http://dx.doi.org/10.12671/jkfs.2016.29.1.61
61
Copyright ⓒ 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received October 27, 2015 Revised November 23, 2015 Accepted November 23, 2015
Address reprint requests to: Sam-Guk Park, M.D.
Department of Orthopaedic Surgery, Yeungnam University Medical Center, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: 82-53-620-3640ㆍFax: 82-53-628-4020
E-mail: [email protected]
Financial support: None. Conflict of interest: None.
골다공성 상완골 근위부 분쇄골절에 대한 내외측 이중 금속판 내고정술
- 2예 보고 -
박삼국
영남대학교의료원 정형외과
Medial and Lateral Dual Plate Fixation for Osteoporotic Proximal Humerus Comminuted Fracture
- 2 Case Reports -
Sam-Guk Park, M.D.
Department of Orthopaedic Surgery, Yeungnam University Medical Center, Daegu, Korea
Some proximal humeral fractures in elderly patients are accompanied by medial metaphyseal comminution and quality of the bone is so poor that head preserving osteosynthesis seems to be amenable. In cases of medial metaphyseal comminution, lateral locking compression plate (LCP) fixation also has a tendency to become a matter of screw cut out or loss of fixation.
The author reports on successful treatment of two osteoporotic proximal humeral fractures combined with medial meta- physeal comminution, with application of additional direct medial supporting plate fixation. Medial plate fixations were added when the fractures were still unstable after the conventional lateral LCP fixation and anterior circumflex humeral arteries had been ruptured before. The fixations were stable enough to start exercise immediately after surgery. The inclinations of the humeral neck were not changed until the last follow-up and clinical results were satisfactory without humeral head osteonecrosis which was a concern.
Key Words: Proximal humerus, Fracture, Osteoporosis, Osteonecrosis, Dual plate fixation
상완골 근위부 골절은 노년층 인구의 증가와 골다공증 환자의 증가로 발생 빈도가 증가하고 있는 추세이다.1) 고
령의 환자의 경우 분쇄상 골절이 많고 골질이 좋지 않아 수술시 견고한 내고정을 얻기가 힘들다. 또한 수술 후 정 복의 소실, 나사의 관절면 돌출, 내고정물의 파괴, 부정 유 합 및 불유합, 견봉하 충돌, 상완골 두 무혈성 괴사 등의 문제점이 보고되어 왔다.2-4) 특히 내측 골간단부 분쇄가 동 반된 경우에는 잠김 나사 금속판을 이용하여도 내반 변형, 나사 탈출, 관절 내 나사 관통과 같은 심각한 합병증이 보 고되고 있다.3,4) 이를 예방하기 위해 잠김 압박 금속판을 이용한 내고정 후 극상건에 긴장대 방법으로 고정을 추가 하거나,2) 동종 지주골 이식을 이용한 잠김 압박 금속판 고
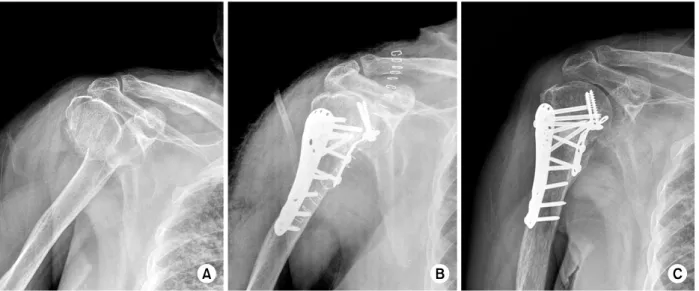
Fig. 1. (A) Preoperative anteroposterior radiograph suggested 3 part humerus surgical neck fracture according to Neer classifi- cation. (B) Immediate postoperative anteroposterior radiograph showing satisfactory fracture alignment with medial & lateral plate fixation. (C) Radiograph taken 50 weeks postoperatively showing no noticeable neck-shaft angle change in comparison with immediate postoperative plain radiograph and healing.
증례 보고
1. 증례 1
70세 여자 환자로 논에서 일하다 넘어져 우측 견과절 부 위에 손상을 받아 응급실에 내원하였다. 이학적 소견상 견 관절 부위에 심한 압통, 부종 동반된 통증으로 운동제한 호소하였으며, 개방창은 없었고 신경학적 손상도 없었다.
방사선 검사상 Neer의 분류법에 따라 3분 골절에 해당하였 다(Fig. 1A). 컴퓨터 단층촬영 검사상 대결절, 소결절, 골간 단부 분쇄가 동반되었고 골두측 골간단부가 12 mm 정도 남아 있었으며 내측 지주의 분쇄가 동반된 상태였다(Fig. 2).
