Received: January 15, 2012 Revised: January 30, 2012 Accepted: February 14, 2012
∙Keun-Bae Lee, M.D., Ph.D.
Department of Orthopaedic Surgery, Chonnam National University Hospital, 42 Jebong-ro, Dong-gu, Gwangju 501-757, Korea Tel: +82-62-227-1640 Fax: +82-62-225-7794
E-mail: [email protected]
J Korean Foot Ankle Soc. Vol. 16. No. 1. pp.9-18, 2012
거골의 골연골 병변
전남대학교 의과대학 정형외과학교실 이 근 배
Osteochondral Lesions of the Talus
Keun-Bae Lee, M.D., Ph.D.
Department of Orthopaedic Surgery, Chonnam National University Medical School and Hospital, Gwangju, Korea
=Abstract=
Osteochondral lesions of the talus are isolated cartilage and/or bone lesions that are known cause of chronic ankle pain. They can occur as the result of a single acute ankle injury or from repetitive loading of the talus. Technical development in radiologic imaging and ankle arthroscopy have improved diagnostic capabilities for detecting osteochondral lesions. Characteristics which are important in assessing an osteochondral lesions include: the size, the type (chondral, subchondral, cystic), the stability, the displacement, the location, and the containment of lesion. Nonoperative treatment involving period of casting and non-weight- bearing is recommended for acute, non-displaced osteochondral lesions in select pediatric and adolescent patients. Operative treatment is recommended for unstable lesions or failed conservative management. Marrow stimulation techniques (abrasion chondroplasty, multiple drilling, microfracture), osteochondral autograft or allograft, autologous chondrocyte implantation, are frequently employed. The purpose of this article is to review the historical background, etiology, classification systems, diagnostic strategies, and to describe a systematic approach to management of osteochondral lesions of the talus.
Key Words: Talus, Osteochondral lesions, Arthroscopy
서 론
거골의 골연골 병변은 족근 관절의 급성 염좌 및 골절 환 자에서 흔히 발생할 수 있는 손상으로, 유병률은 전체 골절 의 0.09%, 모든 거골 골절의 약 1%로 알려져 있다.1,2) 거골
