좌관상동맥의
5
0
0
전체 글
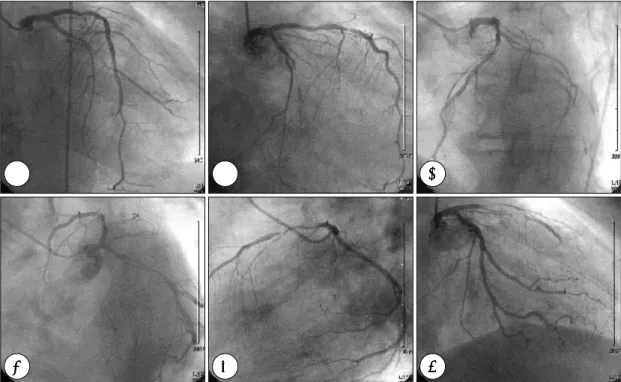
(2) 폐쇄가 될 정도의 연축이 온 것은 매우 드물다.8). 효소 검사도 정상이었다. 심전도에서는 1도 방실 차단. 저자 등은 이형 협심증의 임상적 진단하에 진단 목적. 외에 특이소견은 없었으며, 심초음파도 검사로 측정한. 의 관상동맥 조영술을 시행하던 도중 좌전하행지 및 좌. 구혈율은 62%이었으며, 벽운동 장애를 동반하지 않은. 회선지 관상동맥에 특별한 유발 원인이 없이 자발적으. 정상 좌심실 기능이었다.. 로 교대하여 폐쇄성 연축이 발생하였던 매우 드문 예를 경험하였기에 문헌고찰과 함께 보고하는 바이다.. 내원 2일 째 이형 협심증의 임상적 진단하에 관상동 맥 조영술을 시행하였다. 좌관상동맥 조영술에서 좌전 하행지는 정상 소견을 보였으나, 좌회선지는 근위부에. 증. 례. 서부터 폐쇄성 연축이 있었고 Thrombolysis In Myocardial Infarction flow I이었으며(Fig. 1A), 우전사. 54세 남자가 약 한달 전부터 주로 아침에 발생하는. 위 미부 촬영에서 좌회선지의 혈류는 더욱 감소되었다. 전흉부 동통을 주소로 내원하였다. 흉통의 양상은 짓누. (Fig. 1B). 좌전사위 두부 및 미부 촬영에서 좌회선지. 르는 듯 하였고 1분 내지 2분 동안 지속되다가 특별한. 의 폐쇄는 점차 호전을 보였고 혈류도 개선되어 TIMI. 치료없이 저절로 사라졌으며, 통증이 있을 때 발한을. Ⅱ 소견을 보였으나 좌전하행지는 혈류의 감소와 함께. 동반하였다. 과거력 및 가족력에서 특이 사항은 없었으. 혈관 내경이 감소되었다(Fig. 1C and 1D). 측면 촬영. 며, 사회력에서 하루 두 갑씩 20년간 흡연력이 있었다.. 에서 좌회선지의 내경 및 혈류는 정상화 되었으나 좌전. 혈압 130/90 mmHg, 맥박 80회/분, 체온 36.0℃, 호. 하행지의 내경은 점차 감소되었고 혈류도 TIMI Ⅱ로. 흡수 20회/분이었고, 이학적 진찰소견에서 특이사항은. 감소되었다(Fig. 1E). 우전사위 미부 재촬영에서 좌회. 없었다. 검사실 소견에서 혈액 검사, 생화학 검사 및 뇨. 선지는 정상을 보였으나 좌전하행지는 근위부에서부터. 검사 등에서 특이 사항은 없었으며, 혈중 지질 및 심근. 연축에 의한 완전 폐쇄를 보였다(Fig. 1F). 관상동맥. A. B. C. D. E. F. Fig. 1. Serial changes of left coronary artery during diagnostic coronary angiogram (CAG). Baseline CAG revealed occlusive spasm of left circumflex coronary artery (LCX) and no significant spasm in left anterior descending coronary artery (LAD)(A, B). LCX spasm relieved spontaneously, however, new occlusive spasm developed in LAD during procedure (C, D, E, F).. 872. Korean Circulation J 2000;30(7):871-875.