대퇴골 근위부의 골밀도 검사에서 T score는 −3.3점이었 으며 환자는 당뇨병을 앓고 있었다. 환자는 동종골 이식과 같은 고가의 치료는 거부하였고, 치료 후 농사일을 다시
Rico, Mexico)를 이용하여 극상건, 극하건, 견갑하건에 통 과시켜 대결절과 소결절을 정복하였으며, 골간단부 골절의 외측을 정복한 후 LCP (proximal humerus locking plate;
Zimmer, Warsaw, IN, USA)로 고정하였으나 상완 이두 장 건과 단건 사이로 손가락을 밀어 넣어 상완골 경부 내측을 외측으로 밀어본 결과 불안정성이 남아있었다. 상완 이두 장건을 절단한 후 상완 이두 단건을 내측으로 밀어 전견갑 근을 상방으로 견인하고 상완을 외전, 외회전시켜 골간단 부 내측의 분쇄상 및 불안정성을 확인할 수 있었기에 T형 금속판(3 hole; Zimmer)을 내측 지지가 되도록 변형시켜 고 정하였다. 수술 시야에서 내반 변형과 불안정성이 호전된 것을 확인할 수 있었고, 영상 증폭장치를 이용하여 견고한 고정을 확인할 수 있었다. 골간단부 결손부위로 골 대치물 (Bone medic-s; Meta Biomed, Cheongju, Korea)을 채우고 대흉근 절개 부위와 절단했던 이두 장건을 같이 봉합하였
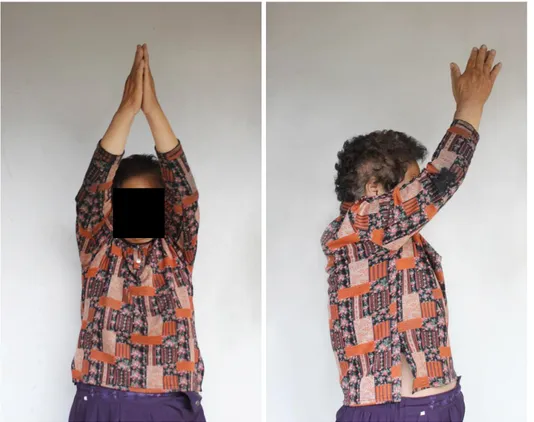
Fig. 3. Photographs of the pa- tient taken 3 years postopera- tively showing abduction of right shoulder joint to 180 degrees and forward flexion to 140 degrees, the same as her left shoulder.
Fig. 2. (A, B) Three dimensional computed tomography image showing comminuted fracture at great tubercle, lesser tubercle and medial metaphysis. (C) Two dimensional computed tomography image suggested the length of the metaphyseal head extension was 12 mm and integrity of medial hinge was disrupted.
이를 하였고, 통증이 호전된 수술 후 5일경부터 추 운동을 시작하였으며, 3주 후부터 능동 보조 운동을 시작하였다.
술 후 6주경부터 유합이 진행되는 것을 관찰할 수 있었고 일상 생활을 시작했으며, 술 후 12주경 고정 상실 없이 정 상적 유합을 얻어 농사일을 시작하였다. 술 후 50주경 경 간 각(neck shaft angle)은 140o로 수술 직후와 변화가 없 었으며(Fig. 1C), 술 후 3년경 기능적 검사상 시각 상사 척 도(visual analogue scale)로 측정한 주관적 통증의 정도는
1.0점이었으며, 견관절의 운동 범위는 전방 거상 140o, 신 전 50o, 외전 180o, 외회전 80o, 내회전 제12흉추 높이를 보였고(Fig. 3), Constant 점수 81점으로 만족할 만한 결과 를 얻었다. 추적관찰 기간 동안 내반 변형(varus malalign- ment), 나사 탈출(screw cutout), 관절 내 나사 관통(articular penetration), 골 괴사(osteonecrosis), 감염 등의 합병증은 관찰되지 않았다.
Fig. 5. Photographs taken during the surgery. (A) Humerus head was dislocated anteriorly and metaphysis was severely com- minuted with bone defect. (B) Unstable varus malalignment state after lateral locking compression plate fixation. (C) Stable acceptable alignment after additional medial buttressing plate fixation.
