294
서 론
우리나라에서 위암은 가장 흔한 암이며, 전체 암 사망률 중에 두 번째로 많은 빈도를 차지하고 있다.(1) 위암의 치료 는 림프절 곽청을 포함한 근치적 절제술이 재발을 줄이고 생존율 향상을 기대할 수 있는 필수적 요소이며, 위벽 침윤 도와 림프절 전이가 가장 중요한 예후인자로 인정되고 있 다.(2-4) 위암에 대한 사회적 관심과 진단기법의 발달로 조 기위암의 빈도가 증가하는 추세에 있으나 아직도 장막침윤 위암(T3)이 전체 위암의 30% 정도를 차지하며,(5) 이 경우 여전히 예후가 불량하고 동일 병기 내에서도 예후차이가 심하기 때문에 예후에 영향을 미치는 인자들을 분석하는 노력이 필요하다.(6-8) 현재 사용하는 림프절 전이에 대한
Prognostic Factors for Serosal Invasive Gastric Cancer: Clinical Significance of Metastatic Lym ph Node Ratio
Jong-Han Kim, M.D., Yoon-Jung Boo, M.D., Sung-Soo Park, M.D., Jin Kim, M.D., Seung-Joo Kim, M.D., Young- Jae Mok, M.D. and Chong-Suk Kim, M.D.
Purpose: The important prognostic factors for gastric cancer are the depth of invasion by the primary tumor and the lymph node metastasis. The 5th edition of the Union Internationale Contrala Cancrums (UICC) TNM classification, which is based on the number of metastatic lymph nodes, has proved to be a reliable and objective method for predicting the prognosis of patients suffering with gastric cancer. However, its value for the prognosis of treating patients with serosal invasive (T3) gastric cancer, it is still being debated. So, we retrospectively studied the prognostic factors for T3 gastric cancer patients and we also evaluated the staging method according to the number of metastatic lymph nodes and the metastatic lymph node ratio.
Methods: This retrospective study was based on the medical records of 369 patients who underwent curative resection for serosal invasive (pT3) gastric cancer from 1992 to 2000. The patients were divided into four groups according to the number of metastatic lymph nodes and the clinicopathologic factors were evaluated by comparative study and the patients were then, classified into 4 groups by the metastatic lymph node ratio (<0.1, 0.1∼0.3, 0.3∼0.5, >0.5). We evaluated the prognostic factors and performed a survival analysis by using the Kaplan-Meier method and the Cox proportional hazard model.
Results: Among the four groups, the significant different factors were tumor size, the Borrmann type, the type of gastrectomy, the histologic type, and lymph node dissection.
장막침윤 위암의 예후인자-림프절 전이 비율의 임상적 의미
고려대학교 의과대학 외과학교실
김종한․부윤정․박성수․김 진․김승주․목영재․김종석
According to the univariate survival analysis, the tumor size, Borrmann type, lymph node stage, and the metastatic lymph node ratio significantly affected the prognosis. Yet, when comparing each survival rate, there was not significant dif- ference between the pT3pN0 and pT3pN1 calassification.
When we classified the metastatic lymph node ratio into 4 categories, each group then showed a significantly different survival rate. By conducting a multivariate analysis, only the metastatic lymph node ratio was an independent prognostic factor for serosal invasive gastric cancer (P=0.028).
