 선호해왔다.25 Paterson 등14은 하복부 수술을 받은 환자라 할지라도 전복막외 접근 복강경 탈장교정술을 충분히 익힌(fully trained) 외과의사라면 시도할만한 수술방 법이라고 하였다. 이에 저자들도 하복부 수술을 받은 환자 들에게도 전복막외 접근 복강경 탈장교정술을 시행하게 되 었다. 저자들의 경우 충수절제술이 전복막외 접근 복강경 탈장교정술에 미치는 영향이 거의 없어서 충수절제술을 제 외한 하복부 수술의 경력이 있는 환자들을 대상으로 연구 를 계획하였다.
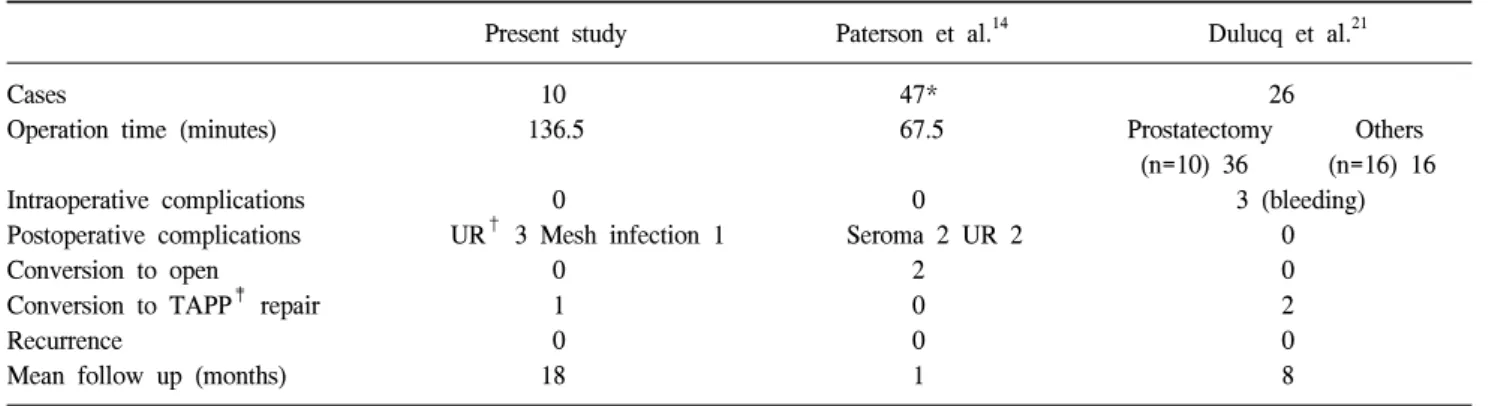
수술 후 합병증으로 Paterson 등14은 20예의 충수절제술을 포함하는 47예의 보고에서 36%에 해당하는 17예에서 이전 수술로 인한 유착으로 수술에 어려움을 겪었지만 경미한
Table 3. Comparison of the results about laparoscopic totally extraperitoneal inguinal hernia repair in patients with previous lower
abdominal surgeryPresent study Paterson et al.14 Dulucq et al.21 Cases
Operation time (minutes) Intraoperative complications Postoperative complications Conversion to open Conversion to TAPP‡ repair Recurrence
Mean follow up (months)
10 136.5
0
UR† 3 Mesh infection 1 0
1 0 18
47*
67.5 0 Seroma 2 UR 2
2 0 0 1
26
Prostatectomy Others (n=10) 36 (n=16) 16
3 (bleeding) 0 0 2 0 8
*20 cases of appendectomy was included; †UR = urinary retention; ‡TAPP = transabdominal preperitoneal.
장액종, 요저류를 각 2예 보고하였고, 수술 중 합병증은 없 었으며 2예에서 개복 무긴장 탈장 교정술로 전환하였다.
Dulucq 등21은 전립선절제술 후 발생한 서혜부 탈장 10예와 충수돌기절제술, 자궁절제술, 대동맥우회술 등 기타 복부 수술 기왕력이 있는 환자 16예, 수술의 기왕력이 없는 환자 124예를 비교 분석하여 수술력이 있는 환자 중 3예에서 수 술 중 출혈을, 2예에서의 경복강전복막 접근법으로의 전환 했음을 보고하였다. 두 연구 모두 각각 30일과 8개월의 평 균 추적 관찰 기간 중 재발한 사례는 없었다. 저자들의 경우 합병증으로 수술 당일 배뇨곤란 3예, 메쉬 감염 1예가 있었 고, 경복강전복막 접근법으로 전환한 경우도 1예 있었다.