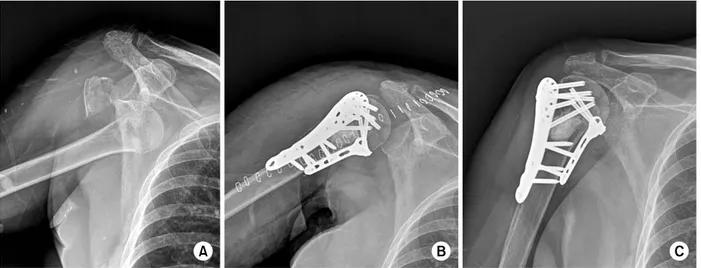
Fig. 4. (A) Preoperative anteroposterior plain radiograph showing the proximal humeral comminuted fracture (Neer type 3) with shoulder joint dislocation. (B) Immediate postoperative plain radiograph showing satisfactory fracture alignment with medial &
lateral plate fixation and reduced shoulder joint. (C) Radiograph taken 54 weeks postoperatively showing no noticeable neck- shaft angle change in comparison with immediate postoperative plain radiograph and healing.
시도하였으나 실패하였다(Fig. 4A). 수술 시 삼각대흉간 접 근법을 사용하였으며 전 회선 상완동맥은 파열되어 외측으
상완 신경총 손상 받은 상태라는 결과가 나왔다. 술 후 6 주경부터 능동적 운동을 할 수 있을 정도로 호전되었다.
수술 후 4일경부터 추 운동을 시작하였으며, 6주 후부터 능동 보조 운동을 시작하였다. 술 후 12주경 정상적 유합 을 확인할 수 있었고 술 후 12개월경 기능적 검사상 시각 상사 척도로 측정한 주관적 통증의 정도는 1.2점이었다.
경간각(neck shaft angle)은 145o로 수술 직후와 최종 추시 에서 변화가 없었으며(Fig. 4C), 견관절의 운동 범위는 전 방 거상 140o, 신전 40o, 외전 135o, 외회전 60o, 내회전 제 12흉추 높이를 보였고, Constant 점수 79점으로 만족한 결 과를 얻었다. 추적 관찰기간 동안 대결절의 작은 골편이 10 mm 정도 전위되었으나 다른 특별한 합병증은 관찰되 지 않았다.
고 찰
골질이 불량하고 골다공증이 있는 고령의 전위된 상완골 근위부 복합 골절에서 LCP 고정 시 내측 피질골 지지대를 복원하여 안정성을 유지할 수 있는 정복을 시행하는 것이 수술 후 정복의 유지 및 유합률을 높이고 합병증의 발생을 줄이는 데 중요한 요인이다.2) 그러나 골다공증이 동반된 상 완골 근위부 분절 분쇄 골절에서는 골간단부에 골결손 및 내측 피질골의 분쇄골절이 동반되는 경우가 많아 내측 지 지대의 안정적 복원이 어려운 경우가 많다. 따라서 LCP 고정 시 최소한 5개 이상의 나사가 다른 방향으로 분기(di- vergent)하게 삽입되어야 하고, 상완골 두가 내반되어 내측 의 지지가 불안정한 골절에서는 고정의 안정성을 얻기 위 해서 상완 거(humeral calcar)를 따라 상완골 두의 아래쪽 으로 잠금 나사를 위치시키는 것이 매우 중요하다. 이 나 사는 후하방 거(posteroinferior calcar)의 결손이 있어 불안 정한 골절에서 골절 부위를 압박하고 지지하는 중요한 역 할을 한다.1) 그 외에 골이식, 추가적인 긴장대 강선 고정, 지주골 이식을 동반한 금속판 고정 등 추가적 안정성을 얻 는 여러 가지 방법들이 시도되고 있다.2,5) 그러나 정복과 유지가 어려워 고정 실패가 흔히 발생할 수 있고, 이런 이 유로 분쇄 및 전위가 심한 근위부 상완골 3, 4분절 골절에 서는 인공관절 반치환술 또는 역행성 견관절 전 치환술 등 의 관절 성형술이 선택되는 경우도 증가하고 있다.3) 내측 주(medial column)가 불안정하여 외측에 LCP 고정 후 내 측에 추가적인 지지 금속판 고정 시 더 견고한 고정을 얻 을 수 있다는 생역학적 연구 보고가 있으나,6) 상완골 근위 부의 내측으로 접근하려면 상완골 두의 혈류 공급에 주된 역할을 하는 전 회선 상완 동맥을 희생시키게 되고,7) 따라 서 상완골 두의 무혈성 괴사가 초래될 우려가 있다. 그러 나 상완골 근위부 골절 환자의 80%에서 전 상완 회선 동 맥은 파열되는데 상완골 두 무혈성 괴사의 예는 그렇게 많 지 않지 않으며, 후 회선 상완 동맥(posterior humerus cir-
cumflex artery)은 상완골 근위부 골절 환자의 85%에서 정 상이라는 보고가 있고,8) 상완골 근위부 골절 시 후 회선 상완 동맥이 더 중요한 역할을 한다는 보고도 있다.9,10) 일 반적으로 전 회선 상완 동맥을 절제하고 수술하게 되는 개 방적 반카르트 복원술(open Bankart operation)의 합병증 으로 상완골 두 무혈성 괴사를 보고한 문헌도 찾아볼 수 없었다. 저자의 2예에서도 수술 시야에서 전 회선 상완 동 맥은 이미 파열된 상태를 확인할 수 있었기에 내측 접근을 시도하였고, 상완골 두 무혈성 괴사에 가장 중요한 요소로 골 두측 골간단부의 길이와 내측 지지대의 안정성이라는 보고9)가 있어서 내측 지지 금속판 고정을 추가하여 확실한 내측 안정성을 부여하는 것이 오히려 상완골 두 무혈성 괴 사를 예방할 수 있는 방법이 될 수도 있다고 생각했다.
