Comparison of Inguinal Hernia in both Sexes and Laparoscopic Surgery for Female Patients
5
0
0
전체 글
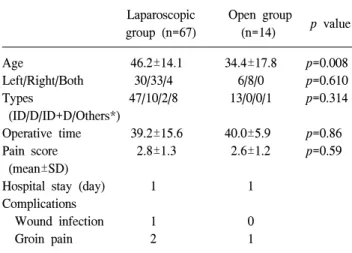
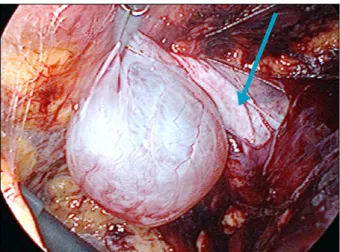
(2) 12 Journal of Minimally Invasive Surgery Vol. 15. No. 1, 2012 은 SPSS 18.0 (SPSS Inc., Chicago, IL)을 이용하여 independent t-test 및 교차분석을 통한 Chi-square test로 하였으 며, p<0.05인 경우 유의성을 두었다. 수술방법: 복강경 수술 환자 중 과거 자궁적출술을 시행받 은 1예는 경복강 복막전층 탈장교정술(TAPP, Transabdominal Preperitoneal Hernioplasty)을 시행받았고, 그 외 다 른 모든 환자들은 전복막접근하 탈장수술(TEP, Totally Ex14 traperitoneal Preperitoneal Hernioplasty)을 받았다. 절개수술 14예 중 4예는 고위결찰술, 10예는 인공막을 이용한 무긴장 탈장수술을 받았다. TEP시술은 원인대로부터 탈장낭을 분 리한 후 인공막을 반 절개하여 원인대하방으로 넣어서 내 서혜륜(internal ring)을 막고 절개한 인공막을 봉합하거나, 원인대와 탈장낭을 원위부에서 자른 후 인공막을 부착하고 원인대를 내서혜륜 근처에 고정하였다(Fig. 1, 2).. 결. 과. 전체 대상환자 965명중 여자는 81명(8.4%)였다. 여자환자 의 평균 연령은 남자보다 적었으며, 양측탈장(남 vs. 여, 12.7 vs. 4.9%, p=0.047) 및 직접탈장의 빈도(24.5 vs. 12.3%, p=0.024)는 남자에서 많았고, 대퇴탈장은 여자에서 많았다 (8.6%/0.6%, p<0.001). 좌 우측 및 간접탈장의 빈도는 남녀 간 차이가 없었다(Table 1). 81예의 여자 환자 중 복강경수 술을 받았던 환자의 평균연령이 더 많았다. 또한 대퇴탈장 환자의 평균연령이 다른 형태의 탈장환자 나이보다 많았다 (56.4±12.5/43.0±15.1 p<0.026). 수술시간 및 수술 후 7일째 통증의 정도는 복강경 및 절개군간 차이가 없었다(Table 2).. Table 1. Demographic feature and hernia location and types of the female and male hernia Female (n=81) Age (mean, range) 44.2 (20∼79) Location (%) Right 41 (50.6) Left 36 (44.4) Bilateral 4 (4.9) Types Indirect (ID) 60 (74.1) Direct (D) 10 (12.3) ID+D 2 (2.5) Femoral 7 (8.6) Others* 2 Fig. 1. Hernia sac (green arrow) was located in anterior side of the round ligament (blue arrow).. Male (n=884). p value. 55.4 (20∼90) p<0.001 460 (52.0) 312 (35.3) 112 (12.7) 614 217 29 5 19. (69.5) (24.5) (3.3) (0.6). p=0.818 p=0.116 p=0.047 p=0.449 p=0.024 p=0.658 p<0.001. *Obturator hernia, ID+femoral, D+femoral, ID+obturator.. Table 2. Demographic feature, hernia anatomy and postoperative course of the laparoscopic and open groups Laparoscopic group (n=67). Fig. 2. Intraoperative finding of applied mesh encircling the round ligament (arrow).. Age 46.2±14.1 Left/Right/Both 30/33/4 Types 47/10/2/8 (ID/D/ID+D/Others*) Operative time 39.2±15.6 Pain score 2.8±1.3 (mean±SD) Hospital stay (day) 1 Complications Wound infection 1 Groin pain 2. Open group (n=14). p value. 34.4±17.8 6/8/0 13/0/0/1. p=0.008 p=0.610 p=0.314. 40.0±5.9 2.6±1.2. p=0.86 p=0.59. *Obturator hernia, ID+femoral, D+femoral.. 1 0 1.