(3) A. B. C. Fig. 2. Serial changes of left coronary artery in right anterior oblique, caudal view during diagnostic coronary angiography, which revealed occlusive spasm in the left circumflex artery (LCx)(A). LCx spasm was relieved spontaneously, but occlusive spasm developed in left anterior descending artery (LAD)(B). LAD spasm was resolved after intracoronary injection of nitroglycerin (C).. A. B. Fig. 3. Right coronary angiogram of the patient revealed spasm in the branch of distal right coronary artery (arrow)(A), which was disappeared after intracoronary nitroglycerin (B).. 조영술 도중 환자는 평소 느끼던 흉통과 동일한 흉통을 호소하였으나, 심전도에서 변화는 없었다. 니트로글리. 고. 찰. 세린을 관상동맥내로 주입한 후 촬영한 우전사위 미부 촬영에서 좌전하행지 혈관 내경과 혈류는 정상화되었고. 관상동맥 연축은 정상 또는 거의 정상 관상동맥을 갖. 좌회선지의 혈류도 정상화되었다(Fig. 2C). 우관상동맥. 는 환자에서의 협심증이나 심근경색증 또는 급사의 요. 조영술에서는 원위부 우관상동맥에 전반적인 경도의 연. 인으로 생각되어지고 있으며 관상동맥 조영술 동안 그. 축이 관찰되었고 분지의 폐쇄가 관찰되었으나 관상동맥. 빈도는 0.26%에서 2.4%로 보고되어 왔다.1-7) Prinz-. 내로 니트로글리세린을 투여한 후 정상으로 회복되었다. metal 등은 이러한 심외막 관상동맥의 연축에 의해 야. (Fig. 3). 관상동맥 조영술을 위한 전체 투시 시간은 3.5. 기되는 심근 혈류의 감소에 기인하며 심전도상의 ST. 분이었으며, 심도자실에서 환자의 체류 시간은 총 45분. 절 상승과 연관된 안정시 흉통을 특징으로 하는 질환을. 이었고 관상동맥 조영술 후 정주 니트로글리세린을 유. 이형 협심증이라 하였다.9). 지하면서 병실로 전실시켰다.. 관상동맥 조영술 동안 연축은 흔히 관상동맥 도자의 기. 임상 경과:환자는 칼슘 길항제, nitrate 제제를 투. 계적 자극이나 약물 자극에 의해 일시적으로 관상동맥의. 여받은 후 퇴원하였고 외래에서 통원 치료 중이며, 6개. 내강 협착이 발생하는 의인성 연축(iatrogenic spasm)과. 월간 외래 추적결과 흉통의 재발은 없었다.. 특별한 유발 자극이 없이 가역적으로 관상동맥의 내강 873.
(4) Table 1. Conventional classification of spontaneous and iatrogenic spasm Iatrogenic. SPontaneous. Pharmacologic. Mechanical Catheter. Provocative agent. No ne. Ergonovine. Location. Variable. Variable. Near catheter tip. Symptoms. Angina (frequent). Angina (frequent). Asymptomatic. Electrocardiographic findings. Signs of ischemia. Signs of ischemia. Unchanged. 협착이 발생하는 자발성 연축(spontaneous spasm)으 8). 맥내로 nitrate 투여로 회복된 예를 보고한 바 있다.. Conti 등의 연구를 포함한 여러 연구들. Igarashi 등18)은 이러한 다발성 연축의 빈도를 43%. 은 이러한 자발성 연축이 이형 협심증의 병태생리에 중. 로 보고하였으며 흉통이 자주 발생하거나 투약 중단 후. 로 분류된다.. 7)10)11). 요한 역할을 한다고 보고하였다.. 도자에 의해 유. 24시간 이내에 자발적으로 흉통이 발생한 경우 또는. 발된 연축(catheter-induced spasm)은 도자 끝에 바. 진행성 협심증의 경우에 다발성 연축의 빈도가 높음을. 로 근접하여 발생하고 흉통이나 심전도의 변화없이 발. 보고하였다.. 생하며 도자를 빼거나 혈관확장제 주입으로 소실된다.. 관상동맥 조영술 도중에 발생하는 관상동맥 연축은. 반면 자발성 연축이나 약물 유발성 연축의 경우에는 도. 대개 관상동맥내로 혈관확장제를 투여하면 개선되지만,. 자 끝과 관상동맥 협착 사이에 어느 정도의 간격이 있. Ilia 등19)이나 Gaspardone 등20)은 혈관확장제의 투여. 으며 심근 허혈의 증상이나 징후가 동반되는 경우가 많. 에 의해 개선되지 않았지만, 다음날 시행한 관상동맥조. 다(Table 1).8). 영술에서 정상 소견을 보여 고정된 관상동맥 협착으로. 본 증례의 경우 관상동맥 조영술에서 도자 끝에 의한. 오인했던 도자 유발성 관상동맥 연축의 예를 보고한 바. 연축보다는 자발성 관상동맥 연축에 의한 협심증을 의. 있다. 따라서, 관상동맥 중재술을 시행하는 시술자는. 심할 수 있었으나, Heupler 등12)은 자발성 연축의 경. 불필요한 관상동맥 중재술을 피하기 위해서 고정된 병. 우에도 증상이 없고 심전도상 변화가 없이 발생할 수. 변과 연축 사이의 구별을 해야하며 혈관확장제의 투여. 있음을 보고하였다. 그러나, 도자에 의한 유발성 연축. 에도 반응이 늦거나 없을 수도 있을 가능성을 항상 생. 도 도자에서 떨어진 부위에 관상동맥 연축이 발생할 수. 각해야 한다고 생각되었다.. 13)14). 관상동맥 조영술 및 임상적. 이형 협심증은 칼슘길항제나 nitrate 제재 등에 대한. 특징으로 자발성 연축과 도자에 의한 유발성 연축을 완. 반응이 좋으며 선택적으로 교감신경의 알파수용체를. 전히 구분하기는 어렵다.. 