저자는 외측 잠김 압박 금속판 고정으로 안정성을 얻을 수 없는 골다공증이 동반된 환자의 상완골 근위부 분쇄 골 절에서 추가적인 내측 지지 금속판 고정을 시행하여 조기 에 관절 운동이 가능한 견고한 고정을 얻었으며, 수술 후 합병증 없이 순조로운 유합과 함께 만족스러운 기능적 결 과를 얻을 수 있었다. 고령의 근위 상완골 골절의 수술적 치료 시 골간단부에 골결손 및 내측 피질골의 분쇄골절이 동반되어 외측 잠김 압박 금속판 고정 후에도 내측 지지가 충분하지 않아 불안정성이 있는 경우, 전 회선 상완 동맥 이 이미 파열되어 있다면 상완골 경부 내측 접근을 이용한 이중 금속판 고정술은 확실한 내측 지지대의 안정성을 부 여할 수 있기에 고려해 볼만한 수술 방법이라고 생각된다.
그러나 전 회선 상완 동맥의 희생과 상완골두 무혈성 괴사 의 연관성, 수술 중 근피 신경(musculocutaneous nerve)과 액와 신경(axillay nerve) 손상 가능성, 그리고 추가적인 안 정성을 얻기 위한 여러 가지 수술 방법과의 비교 관찰에 관한 장기적 추시 관찰과 추가적인 연구가 필요할 것으로 생각된다.
References
1) Oh JH, Kim YH: The current concepts in the treatment of proximal humerus fracture. J Korean Fract Soc, 25:
94-104, 2012.
2) Hawkins RJ, Bell RH, Gurr K: The three-part fracture of the proximal part of the humerus. Operative treatment.
J Bone Joint Surg Am, 68: 1410-1414, 1986.
3) Jung HJ, Jeon IH, Chun JM: Arthroplasty for fractures of the proximal part of the humerus. J Korean Orthop Assoc, 47: 243-249, 2012.
4) Ricchetti ET, Warrender WJ, Abboud JA: Use of lock- ing plates in the treatment of proximal humerus fractures.
Bone Joint Surg Am, 72: 1486-1494, 1990. Surg Am, 92: 943-948, 2010.
Copyright ⓒ 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
http://dx.doi.org/10.12671/jkfs.2016.29.1.61
골다공성 상완골 근위부 분쇄골절에 대한 내외측 이중 금속판 내고정술
- 2예 보고 -
박삼국
영남대학교의료원 정형외과
골다공증성 또는 내측 골간단부 분쇄가 동반된 고령의 상완골 근위부 분쇄 골절의 경우 외측 잠김 압박 금속판을 사용하여도 견고한 고정을 얻기 어려운 경우가 있어 치료 방법에 대하여 논란이 되고 있다. 저자는 골다공증이 동반된 고령의 환자에서 내측 골간단부 분쇄가 동반된 불안정성 상완골 골절에 전 상완 회선 동맥이 파열되어 있고, 외측 잠김 나사 금속판 고정 후에도 견고한 내고정을 얻지 못한 경우 추가적으로 내측지지 금속판 고정으로 견고한 고정을 얻어 조기에 견관절 운동을 허용할 수 있었다. 고정 상실 없이 순조로운 유합을 얻었으며, 우려했던 상완골 두 무혈성 괴사 없이 견관절의 기능은 만족스럽게 회복 되었음을 보고하는 바이다.
색인 단어: 상완골 근위부, 골절, 골다공증, 무혈성 괴사, 이중 금속판 내고정술
접수일 2015. 10. 27 수정일 2015. 11. 23 게재확정 2015. 11. 23 교신저자 박삼국
42415, 대구시 남구 현충로 170, 영남대학교의료원 정형외과
Tel 053-620-3640, Fax 053-620-4020, E-mail [email protected]
67