(3) Choon Sik Chung et al.: Comparison of Inguinal Hernia in both Sexes. Fig. 3. Round ligament cyst just lateral to opened sac (arrow) of hernia. 81예중 9예(11.1%)에서 자궁 원인대 낭종이 발견되었고 (Fig. 3), 6예는 좌측, 3예는 우측으로 좌측에서 그 빈도가 높았으나 통계적 유의성은 없었다(p=0.33). 탈장수술과 더 불어 5예은 낭종절제술, 4예은 절개 개방술(lay open)을 시 행받았다. 낭종의 크기는 2∼7 cm으로 다양하였으며, 낭종 을 절제한 5예의 조직검사 결과는 epithelial cyst (2예), inclusion cyst (2예), endometrial cyst (1예)이었다. 모든 환자는 수술 다음날 퇴원하였으며, 수술에 따른 합병증으로 복강 경 환자에서 창상감염 1예, 3개월 이상 간헐적 서혜부 통증 2예였고 절개수술환자에서는 간헐적 통증 1예 외 없었다. 평균추적기간 25개월(7∼50개월) 현재 재발된 예는 없다.. 고. 찰. 여자는 남자에 비하여 상대적으로 복횡근(transverse abdominal muscle)과 복횡근 건막(transversalis fascia)이 발달 되었고, 복횡근 건막궁(transversus abdominis aponeurosis arch)이 쿠퍼씨 인대(Cooper’s ligament)에 넓게 부착되어 직 5,11,15 본 연구 접탈장의 빈도가 낮은 것으로 알려져 있으며, 에서도 남자에 비해 유의하게 낮은 빈도를 보였다. 양측탈 장은 간접탈장보다 직접탈장이 많고, 그 빈도는 3.7∼10% 11,16,17 여자에서 직접탈장의 빈도가 낮아 양측 탈 정도이다. 장이 적으며, 본 연구에서도 4.9%로 남자들에 비해 그 빈도 가 낮았다. 본 연구에서 여자환자의 대퇴탈장 빈도는 7.8% 3,5,7,11 상대적으로 로 남자에 비해 높으나, 다른 연구에 비해 낮은 것은 대퇴탈장이 비교적 고령의 연령에서 좀 더 많이 발생하고, 감돈에 의한 장폐색으로 응급실을 통하여 입원 하는 경우가 많아, 응급실이 없는 본원 사정상 상대적으로 그 빈도가 낮은 것으로 생각되며, 전체 여자 환자 중 한 명 만 대퇴탈장 감돈으로 응급수술을 받았다. 복강경 서혜부탈장수술은 기존의 절개방식에 비해 통증. 13. 이 적고 일상생활로 복귀가 빠른 장점이 있으나,8-10 기존의 절개방식에 비하여 장 혹은 방광손상과 같은 심각한 합병 18-20 인공막을 이용한 절개수술과 증의 가능성은 더 높으며, 21,22 복강경 탈장 재발율은 큰 차이가 없다는 보고들도 있다. 수술은 복강내 접근법에 의한 탈장수술법(TAPP, IPOM)과 복막외 접근법이 있다. 복강내 접근법은 추가적인 시술 없 이 반대편을 확인할 수 있는 장점은 있으나, 수술 중 복강내 장기의 손상, 복막을 열었다가 다시 닫아야 하는 부담감, 수 술 후 장유착과 같은 합병증이 발생할 수 있다. 복막외 접근 법은 이러한 합병증은 없으나 해부학적 구조물이 복잡하고 반대편 탈장이 있는지 확인하기 위해 추가적인 시술이 필 요하며 좁은 공간에서 수술을 하므로 익숙해지는데 시간에 23-25 본 연구의 복강경 수술군에서 과거 하복부 더 소요된다. 절개 반흔으로 인해 복강내 접근법(TAPP)으로 수술받은 1명을 제외한 모든 환자는 복막외 접근법(TEP)으로 수술을 받았다. 본 연구에서 절개수술과 비교한 여자 서혜부 탈장의 복 강경 수술은 수술시간, 입원기간, 수술후 통증에 있어서 큰 차이가 없었다. 그러나 복강경 수술환자 중 4명이 외래진찰 및 초음파 검사상 1개의 탈장으로 진단되었으나 수술 중 2개 이상의 탈장이 동반된 것이 확인되었다. 또한 절개수술 에서는 대퇴 탈장이 1명도 없었으나 복강경 수술에서는 7 명이었으며, 평균연령도 다른 형태의 탈장에 비해 많았으 며, 이는 대퇴탈장이 다른 형태의 탈장에 비해 비교적 고령 5 에서 발생하는 것을 보여준다. Koch 등 의 연구에 의하면 직접 및 간접 탈장으로 수술을 받은 여자환자에서 향후 재 발환자의 52.6%가 대퇴탈장으로 재발하여 남자의 6.5%에 비해 월등히 높으며, 복강경을 이용한 탈장수술시 이러한 빈도는 상대적으로 낮다고 보고하였다. 또 다른 연구들에 7,26 서도 전체인구에서 발생하는 대퇴탈장의 빈도보다 서혜 부탈장수술 후 대퇴탈장으로 재발하는 빈도가 약 15배가 높으며, 여자의 재발 빈도가 수술방법과 상관없이 4.3%로 남자(3.1%)에 비해 높고, 재발된 예의 41.5%가 대퇴탈장으 로 남자(5.4%)에 비해 높았다. 