메쉬 감염이 생긴 1예는 방광암으로 수술 받고 회장루를 가진 환자로 탈장교정술 후 6개월 째 감염이 발생하여 보존 적 치료에 실패하여 수술 18개월 째 메쉬를 제거하였다. 평 균 수술시간은 저자들의 경우 136.5분으로 66.1∼87.1분으 로 보고한 다른 보고에 비하여 길었다.26 Paterson 등14은 수 술의 경력이 있는 경우 67.5분, Dulucq 등21은 과거 수술이 근치적 전립선절제술인 경우 38분, 기타 다른 수술인 경우 16분, 수술의 경력이 없는 경우 15.8분이라고 보고하였다 (Table 3). 전복막외 접근 복강경 탈장교정술의 수술 합병증 으로는 창상감염, 혈종, 요저류, 고환부종 등이 알려져 있 다.9-11 Osama 등27은 108예 중에서 17예의 하복부 수술을 받 은 자를 그렇지 않은 자와 비교한 후향적 연구에서 수술 후 합병증 발생에 유의한 차이가 없음을 보고하였고, Tetik 등28은 서혜부 탈장의 복강경 수술에 관한 합병증과 재발율 에 대해 기술한 다기관 후향 연구에서 복강경 전복막외 접 근 복강경 탈장교정술 후 혈종, 장액종, 피하기종 등의 구역 합병증이 가장 많고 다음으로 신경학적 합병증을 보고하 고, 23예의 요저류와 6예의 메쉬감염을 보고하였는데 후자 는 경복강전복막 접근법에 더 흔하다고 하였으며 총 2.2%
의 재발율을 기술하였다. Duluk 등29은 15년 동안 시행한 3,100예의 복강경 탈장교정술에서 0.21% (5예)의 신경통과 0.46% (11예)의 재발율을 보고하였다. 이 연구에서도 혈종
과 장액종이 2.1% (50예)로 가장 많은 합병증이었으며 1예 의 메쉬 감염을 보고하였다.
결 론
저자들은 충수절제술을 제외한 하복부 수술의 과거력이 있는 환자 10예에서 전복막 외 접근 복강경 탈장교정술을 성공적으로 시행하였다. 그러나 복강경 수술에 충분한 경 험을 가진 외과의사가 시행하였음에도 불구하고 대부분에 서 심한 유착으로 인하여 수술에 어려움이 있었고 긴 수술 시간이 필요하였다.
서혜부 탈장으로 진단된 개복 전립선절제술이나 근치적 방광절제술 등 골반 내에서 시행되는 수술의 과거력을 가 진 환자들을 대상으로 시행하는 전복막외 접근 복강경 탈 장교정술의 안전성과 유효성은 저자들의 증례 수가 많지 않고 추적기간이 짧아, 향후 많은 경험과 장기적인 추적관 찰이 필요할 것으로 생각된다.
참고문헌
1) Nyhus L, Condon R. Hernia. 4th ed. Philadelphia: JB Lippin- cott; 1995.
2) Bassini E. Nuovo Metodo Sulla Cura Radicale dell’ Ernia Inguinale Arch Soc Ital Chir 1887;4:380.
3) Lichtenstein I, Shore J. Simplified repair of femoral and recurrent inguinal hernias by a “plug” technic. Am J Surg 1974;128:439-444.
4) Ger R, Monroe K, Duvivier R, Mishrick A. Management of indirect hernias by laparoscopic closure of the neck of the sac.
Am J Surg 1990;159:370-373.
5) Arregui M, Davis C, Yucel O, Nagan R. Laparoscopic mesh repair of inguinal hernia using a preperitoneal approach: a preliminary report. Surg Laparosc Endosc 1992;2:53-58.
6) McKernan J, Laws H. Laparoscopic repair of inguinal hernias
using a totally extraperitoneal prosthetic approach. Surg Endosc 1993;7:26-28.
7) Kumar S, Wilson R, Nixon S, Macintyre I. Chronic pain after laparoscopic and open mesh repair of groin hernia. Br J Surg 2002;89:1476-1479.
8) Memon M, Cooper N, Memon B, Memon M, Abrams K.
Meta-analysis of randomized clinical trials comparing open and laparoscopic inguinal hernia repair. Br J Surg 2003;90:
1479-1492.