Conclusion: For evaluating patients with serosal invasive gastric cancer, there have been some problems with using the lymph node staging, so the metastatic lymph node ratio is a more reliable prognostic factor as it provides information about the extent of lymph node dissection and the degree of lymph node metastasis. (J Korean Surg Soc 2006;70:
294-300)
Key Words: Serosal invasive gastric cancer, Lymph node stage, Metastatic lymph node ratio
중심 단어: 장막 침윤성 위암, 림프절 병기, 전이 림 프절 비율
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, College of Medicine, Korea Univer- sity, Seoul, Korea
책임저자:김종석, 서울시 성북구 안암동 5가 126-1 ꂕ 136-705, 고려대학교 의과대학 외과학교실 Tel: 02-920-5866, Fax: 02-928-1631
E-mail: [email protected]
접수일:2005년 9월 20일, 게재승인일:2006년 1월 2일
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 평가는 1997년 제5판 UICC TNM 병기 분류에 따라서 전이
된 림프절의 수에 따라서 병기를 나누고 있으며, 이는 1987 년 제4판 UICC와 일본 위암학회에서 정한 해부학적 위치에 따른 림프절 구분 병기 분류에 비하여 객관적이고 편리한 방법으로 밝혀져 널리 사용되고 있다.(2,9-15) 하지만 이러 한 장점에도 불구하고 몇 가지 제한점이 지적되고 있는데 우선 정확한 병기 설정을 위해 충분한 수의 림프절 절제가 필요하며 절제 림프절의 수가 증가함에 따라 동일 병기에 서 예후가 달라지는 병기 이동 현상이 발생할 수 있 다.(11,16)
최근 들어, 전이된 림프절의 수보다 절제된 림프절의 수 에 대한 전이 림프절의 비율이 더욱 객관적으로 림프절 전 이 정도를 나타낸다는 주장이 제기되고 있다.(8,17-19) 이에 저자들은 진행성 위암 중 장막 침윤 위암에 대하여 예후인 자를 분석하고 전이 림프절 수와 전이 림프절 비율(NR:
Lymph node Ratio)에 따른 생존율을 비교 분석하여 N stage 로 과연 어느 기준이 더 정확한 예후 판정을 할 수 있는지 알아보고자 하였다.
방 법
1992년부터 2000년까지 고려대학교 의과대학 외과학교 실에서 위암으로 진단 후 수술을 시행 받은 1,430명의 환자 중 술 후 종양의 위벽 침윤도에 있어 1992년 대한위암학회 와 1997년 AJCC에서 정한 규칙에 따라 병리학적으로 장막 에 침윤을 동반하고 주위 인접 장기로 침윤하지 않은 경우 를 pT3로 정하여(20) 장막 침윤성(pT3) 위암으로 분류된 519예를 대상으로 하였다. 림프절 전이 외의 혼란 요소를 배제하기 위하여 원격전이를 동반한 67예와 비 근치적 절 제술을 시행 받은 44예, 절제된 림프절 개수가 15개 미만인 39예를 제외한 369예에서 후향적 연구를 시행하였다.
제5판 UICC 분류법 20에 근거하여 환자 군을 4개의 군으 로 나누어 각각의 군에 대한 임상 병리학적 특성을 비교 분석하였다. 전체 환자 369명 중 N0군이 70명, N1군이 135 명, N2군이 108명, 그리고 N3군이 56명이었다. 절제된 림프 절 수에 대한 전이 림프절의 비율(NR)에 의한 분류가 의미 가 있는지 알아보기 위해 전체 환자를 NR에 따라 다시 4개
의 군(<0.1: NR1, 0.1∼0.3:NR2, 0.3∼0.5: NR3, >0.5:
NR4)으로 나누어 이전의 UICC 분류법과의 차이를 비교 분 석하였는데 이는 각 림프절 병기에서 절제된 림프절 수에 대한 전이 림프절 수의 비율을 구한 값을 바탕으로 기준을 정하였다.
예후인자 분석을 위하여 각각의 임상병리학적 특성을 가 지고 단변량 분석을 시행하였고 이 중 의미 있는 인자들에 대하여 다변량 분석을 시행하였다. 평균 추적 기간은 52.7
±37.0개월이었으며, 전체 369예 중 사망 202예, 생존 142 예, 그리고 중도탈락 25예로서 추적률은 93.2%였다.
통계학적 분석은 SPSS 12.0K for windows를 이용하여 시 행하였고 각 군 간의 임상 병리학적 특성의 비교에는 Ch- square test와 ANOVA를 사용하였으며 Kaplan-Meier법으로 생존율을 구하였고 Log-Rank법으로 비교하였다. 또한 의미 있는 인자들에 대한 다변량 분석은 Cox's proportional hazard model을 사용하였으며 P값이 0.05 미만인 경우 유의 한 것으로 판정하였다.