의 골연골 병변에 대한 최초의 보고는 1737년 Monro3)가 족근 관절로부터 유리체의 제거를 기술한 것이며, 외상에 의한 병변으로 생각하였다. 이후 1888년에 König4)가 슬관 절 내의 유리체를 골연골이 괴사되어 생긴 것이라는 의미 에서 골연골 염(osteochondritis dissecans)이라는 용어를 처음 사용하였으며, 거골의 골연골 병변에 대해서는 거골 골연골 결손(talar osteochondral defect), 경연골 거골 원개 골절(transchondral talar dome fractures), 골연골 체 (osteocartilagenous bodies), 관절서(joint mice) 등의 명칭 을 함께 사용하여 왔다. 그러나 거골의 골연골 병변이 외상 뿐만 아니라 무혈성 괴사에 의해서도 발생할 수 있다는 보 고에 따라 서로 다른 원인으로 발생한 병변일 가능성이 있
Table 1. Characteristics of Osteochondral Lesion of the Talus71)
1. Type of lesion
A. Chondral (cartilage only)
B. Chondral/subchondral (cartilage and underlying bone) C. Subchondral (intact overlying cartilage)
D. Cystic (>5 mm deep) 2. Stability of lesion
A. Stable B. Unstable
3. Displacement of lesion A. Displaced
B. Non-displaced 4. Location
A. Medial (anterior, central, or posterior) B. Lateral (anterior, central, or posterior) C. Central (anterior, central, or posterior) 5. Containment
A. Contained
B. Uncontained (shoulder lesion) 6. Size of lesion
A. Small (area<1.5 cm2 or greatest diameter<15 mm) B. Large (area>1.5 cm2 or greatest diameter>15 mm)
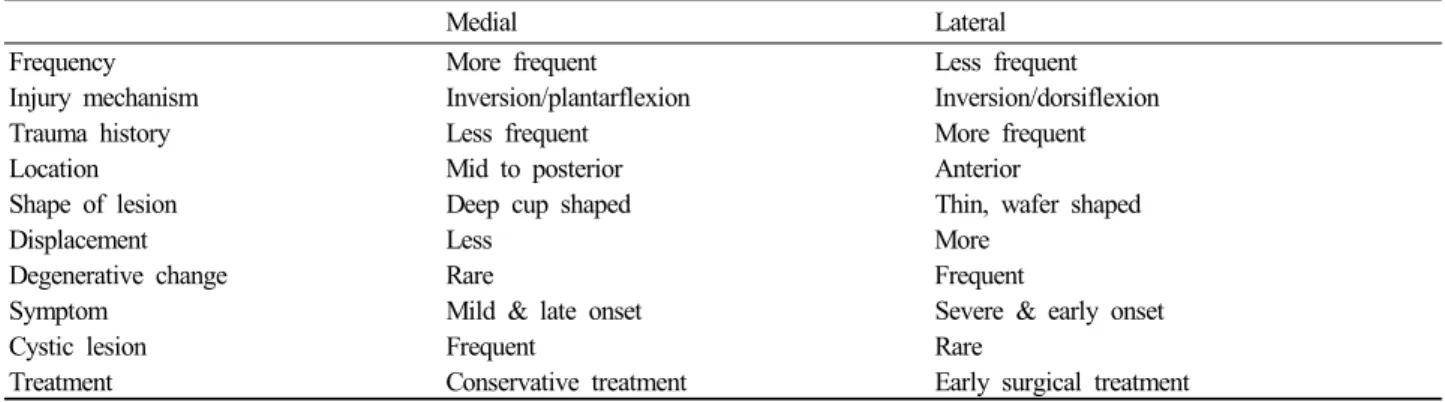
Table 2. Characteristics of Osteochondral Lesion of the Talus by Location
Medial Lateral
Frequency More frequent Less frequent
Injury mechanism Inversion/plantarflexion Inversion/dorsiflexion
Trauma history Less frequent More frequent
Location Mid to posterior Anterior
Shape of lesion Deep cup shaped Thin, wafer shaped
Displacement Less More
Degenerative change Rare Frequent
Symptom Mild & late onset Severe & early onset
Cystic lesion Frequent Rare
Treatment Conservative treatment Early surgical treatment
으므로 현재는 거골의 관절면이나 연골하 부위 유래의 병 변에 대하여 '거골의 골연골 병변(osteochondral lesions of the talus)'이라는 넓은 의미의 명칭이 널리 사용되고 있다.
최근에는 거골 골연골 병변의 특징을 크게 여섯 가지로 나 누어 분류하고 있다(Table 1). 일반적으로 거골의 골연골 병변은 대부분 내측에 발생하며, 주로 후방에 발생하고 모 양이 컵 형태로 깊은 반면, 외측의 경우는 외상과 관련이 많고 전방에 주로 발생하며 흔히 전위되어 보다 심한 증상 을 보인다(Table 2).2,5-7)
원 인
거골의 골연골 병변의 가장 흔한 원인은 외상이며 족근
관절 염좌 후 자주 발생한다. 1955년에 Bosien 등8)은 전체 족근 관절 염좌의 6.5%에서 골연골 병변이 관찰되었으며 대부분 10대부터 30대에서 발생한다고 보고하였다. 하지만 최근엔 스포츠 손상이 증가함에 따라 거골의 골연골 병변 의 유병률도 크게 증가하고 있으며 발생 연령대도 더 다양 해지는 추세이다.9,10) 1959년 Berndt와 Harty2)는 거골 골연 골 병변의 내측과 외측 부위 손상의 기전을 밝히고 내측 손 상은 내번 및 족저 굴곡에 의하여 생기며, 외측 손상은 내 번 및 족배 굴곡에 의해 발생한다고 보고하였다. 그 외의 선행 원인으로는 국소 무혈성 괴사, 만성 미세 손상, 내분비 계(부갑상선 기능저하증 또는 항진증)나 대사성 질환, 퇴행 성 관절 병변, 관절의 부정렬 및 유전적인 원인 등이 알려 져 있다.