9) Koch A, Grinberg G, Farley D. Incidence and risk factors for urinary retention after endoscopic hernia repair. Am J Surg 2006;191:381-385.
10) Winslow E, Quasebarth M, Brunt L. Perioperative outcomes and complications of open vs laparoscopic extraperitoneal inguinal hernia repair in a mature surgical practice. Surg Endosc 2004;18:221-227.
11) Bollaboration E. Laparoscopic compared with open methods of groin hernia repair: systemic review of randomized controlled trials. Br J Surg 2000;87:860-867.
12) Andersson B, Hallen M, Leveau P, Bergenfelz A, Westerdahl J. Laparoscopic extraperitoneal inguinal hernia repair versus open mesh repair: a prospective randomized controlled trial.
Surgery 2003;133:464-472.
13) Bringman S, Ramel S, Heikkinen T, Englund T, Westman B, Anderberg B. Tension-free inguinal hernia repair: TEP versus mesh-plug versus Lichtenstein: a prospective randomized cont- rolled trial. Ann Surg 2003;237:142-147.
14) Paterson H, Casey J, Nixon S. Totally extraperitoneal laparoscopic hernia repair in patients with previous lower abdominal surgery. Hernia 2005;3:228-230.
15) Rutkow I. Epidemiology, economic and sociologic aspects of hernia surgery in the United States in the 1990s. Surg Clin North Am 1998;73:413-426.
16) Heikkinen T, Haukipuro K, Koivukangas P, Hulkko A, A prospective randomized outcome and cost comparison of totally extra-peritoneal endoscopic hernioplasty versus Lichtenstein operation among employed patients. Surg Laparosc Endosc 1998;8:338-344.
17) Lal P, Kajla R, Chander J, Saha R, Ramteke V. Randomised controlled study of total extra-peritoneal versus open Lichten- stein inguinal hernia repair. Surg Endosc 2003;17:850-856.
18) McCloud J, Evans D. Day-case laparoscopic hernia repairin a single unit. Surg Endosc 2003;17:491-493.
19) Ferzli G, Sayad P, Vasisht B. The feasibility of laparoscopic extraperitoneal hernia repair under local anesthesia. Surg Endosc 1999;13:588-590.
20) Ferzli G, Massaad A, Dysarz F, Kopatsis A. A study of 101 patients treated with extraperitoneal endoscopic laparoscopic herniorrhaphy. Am Surg 1993;59:707-708.
21) Dulucq J, Wintringer P, Mahajna A. Totally extraperitoneal (TEP) hernia repair after radical prostatectomy or previous lower abdominal surgery Is it safe? A prospective study. Surg Endosc 2006;20:473-476.
22) Regan T, Mordkin M, Constantinople N, Spence J, Dejter S.
Incidence of inguinal hernias following radical retropubic prostatectomy. Urology 1996;47:536-537.
23) Lodding P, Bergdahl C, Nyberg M, Pileblad E, Stranne J, Hugosson J. Inguinal hernia repair after retropubic prosta- tectomy for prostate cancer: a study of incidence and risk factors in comparison to no operation and lymphadenectomy.
J Urology 2001;166:964-967.
24) Shpitz B, Lansberg L, Bugayer N, Tiomkin V, Klein E.
Should peritoneal tears be routinely closed during laparoscopic total extraperitoneal repair of inguinal hernias? A reappraisal.
Surg Endosc 2004;18:1771-1773.
25) Palanivelu C. Operative manual of laparoscopic hernia surgery. 1st ed. GEM Foundation: Coimbatore, India; 2004;
99-117.
26) Ramshaw B, Shuler F, Jones T, White D, Wilson R, Lucas G, et al. Laparoscopic inguinal hernia repair-lessons learned after 1224 consecutive cases. Surg Endosc 2001:15:50-54.
27) Osama A, Dhafir A, Muhammad Z, Cunningham F, Josepph P. Totally extraperitoneal laparoscopic inguinal hernia repair is a safe option in patients with previous lower abdominal surgery. J Laparoendosc Adv Surg Tech 2008;18:352-357.
28) Tetik C, Arregui M, Dulucq J, Fitzgibbons R, Franklin M, McKernan J, et al. Complications and recurrences associated with laparoscopic repair of groin hernias- A multi-instituinal retrospective analysis. Surg Endosc 1994;8:1316-1323.
29) Duluck J, Wintringer P, Mahajna A. Laparoscopic totally extraperitoneal inguinal hernia repair: lessons learned from 3,100 hernia repairs over 15 years. Surg Endosc 2009;23:482-486.