결 과
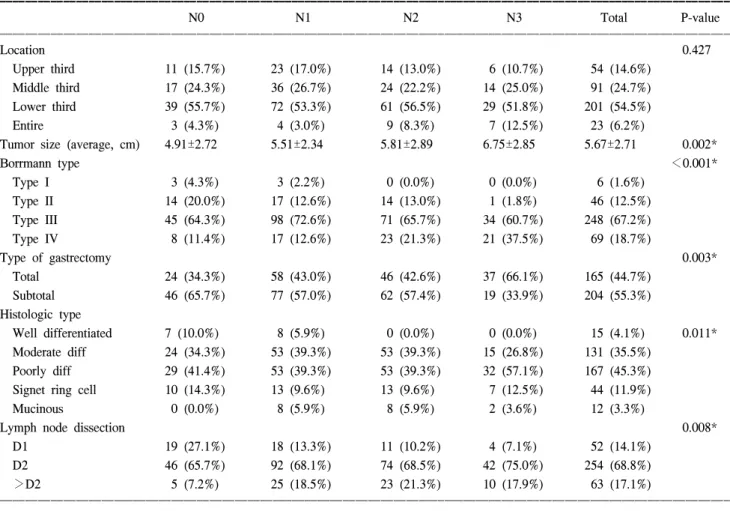
1) UICC림프절 병기에 따른 임상병리학적 특성 대상환자 369명을 제5판 UICC 분류법에 근거한 림프절 병기에 따라 4군으로 나누어 임상 병리학적 특성을 비교 분석하였을 때 전체 군에서 평균연령은 56.35세였으며 남 자가 246명, 여자가 123명으로 각 군 간에 있어서 평균연령 과 남녀 비율은 유의한 차이를 보이지 않았다(Table 1). 종 양의 위치는 하부위암이 201예(54.5%)로서 가장 높은 빈도 를 보였으나 각 군 간에 유의한 차이를 보이지 않았다. 종양 의 크기는 병기가 증가할수록 유의하게 증가하였다. Borr- mann 형은 제2형과 제3형의 경우 저 병기에서 빈도가 높았고 제4형의 경우 N2군에서 23예(21.3%), N3군에서 21예(37.5%)로 고 병기에서 상대적으로 유의하게 높았다. 위 절제술의 형 태에 있어서는 N0군에서 전 절제술이 24예(34.3%), 아전 절 제술이 46예(65.7%)였고 N3군에서 전 절제술이 37예(66.1%), 아전 절제술이19예(33.9%)로 고 병기에서 전 절제술을 시 행 받은 경우가 유의하게 많았다. 조직 형의 경우 전체 군에 서 미분화형이 167예(45.3%)로 유의하게 많은 빈도를 보였
Table 1. Patient's characteristics according to lymph node stage in T3 gastric cancer
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Lymph node stage T3N0 (n=0) T3N1 (n=1∼6) T3N2 (n=7∼15) T3N3 (n≥16) Total P-value
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Average age (yrs) 56.59±11.46 56.79±11.26 56.52±11.86 54.64±13.93 56.35±11.88 0.709
Sex 0.684
Male 48 (68.6%) 93 (68.9%) 67 (62.0%) 38 (67.9%) 246 (66.7%)
Female 22 (31.4%) 42 (31.1%) 41 (38.0%) 18 (32.1%) 123 (33.3%)
Total 70 (19.0%) 135 (36.6%) 108 (29.3%) 56 (15.2%) 369 (100%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
으며 특히 N3군에서 32예(57.1%)로 가장 높은 빈도를 보였 다. 림프절 절제 방법에 있어서 N0군에서 D1절제술이 19예 (27.1%), D2절제술이 46예(65.7%)였으며 N3군에서 D1절제 술 4예(7.1%), D2절제술 254예(75.0%)로서 병기가 증가할수 록 D2 이상의 절제술을 시행 받는 경우가 많았다(Table 2).