분 류
거골의 골연골 병변은 단순 방사선 소견, 전산화 단층 촬영(CT), 자기 공명 영상(MRI) 및 관절경적 소견에 따라 분류할 수 있다. 1959년 Berndt와 Harty2)는 단순 방사선 소견에 따라 병변의 정도를 4단계로 분류하였으며, 이 분 류법은 지금까지도 이용되고 있다(Table 3, Fig. 1). 하지 만 단순 방사선 소견으로 병변의 단계를 정확히 구분하기 에는 한계가 있다. Loomer 등11)은 92명을 대상으로 한 연 구에서 골연골 병변의 50% 정도는 단순 방사선 소견상 발견되지 않았다고 하였다. 따라서 보다 정확한 진단을 위 하여 전산화 단층 촬영이나 자기 공명 영상 촬영 등이 필 요하며 관절경 시야에서 직접 골연골 병변의 상태를 검사 할 수도 있다. 현재는 전산화 단층 촬영이나 자기 공명 영 상, 관절경 등의 새로운 영상 기술이 발전, 도입됨에 따라 다양한 분류법들이 제시되어 사용되고 있다. 전산화 단층 촬영은 단순 방사선 촬영에 비해 우수하고 연골하 낭종을 관찰할 수 있다는 장점이 있다. 1990년 Ferkel 등12)은 전
Table 3. Berndt and Harty Classification System2) Stage Feature
I Focal compression of the subchondral bone (bone beneath the cartilage)
II Focal compression of the subchondral bone with partial detachment of a fragment of cartilage
III Focal compression of the subchondral bone with a fully detached fragment of cartilage still situated in place at the site of injury
IV Focal compression of the subchondral bone with a fully detached fragment of cartilage detached from the site of injury and floating in the joint space
Figure 1. Berndt and Harty classification system.2,72)
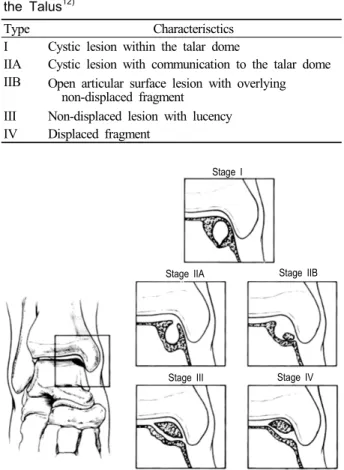
Table 4. CT Classification of Osteochondral Lesion of the Talus12)
Type Characterisctics
I Cystic lesion within the talar dome
IIA Cystic lesion with communication to the talar dome IIB Open articular surface lesion with overlying
non-displaced fragment III Non-displaced lesion with lucency IV Displaced fragment
Stage I
Stage IIA Stage IIB
Stage III Stage IV
Figure 2. CT classification of osteochondral lesion of the talus.12,73) 산화 단층 촬영에서 관절면의 상태와 연골하 낭종의 유무
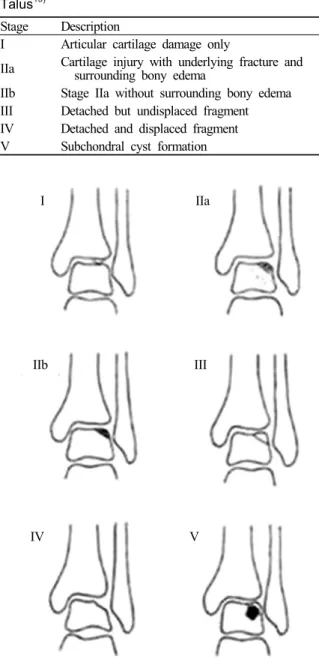
에 따라 4단계로 분류하고(Table 4, Fig. 2), 제I, II기는 보존적 치료를, 제III기와 IV기 그리고 보존적 치료에 실 패한 경우에서는 수술을 필요로 한다고 하였다. 거골의 골 연골 병변의 진단 및 분류에 가장 널리 쓰이는 자기 공명 영상 촬영은 병변의 범위를 파악하는 데 매우 유용하다. 1989년 Anderson 등13)이 MRI를 이용한 분류를 처음 제 시하였으며, 1999년에 Taranow 등14)이 MRI에 의한 분류 법을 발표하였고, 같은 해에 Hepple 등15)도 주변부의 부 종 유무에 따라 IIa기와 IIb기를 세분하는 MRI 분류법을 보고하였으며 현재 널리 이용되고 있다(Table 5, Fig. 3).