복강경 수술은 서혜부탈장이 발생할 수 있는 취약점의 상태를 직접 확인하고 인공막을 이용하여 이 부위들을 보강하므로 상대적으로 재발의 가능 성이 낮다. 재발시 대퇴탈장의 빈도가 높은 정확한 이유는 알 수 없으나, 수술 전 대퇴탈장과 서혜부탈장이 잘 구별되 지 않는 점과 첫 수술에서 재발까지 시간이 남자보다 여자 에서 짧고 여자에게 빈도가 높은 것으로 보아 첫 수술 때 7,11,26 본 연구에서 이미 대퇴탈장이 동반되었을 가능성 높다. 는 추적기간이 상대적으로 짧고, 여자 환자수가 많지 않아 수술방법에 따른 재발율의 차이는 없었다. 골반부의 모양과 근인대의 부착모양, 그리고 서혜관을 통과하는 구조물의 모양 때문에 여자는 남자들보다 탈장의 빈도가 낮으나 대퇴탈장의 빈도는 더 높아 응급수술을 하 는 경우가 상대적으로 많다. 대퇴탈장은 상대적으로 진단.
(4) 14 Journal of Minimally Invasive Surgery Vol. 15. No. 1, 2012 과 치료가 늦어져 수술후 합병증의 빈도가 높고 심한 경우 사망에도 이를 수가 있다.5,27 복강경 서혜부탈장수술이 기 존의 절개수술과 비교하여 수술시간, 입원기간, 수술후 통 증 및 합병증에 있어서 큰 차이는 없지만 여자의 경우 대퇴 탈장의 빈도가 높아 응급수술이나 수술합병증의 위험성이 높은 만큼 수술시 대퇴탈장의 유무를 쉽게 확인하고 한번 에 탈장이 발생할 수 있는 모든 부위를 보강해줄 수 있는 복강경 탈장수술도 권할 만 하다. 절개수술에 비해 복강경 수술의 단점은 대개 전신마취가 필요하고, 비키니 선위 복부, 특히 배꼽 주위에 흉터가 생기 므로 젊은 여성에서는 술전 충분한 설명이 필요하며, 본원 에서는 미혼여성은 일반적으로 복강경 수술을 권하지 않아 절개군의 연령이 훨씬 젊다. 여자에서 서혜부탈장과 감별 되어야 할 질환중에는 지방종, 자궁내막증, 림프절, 피하양 성종양, 다양한 자궁 원인대낭종등이 있으며, 자세한 병력 청취와 이학적 검사 및 초음파, MRI 촬영으로 진단이 가능 28,29 본 연구에서 9예(13.6%)의 자궁 원인대낭종 중 7예 하다. 가 좌측에 있었으며, 1예을 제외한 모든 환자가 복강경 수 술을 받았다. 복강경 및 절개수술에서 수술시간상 유의한 차이는 없었 으나 복강경 환자군에서는 4예의 양측 탈장이 포함되어있 었다. 직접 및 대퇴탈장에 비해 간접탈장은 원인대(round ligament)와 탈장낭이 한 구조물로 존재하므로 복강경 수술 시 좀 더 복잡할 수 있다. 본원에서는 TEP 수술시 두 가지 방법을 주로 사용하는데, 탈장낭을 원인대로부터 분리한 후 원인대를 감싸는 형태로 인공막을 설치하거나(Fig. 1), 원인대와 탈장낭을 원위부에서 절단한 후 인공막을 부착하 고 원인대를 내서혜륜 근처에 고정한다. 전자가 해부학적 으로 좀 더 바람직하고 인공막 고정을 위한 핀을 사용하지 않아도 된다는 장점이 있는 반면, 후자는 수술시간을 줄일 수 있는 장점이 있다. 그러나 두 가지 방법 중 어떤 것을 선택하는데 특별한 기준은 없다. 수술 후 통증은 호르몬, 해 30,31 양 부학적 구조 및 정신적인 요인 등에 영향을 받으며, 군간 유의한 차이가 없는 것은 절개수술 환자 중 젊은 여자 에서는 고위결찰만 하거나 무장력 인공막을 이용한 수술을 했기 때문으로 생각된다.. 결. 론. 여자 환자의 서혜부 탈장은 남자에 비해 대퇴탈장 및 간 접탈장의 빈도는 높고 양측탈장은 상대적으로 적었다. 여 자 서혜부 탈장에 대한 복강경수술과 절개수술간에 수술시 간 및 입원기간, 수술 후 통증의 강도, 그리고 합병증에서는 차이가 없었다. 중년 이상의 여자에서는 대퇴탈장의 빈도 가 상대적으로 높아 수술시 대퇴탈장의 유무를 쉽게 확인 가능한 복강경 탈장수술을 선택적으로 권할 만 하다고 판 단되나, 재발율의 차이에 대해서는 좀 더 많은 환자를 대상. 으로 장기추적관찰결과를 알아보아야 하겠다.. 참고문헌 1) Alvarez JA, Baldonedo RF, Bear IG, Sols JA, Alvarez P, Jorge JI. Incarcerated groin hernias in adults: presentation and outcome. Hernia 2004;8:121-126. 2) Kulah B, Kulacoglu IH, Oruc MT, Duzgun AP, Moran M, Ozmen MM, et al. Presentation and outcome of incarcerated external hernias in adults. Am J Surg 2001;181:101-104. 