절제 림프절 전체 수는 전체 군에서 평균 37.1±14개의 절 제를 시행하였는데 병기가 증가할수록 절제 림프절 수가
증가하였다. 병기에 따른 절제 림프절 수에 대한 전이 림프 절 수의 비율을 구하였을 때 N1군이 0.11±0.08, N2군이 0.30±0.15, N3군이 0.54±0.18로 나타났다(Table 3).
2) 임상병리학적 특성 및 림프절 전이에 따른 생존율 분석
생존율 분석 결과 전체 369명 환자의 5년 누적 생존율은 Table 2. Clinicopathologic factors according to lymph node stage in T3 gastric cancer
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
N0 N1 N2 N3 Total P-value
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Location 0.427
Upper third 11 (15.7%) 23 (17.0%) 14 (13.0%) 6 (10.7%) 54 (14.6%) Middle third 17 (24.3%) 36 (26.7%) 24 (22.2%) 14 (25.0%) 91 (24.7%)
Lower third 39 (55.7%) 72 (53.3%) 61 (56.5%) 29 (51.8%) 201 (54.5%)
Entire 3 (4.3%) 4 (3.0%) 9 (8.3%) 7 (12.5%) 23 (6.2%)
Tumor size (average, cm) 4.91±2.72 5.51±2.34 5.81±2.89 6.75±2.85 5.67±2.71 0.002*
Borrmann type <0.001*
Type I 3 (4.3%) 3 (2.2%) 0 (0.0%) 0 (0.0%) 6 (1.6%)
Type II 14 (20.0%) 17 (12.6%) 14 (13.0%) 1 (1.8%) 46 (12.5%)
Type III 45 (64.3%) 98 (72.6%) 71 (65.7%) 34 (60.7%) 248 (67.2%)
Type IV 8 (11.4%) 17 (12.6%) 23 (21.3%) 21 (37.5%) 69 (18.7%)
Type of gastrectomy 0.003*
Total 24 (34.3%) 58 (43.0%) 46 (42.6%) 37 (66.1%) 165 (44.7%)
Subtotal 46 (65.7%) 77 (57.0%) 62 (57.4%) 19 (33.9%) 204 (55.3%)
Histologic type
Well differentiated 7 (10.0%) 8 (5.9%) 0 (0.0%) 0 (0.0%) 15 (4.1%) 0.011*
Moderate diff 24 (34.3%) 53 (39.3%) 53 (39.3%) 15 (26.8%) 131 (35.5%)
Poorly diff 29 (41.4%) 53 (39.3%) 53 (39.3%) 32 (57.1%) 167 (45.3%)
Signet ring cell 10 (14.3%) 13 (9.6%) 13 (9.6%) 7 (12.5%) 44 (11.9%)
Mucinous 0 (0.0%) 8 (5.9%) 8 (5.9%) 2 (3.6%) 12 (3.3%)
Lymph node dissection 0.008*
D1 19 (27.1%) 18 (13.3%) 11 (10.2%) 4 (7.1%) 52 (14.1%)
D2 46 (65.7%) 92 (68.1%) 74 (68.5%) 42 (75.0%) 254 (68.8%)
>D2 5 (7.2%) 25 (18.5%) 23 (21.3%) 10 (17.9%) 63 (17.1%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*P<0.05.