차단하는 약제인 prazosin도 유용하나, 아스피린은 관. 있다는 보고가 있으며,. 이형 협심증에서 발생하는 관상동맥 연축은 대개 동맥. 상동맥에 확장 작용을 하는 prostacyclin의 합성을 억. 경화반의 근처에서 국소적으로 발생하며 단일 관상동맥. 제하여 증상을 악화시킬 수도 있다.15) 본 환자의 경우. 을 침범하는 경우가 많으나, 다혈관성 연축이 발생하거나. 에도 칼슘길항제와 nitrate 제제의 사용으로 증상의 발. 15). 한 혈관에서도 다발적으로 연축이 발생할 수도 있다.. 생 없이 외래 치료중이다.. 본 환자의 경우 좌회선지와 좌전하행지에 관상동맥 조영. 이형 협심증은 치료에 대한 반응이 좋아 장기적인 예. 술도중 순차적으로 폐쇄성 연축이 발생하였으며, 우관상. 후는 좋은 것으로 알려져 있으나 급사는 가장 중요한. 동맥의 원위부에도 경도의 연축이 발생하였다. 관상동맥. 임상적인 문제이다. 심장사는 이형 협심증 환자의 2%. 조영술 도중 본 환자의 경우처럼 여러 혈관에 폐쇄성 연. 에서 20%까지 발생하며 심장사의 41%에서 71%는. 16). 축이 발생한 경우는 매우 드물다. Mauser 등 은 심도. 갑작스럽게 발생한다. Yasue 등21)은 다혈관 연축이 불. 자의 자극에 의해 좌전하행지와 좌회선지에 동시에 폐쇄. 량 예후와 연관되어 있음을 보고하였고, Koyanagi 등. 17). 성 연축이 발생한 예를 보고하였으며, Guenot 등 은. 22). 두 개의 좌관상동맥에 동시에 발생한 자발성 폐쇄성. 높음을 보고하였다. 따라서 본 환자와 같이 다혈관 연. 연축에 의해 심정지가 발생하여 심폐소생술 및 관상동. 축을 갖는 환자는 칼슘길항제와 nitrate 제제 등으로. 874. 은 다혈관 연축을 갖는 환자에서 급사의 빈도가 더. Korean Circulation J 2000;30(7):871-875.
(5) 강력히 치료해야 하며 이러한 환자에서 약제의 중단이. 11) Roberts WC, Curry RC, Isner JM. Sudden death in Prin-. 급사의 발생에 중요한 역할을 하므로 장기간 동안 충분 히 약물 치료를 시행하는 것이 중요하리라 생각된다.. 12). 중심 단어:이형 협심증・자발적 관상동맥 폐쇄성 연축. 13). REFERENCES 1) Oliva PB, Potts DE, Pluss RG. Coronary artery spasm in Prinzmetal angina. N Engl J Med 1973;288:745-51.. 2) Yasue H, Touyama M, Kato H, Tanaka S, Akiyama F.. 3) 4) 5). 6) 7) 8). 9) 10). Prinzmetal’s variant form of angina as a manifestation of alpha-adrenergic receptor mediated coronary artery spasm. Am Heart J 1976;91:148-55. Maseri A, Mimmo R, Chierchia S, Marchesi C, Pesola A, L’Abbare A. Coronary artery spasm as a cause of acute myocardial ischemia in man. Chest 1975;68:625-33. Oliva PB, Breckinridge JC. Arteriographic evidence of coronary artery spasm in acute myocardial ischemia in man. Circulation 1977;56:366-74. Bertrand ME, Lablanche JM, Tilmant PY, Thieuleux FA, Delforge MG, Chahine RA. The provocation of coronary arterial spasm in patients with recent transmural myocardial infarction. Eur Heart J 1983;4:532-5. Chahine RA, Raizner AE, Ishimori T, Luchi RJ, Mclntosh HD. The incidence and clinical implications of coronary spasm. Circulation 1975;52:972-8. Conti CR, Feldman RL. Pepine CJ. Coronary artery spasm: Prevalence, clinical significance and provocative testing. Am Heart J 1982;103:584-7. Deckelbaum DI, Isner JM, Konstam MA, Salem DN. Catheterinduced versus spontaneous spasm: Do these coronary bedfellows deserve to be estranged? Am J Med 1985;79:1-4. Prinzmetal M, Kennamer R, Merliss R, Wade T, Bor N. A variant form of angina pectoris. Am J Med 1959;27: 375-88. Hillis LD, Braunwald E. Coronary artery spasm. N Engl J Med 1978;299:695-702.. 14) 15) 16) 17). 18). 19). 20). 21) 22). zmetal’s angina with coronary spasm documented by angiography. Am J Cardiol 1982;50:203-10. Heupler FA, Proudfit WL, Razivi M, Shirey EK, Greenstreet R, Sheldon WC. Ergonovine maleate provocative test for coronary artery spasm. Am J Cardiol 1978;41: 631-40. Schatz RE, Butman S. Catheter-induced nonproximal coronary artery spasm. Am J Cardiol 1984;53:352-4. Lafia P, Dincer B. Coronary artery catheter-induced spasm. Cathet Cardiovasc Diagn 1982;8:607-10. Braunwald E. Heart Disease. 