3) Sandblom G, Haapaniemi S, Nilsson E. Femoral hernias: a register analysis of 588 repairs. Hernia 1999;3:131-134. 4) Glassow F. Femoral hernia. Review of 2105 repairs in a 17 year period. Am J Surg 1985;150:353-356. 5) Koch A, Edwards A, Haapaniemi S, Mordin P, Kald A. Prospective evaluation of 6895 groin hernia repairs in women. Br J Surg 2005;92:1553-1558. 6) Nilsson E, Kald A, Anderberg B, Bragmark M, Fordell R. Haapaniemi S, et al. Hernia surgery in a defined population: a prospective three year audit. Eur J Surg 1997;163:823-829. 7) Bay-Nielsen M, Kehlet H. Inguinal herniorrhaphy in women. Hernia 2006;10:30-33. 8) Heikkinen TJ, Haukipuro K , Koevukangas P, Hulkko A. A prospective randomized outcome and cost comparison of totally extra-peritoneal endoscopic hernioplasty versus Lichtenstein operation among employed patients. Surg Laparosc Endosc 1998;8:338-344. 9) Pawanindra L, Kajla RK, Chander J, Saha R, Ramteke VK. Randomized controlled study of laparoscopic total extraperitoneal versus open Lichtenstein inguinal hernia repair. Surg Endosc 1996;17:850-856. 10) Lau H, Patil NG, Yuen WK. Day-case endoscopic totally extraperitoneal inguinal hernioplasty versus open Lichtenstein hernioplasty for unilateral primary inguinal hernia in males. A randomized trial. Surg Endosc 2006;20:76-81. 11) Kark AE, Kurzer M. Groin hernias in women. Hernia 2008; 12:267-270. 12) Lau H, Patil NG, Yuen WK. Is endoscopic totally extraperitoneal herioplasty justified for the repair of groin hernia in female patients? Surg Endosc 2005;19:1544-1548. 13) Youn SI, Kim BG, Cha SJ, Chang IT. The comparative analysis between laparoscopic inguinal herniorrhphy and open inguinal herniorrhaphy. J Korean Surg Soc 2005;69:166-171. 14) Chung CS, Lee JE, Joh YG, Yu SH, Jeong GY, Kim SH, et al. The incidence of the occult contralateral hernina in patients undergoing total extraperitoneal (TEP) repair of a left inguinal hernia. J Korean Soc Endosc Laparosc Surg 2009;12:50-53. 15) McVay CB, Savage LE. Etiology of femoral hernia. Ann Surg 1961;154:25. 16) Glassow F. An evaluation of the strength of the posterior wall of the inguinal canal in women. Br J Surg 1973;60:342-344..