Table 3. Lymph node ratio status according to lymph node stage in T3 gastric cancer
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
N0 N1 N2 N3 Total P-value
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ No. of retrieved lymph nodes
32.94±10.32 34.15±12.92 38.51±13.67 46.95±15.63 37.14±13.91 <0.001*
(mean±SD)
No. of metastatic lymph nodes
0 3.41±1.79 10.12±2.65 23.96±7.63 7.84±8.48 <0.001*
(mean±SD)
Ratio of metastatic lymph nodes
0 0.11±0.08 0.30±0.15 0.54±0.18 0.21±0.21 <0.001*
(mean±SD)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*P<0.05. No. = number; SD = standard deviation.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
50.9%였다. 연령, 성별, 종양의 위치, 위 절제의 형태, 그리 고 조직학적 유형에 따른 5년 생존율은 차이가 없었다. 종 양의 크기에 있어서는 종양의 크기가 증가할수록 생존율이 유의하게 감소하였으며 종양 형에 있어서는 Borrmann 4형 에서 생존율이 유의하게 감소하였다. 림프절 절제 범위에 따른 5년 생존율은 D1의 경우 42.1%, D2의 경우 51.1%, D2 이상에서 54.7%로 D2 이상을 시행한 경우 생존율이 높았으 나 유의한 차이는 없었다(Table 4). 림프절 병기에 따른 5년 생존율은 N0군이 66.0%, N1군이 65.6%, N2군이 40.0%, 그 리고 N3군이 13.2%로 전체적으로 유의한 차이를 보였으나 N0군과 N1군 간에는 유의한 차이를 보이지 못하였다(Table 5, Fig. 1). 그러나 전이 림프절 비율에 따른 5년 생존율은 NR1군이 66.3%, NR2군이 54.7%, NR3군이 33.4%, 그리고
NR4군이 8.3%로서 각각의 군 간에 통계적으로 유의한 차 이를 보였다(Table 5, Fig. 2). 단변량 분석 결과 의미가 있었 던 예후 인자들은 종양의 크기, Borrmann형, 림프절 병기, 전이 림프절 비율이었고 이러한 인자들을 다변량 분석한 결과 오직 전이 림프절 비율만이 독립적인 예후인자로 나 타났다(Table 6, P=0.028).
고 찰
위암에 있어서 병기는 종양의 위벽 침윤도, 림프절 전이 정도, 원격전이의 유무에 따라 결정되며 가장 이상적인 기 준을 제시하기 위해 계속적인 연구와 개정이 이어지고 있 다. 림프절 전이 개수에 의한 제5판 UICC 병기 분류법은 기존의 전이 림프절의 위치에 따른 분류법에 비하여 객관 Table 4. Univariate survival analysis of clinicopathologic factors
in T3 gastric cancer
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Clinicopathologic No. of 5-YSR
(%) P-value
factors patients (%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Age (yrs) 0.381
<40 39 10.6 46.8
40∼64 226 61.2 53.1
≥65 104 28.2 46.2
Sex 0.299
Male 246 66.7 50
Female 123 33.3 51.6
Location 0.191
Upper third 54 14.6 49.9 Middle third 91 24.7 60.4 Lower third 201 54.5 48.5
Entire 91 6.2 30.4
Tumor size (cm) 0.013*
<3.0 68 18.4 56.2
3.0∼6.0 174 47.2 57.2
>6.0 127 34.4 37.5
Borrmann type <0.001*
Type I 6 1.6 33.3
Type II 46 12.5 66.1
Type III 248 67.2 53.2
Type IV 21 18.7 32.6
Type of gastrectomy 0.067
Total 165 44.7 44.9
Subtotal 204 55.3 54.8
Histologic type 0.187
Well differentiated 15 4.1 80 Moderate diff 131 35.5 53.1
Poorly diff 167 45.3 47
Signet ring cell 44 11.9 42.9
Mucinous 12 3.3 60.7
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Table 5. Survival analysis according to lymph node stage &
metastatic lymph node ratio
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
No. of 5-YSR
Factors (%) P-value
patients (%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Lymph node stage (UICC) <0.001*
N0 70 19 66
N1 (1∼6) 135 36.6 65.6
N2 (7∼15) 108 29.3 40
N3 (>16) 56 15.2 13.2
Ratio of metastatic lymph node <0.001*
NR1 (<0.1) 135 36 66.3
NR2 (0.1∼0.3) 137 37.1 54.7
NR3 (0.3∼0.5) 52 14.1 33.4
NR4 (>0.5) 45 12.2 8.3
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*P<0.05. NR = node ratio (metastatic lymph node ratio).