5th ed. Philadelphia: W.B. Saunders Company;1997. p.1340-3. Mauser M, Dittmann H, Voelker W, Kuhlkamp V, Karsh KR. Occluding spasm of the total left coronary artery during coronary angiography (abst). Z Kardiol 1990;79:654. Guonet O, Pellet J, Terraube P, Grosclaude G, Couche L, Legrand M, et al;Coronary vasospasm: A cause of sudden death. Case report of reversible heart arrest with spontaneous coronary spasm documented by angiography (abst). Arch Mal Coeur Vaiss 1990;83:1859. Igarashi Y, Tamura Y, Tanabe Y, Fujita T, Hayashi S, Yamazoe M, et al. Clinical and angiographic characteristics of patients with multivessel coronary spasm in variant angina. Jpn Heart J 1994;35:419-30. Ilia R, Cafri C, Jafari J, Weinstein JM, Abu-Ful A, Battler A. Prolonged catheter-induced coronary artery spasm mimicking fixed stenosis. Cathet Cardiovasc Diagn 1997; 41:170-3. Gaspardone A, Tomai F, de Peppo AP, Chiariello L, Gioffre PA. Prolonged asymptomatic catheter-induced left and right coronary artery spasm resistant to high dose of intracoronary nitroglycerine (abst). Cardiologia 1992;37: 701. Yasue H, Takizawa A, Nagao M, Nishida S, Horie M, Kubota J, et al. Long-term prognosis for patients with variant angina and influential factors. Circulation 1988;78:1. Koyanagi S, Takeshita A, Nakamura M. Clinical characteristics of sudden cardiac death in patients with vasospastic angina. Jpn Cir J 1989;53:154.. 875.
(6)
수치

관련 문서
Coronary angiography revealed no fixed stenosis expect for coronary artery anomaly which showed same origin of right coronary artery (RCA) and left circumflex artery (LCX),
Right coronary artery (thin filled arrow), left main coronary artery (thick filled arrow), left anterior descending branch (thin empty arrow) and left circumflex branch (thick
IVUS, intravascular ultrasound; LCx, left circumflex artery; LAD, left anterior descending artery; RCA, right coronary artery; MI, myocardial infarction.. 관상동맥의
Selective coronary angiography through the left main coronary artery shows a tortuous vessel (arrow) arising from the proximal portion of the left circumflex artery, coursing
(A) Left coronary angiogram shows total occlusion of the left anterior descending artery and the left circumflex artery, (B) Right coronary angiogram shows critical diffuse stenosis
Unreported Coronary Artery Anomaly: Association of Right Coronary Artery and Circumflex Coronary Artery with Single Ostium Originate from High Left Anterior Aorta.. Ferhat
LAD: left anterior descending coronary artery, RCA: right coronary artery. LAO view of coronary angiography showed the LCx ori- ginating from the PL branch of RCA. LAO: left
perfusion defect at left lung. Coronary angiography showed coronary arterial fistula from left circumflex artery which flows to the left bronchial artery. A:RAO cranial view.