(5) Choon Sik Chung et al.: Comparison of Inguinal Hernia in both Sexes. 17) Serpell JW, Jarrett PE, Johnson CD. A prospective study of bilateral inguinal hernia repair. Ann R Coll Surg Engl 1990; 72:299-303. 18) Jagad RB, Shah J, Patel GR. The laparoscopic transperitoneal approach for irreducible inguinal hernias: perioperative outcome in four patients. J Minimal Access Surg 2009;5:31-34. 19) Vidović D, Kirac I, Glavan E, Filipović-Cugura J, Ledinsky M, Bekavac-Beslin M. Laparoscopic totally extraperitoneal hernia repair versus open Lichtenstein hernia repair: results and complications. J Laparoendosc Adv Surg Tech 2007;17: 585-590. 20) Duron JJ, Hay JM, Msika S, Gaschard D, Domergue J, Gainant A, et al. Prevalence and mechanisms of small intestinal obstruction following laparoscopic abdominal surgery: a retrospective multicenter study. French Association for Surgical Research. Arch Surg 2000;135:208-212. 21) Evans MD, Williams GL, Stephenson BM. Low recurrence rate after laparoscopic (TEP) and open (Lichtenstein) inguinal hernia repair: a randomized, multicenter trial with 5-year follow-up. Ann Surg 2009;250:354-355. 22) Eklund AS, Montgomery AK, Rasmussen IC, Sandbue RP, Bergkvist LA, Rudberg CR. Low recurrence rate after laparoscopic (TEP) and open (Lichtenstein) inguinal hernia repair: a randomized, multicenter trial with 5-year follow-up. Ann Surg 2009;249:33-38. 23) O’Dwyer PH, MRC Laparoscopic Groin hernia Trial Group. Laparoscopic versus open repair of groin hernias: a random-. 15. ized controlled comparison. Lancet 1999;354:185-190. 24) Lal P, Kajla RK, Chander J, Saha R, Ramteke VK. Randomized controlled study of laparoscopic total extraperitoneal vs open Lichtenstein inguinal hernia repair. Surg Endosc 2003;17: 850-856. 25) Schererlein H, Schiller A, Schneider C, Scheidback H, Tamme C, Kockerling R. Totally extraperitoneal repair of recurrent inguinal hernia. Results from 179 consecutive patients. Surg Endosc 2003;17:1072-1076. 26) Mikkelsen T, Bay-Nielsen M, Kehlet H. Risk of femoral hernia after inguinal herniorrhaphy. Br J Surg 2002;89:486-488. 27) Bendavid R. Femoral hernias: primary versus recurrence. Int Surg 1989;71:99-100. 28) Oh SN, Jung SE, Lee JM, Chung JH, Park GS. Sonographic diagnosis of a round ligament cyst in the inguinal area. J Clin Ultrasound 2007;35:226-228. 29) Lee HS, Joo KB, Song HT, Kim YS, Park DW, Park CK, et al. Relationship between sonographic and pathologic findings in epidermal inclusion cysts. J Clin Ultrasound 2001;29: 374-383. 30) Lau H, Patil NG. Acute pain after endoscopic totally extraperitoneal (TEP) inguinal hernioplasty: multivariate analysis of predictive factors. Surgical Endoscopy 2004;18:92-96. 31) Robinson ME, Riley JL III, Brown FF, Gremillion H. Sex differences in response to cutaneous anesthesia: a double-blind randomized study. Pain 1988;77:143-149..
(6)
수치
관련 문서
24 Comparison between profiles of acoustic pressure and heat transfer augmentation in case of output power level of 300W.. 25 Comparison between profiles of acoustic pressure
(2002) Blinded, randomized, multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily filgrastim as an adjunct to chemotherapy in
Patient had laparoscopic surgery on the adnexal tumor and excised tissue was removed through Douglas pouch incision by single surgeon.. Results: The mean age
The purpose of this case study was to find comparison of sports related physical fitness and anaerobic power changes of college hockey players and
Pelvic floor muscle training versus no treatment for urinary incontinence in women.. Acute back pain: a control-group comparison of behavioral vs
This study investigated sociopsychological influences on cosmetic surgery acceptance, including upward appearance comparison, awareness of an emphasis on beauty
In this study, we determined the Ce of remifentanil for preventing emergence cough following extubation in male and female elderly patients and evaluated the
Previous studies suggested using the poste- rior condylar axis (PCA) [12], Whiteside’s line [18] or the transepicondylar axis (TEA) [9, 11, 14, 20] as a reference axis