Fig. 1. Survival curves according to lymph node stage in T3 gastric cancer.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
적이고 더욱 정확히 예후를 예측할 수 있다고 인정되어 사 용되어 왔으나,(9,10,12,14) 최근에 진행 위암에서 림프절 병 기가 생존율을 정확히 반영하지 못한다는 문제점이 제기되 고 있다. 본 연구에서는 위벽 침윤도에 있어서 진행성 위암 을 대표하는 장막 침윤성(pT3) 위암에서 림프절 병기에 따 라 환자 군을 나누고 특성을 비교한 결과 종양의 크기, Borrmann형, 위 절제술의 형태, 조직형, 림프절 절제 정도에 있어서 유의한 차이를 보였고 단변량 분석결과 종양의 크 기와 Borrmann형이 예후에 영향을 미치는 것으로 나타났 다. 위암의 육안형이 예후와 깊은 관련이 있어 Borrmann IV 형이 I, II, III 형에 비해 예후가 나쁘고, 종양의 크기가 클수 록, 위암의 침윤 깊이가 깊을수록 생존율이 낮다고 보고되 고 있으며,(22,23) 이는 본 연구의 결과와 일치하였다.
Ichikura 등(10)은 제5판 UICC 림프절 병기에 따른 생존율 에 균등한 차이를 보이지 않음을 보고하였고, 각 pT 병기에 서 림프절 개수에 따라 분류하였을 때 pN0기와 pN1기에 있 어서 생존율에 차이를 보이지 않았다고 주장하였다. 본 연 구에서도 장막 침윤성(T3) 위암에 있어서, N0군과 N1군 간 에 있어서 생존율이 차이가 나지 않는 것으로 나타나 진행 성 위암에서 제5판 UICC 림프절 병기의 문제점이 발견되었 다. 저자들은 이러한 문제점이 림프절 미세전이와 관련이 있지않나 생각하였는데, 기존의 H-E 염색상 림프절 전이 음성으로 판명된 경우라 할지라도 “세포 케라틴”이라는 표 지 자를 이용하여 면역 형광 염색법으로 검사한 결과 양성 으로 나오는 경우 암세포의 미세전이를 예측할 수 있으 며,(24) Yasuda 등(25)에 의하면 T3 위암에서 일반 조직 검 사상 pN0인 경우 미세전이를 조사하였을 때 32% 정도에서 양성을 보이며 이 경우 더 낮은 5년 생존율을 보인다고 주 장하였다. 미세전이가 기존의 림프절 병기에 영향을 미치 는지에 대해서는 향후 좀더 연구가 필요하리라 사료된다.
Kodera 등(11)에 의하면 제5판 UICC 병기의 가장 큰 문제점 은 병기 이동 현상인데 이러한 현상이 특히 D1절제술을 시 행한 환자에서 두드러지며, Inoue 등(18)에 의하면 D2 절제 술을 시행했더라도 절제된 전체 림프절 개수의 영향에 의 해 병기 이동이 발생할 수 있다고 하였다. 이와 같이 제5판 림프절 병기 분류의 문제점은 림프절 병기가 절제된 전체 림프절의 개수와 림프절 곽청도에 의해 영향받을 수 있으 며 이러한 문제점을 극복하기 위해 저자들은 림프절 전이 비율(NR)에 따라 환자 군을 분류하였다. 림프절 전이 비율 분류의 기준은 연구마다 차이를 보이는데, Inoue 등(18)은 25%와 50%를 기준으로 3개의 군으로 분류하였으며, Kuni- saki 등(19)은 0.1과 0.2를 기준으로 4개의 군으로, 이 등(17) 은 0.1, 0.3, 그리고 0.5를 기준으로 5개의 군으로 분류하였 다 본 연구에서는 각 림프절 병기를 4개의 군으로 분류하였 고(<0.1, 0.1∼0.3, 0.3∼0.5, >0.5), 각각의 군에 대하여 생 존곡선을 구하였을 때 의미 있는 차이를 보였다. 전이 비율 에 따른 분류가 수에 의한 분류보다 더욱 효과적이라는 주 장들을 보면, 형 등(8)에 의하면 T3 위암에서 전이 비율이 림프절 절제 정도와 전이 정도를 함께 포함하는 요소이기 때문에 더욱 효과적으로 예후를 나타낸다고 하였으며, 이 등(17)도 D2 이상의 곽청을 시행한 경우 림프절 전이 비율 이 더욱 강한 예후 인자라고 주장하였다. Inoue 등(18)은 전 Fig. 2. Survival curves according to the metastatic lymph node
ratio (NR) in T3 gastric cancer. NR1 (node ratio 1) <0.1;
NR2=0.1∼0.5; NR4>0.5.
Table 6. Multiple stepwise regression analysis of prognostic factors with the Cox proportional hazard model ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Prognostic Relative 95% Confidence
P-value
factors risk interval
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Tumor size (cm) 0.304
<3.0 1
3.0∼6.0 1.101 0.722∼1.679
>6.0 1.35 0.869∼2.097
Borrmann type 0.082
Type I 1
Type II 0.349 0.115∼1.064
Type III 0.5 0.178∼1.406
Type IV 0.656 0.226∼1.904
Lymph node stage 0.172
N0 (n=0) 1
N1 (n=1∼6) 0.838 0.485∼1.449
N2 (n=7∼15) 1.344 0.661∼2.731
N3 (n>16) 1.563 0.661∼3.679
Metastatic lymph node ratio 0.028*
NR1 (<0.1) 1
NR2 (0.1∼0.3) 1.244 0.731∼2.118 NR3 (0.3∼0.5) 1.59 0.793∼3.186
NR4 (>0.5) 2.858 1.315∼6.214
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*P<0.05. NR = node ratio (metastatic lymph node ratio).
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 이 림프절 수에 의한 분류 시 가장 문제시되는 것이 병기
이동 현상인데 림프절 전이 비율에 의해 분류할 경우 이 문제가 해결될 수 있다고 주장하였다. 본 연구에서 생존율 에 영향을 미치는 여러 인자들에 대하여 다변량 분석을 시 행한 결과 오직 림프절 전이 비율만이 예후에 영향을 미치 는 독립적인 인자로 판명되었다.
결 론
장막 침윤성 위암에서 예후인자 분석 결과 종양의 크기, Borrmann형, 림프절 병기, 전이 림프절 비율이 예후에 영향 을 미치는 인자였으며, 이들에 대한 다변량 분석 결과 전이 림프절 비율이 독립적인 예후인자였다. 따라서, 전이 림프 절 비율에 따른 병기 분류는 기존의 전이 림프절 수에 의한 병기 분류에 비하여 좀더 객관적이고 더욱 정확하게 예후 를 예측할 수 있는 방법이 될 수 있을 것이다.
REFERENCES
1) Lee HJ, Yang HK, Ahn YO. Gastric cancer in Korea. Gast- ric Cancer 2002;5:177-82.
2) Kim JP, Kim YW, Yang HK, Noh DY. Significant prognos- tic factors by multivariate analysis of 3926 gastric cancer patients. World J Surg 1994;18:872-7; discussion 877-8.
3) Kooby DA, Suriawinata A, Klimstra DS, Brennan MF, Karpeh MS. Biologic predictors of survival in node-negative gastric cancer. Ann Surg 2003;237:828-35; discussion 835-7.
4) Isozaki H, Okajima K, Kawashima Y, Yamada S, Nakata E, Nishimura J, et al. Prognostic value of the number of metastatic lymph nodes in gastric cancer with radical surgery.
J Surg Oncol 1993;53:247-51.
5) Association KGC. Nationwide gastric cancer report in Korea.
J Korean Gastric Cancer Assoc 2002;2:105-14.
6) Kim YJ, Choi WY, Yuk JH, Oh ST, Park KC. Prognostic significance of group 2 lymph node metastasis in pT3pN1 gastric cancer patients. J Korean Gastric Cancer Assoc 2004;
4:32-5.
7) Jang SW, Kim CH, Kim SW, Song SK. Prognostic factors and survival rates of stage III gastric cancer patients after a gastrectomy. J Korean Gastric Cancer Assoc 2004;4:137-42.
8) Hyung WJ, Noh SH, Yoo CH, Huh JH, Shin DW, Lah KH, et al. Prognostic significance of metastatic lymph node ratio in T3 gastric cancer. World J Surg 2002;26:323-9.
9) Yoo CH, Noh SH, Kim YI, Min JS. Comparision of prognos- tic significance of nodal staing between old (4th edition) and new (5th edition) UICC TNM classification for gastric car- cinoma. World J Surg 1999;23:492-8.
10) Ichikura T, Tomimatsu S, Uefuji K, Kimura M, Uchida T, Morita D, et al. Evaluation of the new AJCC/UICC clas- sification of lymph node metastasis from gastric carcinoma in comparision with the Japanese classification. Cancer 1999;86:
553-8.
11) Kodera Y, Yamamura Y, Shimizu Y, Torii A, Hirai T, Ya- sui K, et al. The number of metastatic lymph nodes: a pro- mising prognostic determinant for gastric carcinoma in the latest edition of the TNM classification. J Am Coll Surg 1998;187:597-603.
12) de Manzoni G, Verlato G, Guglielmi A, Laterza E, Tomez- zoli A, Pelosi G, et al. Classification of lymph node metastases from carcinoma of the stomach: comparison of the old (1987) and new (1997) TNM systems. World J Surg 1999;23:664-9.
13) Kim SC, Yang HG, Kim YI, Kim JB. Comparative study between TNM staging according to number of metastatic lymph node UICC-TNM staging in stomach cancer. J Korean Surg Soc 1998;54:874-82.
14) Karpeh MS, Leon L, Klimstra D, Brennan MF. Lymph no- de staging in gastric cancer: is location more important than number? An analysis of 1,038 patients. Ann Surg 2000;
232:362-71.
15) Kranenbarg EK, Hermans J, van Krieken JHJM, van de Vel- de CJH. Evaluation of the 5th edition of the TNM clas- sification for gastric cancer: improved prognostic value. British Journal of Cancer 2001;84:64-71.
16) Bunt AMG, Hermans J, Smit VTHBM, van de Velde CJH, Fleuren GJ, Bruijn JA. Surgical/pathologic-stage migration confounds comparisons of gastric cancer survival rates be- tween Japan and Western countries. J Clin Oncol 1995;13:
5-7.
17) Lee JH, Kim SJ, Yu HJ, Yang HG, Kim JB. Ratio of invol- ved lymph nodes to resected lymph nodes as a prognostic factor of gastric cancer. J Korean Surg Soc 1998;55:76-83.
18) Inoue K, Nakane Y, Iiyama H, Sato M, Kanbara T, Nakai K, et al. The superiority of ratio-based lymph node staging in gastric carcinoma. Ann Surg Oncol 2002;9:27-34.
19) Kunisaki C, Shimada H, Nomura M, Matsuda G, Otsuka Y, Ono H, et al. Clinical impact of metastatic lymph node ratio in advanced gastric cancer. Anticancer Res 2005;25:1369-75.
20) American Cancer Society. AJCC Cancer Staging Manual. 5th ed. Philadelphia: Llppincott-Raven; 1997.
21) Makino M, Moriwaki S, Yonekawa M, Oota M, Kimura O, Kaibara N. Prognostic significance of the number of metastatic lymph nodes in patients with gastric cancer. J Surg Oncol 1991;47:12-6.
22) Kim DY, Kim HR, Kim YJ, Kim S. Clinicopathological
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ features of patients with Borrmann type IV gastric carcinoma.
ANZ J Surg 2002;72:739-42.
23) Adachi Y, Oshiro T, Sugimachi K. Tumor size as a simple prognostic indicator for gastric carcinoma. Ann Surg Oncol 1997;4:137-40.
24) Nakajo A, Natsugoe S, Ishigami S, Matsumoto M, Nakashima S, Hokita S, et al. Detection and prediction of micrometastasis
in the lymph nodes of patients with pN0 gastric cancer. Ann Surg Oncol 2001;8:158-62.
25) Yasuda K, Adachi Y, Shiraishi N, Inomata M, Takeuchi H, Kitano S. Prognostic effect of lymph node micrometastasis in patients with histologically node-negative gastric cancer. Ann Surg Oncol 2002;9:771-4.