관절경적 소견을 이용한 분류법도 등장하였는데, 1986년 Pritsch 등16)은 관절경적 소견을 기초로 하여 제I기는 연 골 표면이 딱딱하며 빛나는 경우, 제II기는 연속성은 있으 나 부드러운 경우, 제III기는 연속성이 파괴되어 연골이 너덜거리는(frayed) 경우로 기술하였다. 그 후 1999년에 Ferkel과 Cheng17)은 다음과 같은 구체적인 관절경적 분류 법을 제시하였다(Table 6).
임상 증상 및 진단
1. 임상 증상
거골의 골연골 병변의 평균 발생 연령은 20-30대이며, 남 성에서 70% 정도 호발하고, 양측성으로 보고되는 경우도 10% 정도 된다.18) 대부분의 환자가 족근 관절 부위 외상의 과거력을 가지며,19) 증상으로 족근 관절의 부종, 동통, 잠김 현상 등을 보인다. 어느 순간 족근 관절의 심한 통증이 있 다가 자연적으로 좋아지는 증상이 반복되는 것이 특징적이
Table 5. MRI Staging of Osteochondral Lesion of the Talus15)
Stage Description
I Articular cartilage damage only
IIa Cartilage injury with underlying fracture and surrounding bony edema
IIb Stage IIa without surrounding bony edema III Detached but undisplaced fragment IV Detached and displaced fragment V Subchondral cyst formation
I IIa
IIb III
IV V
Figure 3. MRI staging of osteochondral lesion of the talus.15)
Table 6. Arthroscopic Staging of Osteochondral Lesion of the Talus17)
Stage Description
A Smooth/intact cartilage B Rough cartilage C Fibrillations/fissures
D Cartilage flap present or bone exposed E Loose, undisplaced osteochondral fragment F Displaced osteochondral fragment
다. 또한 증상은 오랜 보행이나 달리기, 점프 같은 충격량이 많은 운동으로 악화된다. 신체 검사상 병변 부위에 압통을 관찰할 수 있으며, 이외에도 족근 관절 운동 범위의 감소, 관절 내 삼출액 증가, 연발음, 불안정성 등을 관찰할 수 있 다.
2. 영상학적 검사
족근 관절의 단순 방사선 사진(체중 부하 전후방, 측면,
경사)을 시행하여 골절 유무를 확인하여야 한다. 내측 병변 은 후방에 위치하는 경우가 많으므로 족근 관절을 족저 굴 곡한 상태에서 전후면 촬영을 하면 더 잘 보이며, 외측 병 변은 전방에 위치하는 경우가 많으므로 족배 굴곡한 상태 에서 mortise 사진을 촬영하면 병변을 더 잘 관찰할 수 있 다. 그러나 단순 방사선 검사는 약 50% 정도에서 골연골 병변을 발견할 수 없으며,12) 골연골의 상태를 알기 어려우 므로 추가적인 검사가 필요하다. 전산화 단층 촬영은 병변 의 위치, 크기, 형태, 그리고 골연골의 전위 정도를 진단하 는 데 유용한 검사이지만, 관절 연골, 골 타박, 비전위성 병 변을 관찰하는 데는 한계가 있다.20) 골주사 검사는 단순 방 사선 사진에서 병변을 확인할 수 없는 경우 선별 검사로 이 용할 수 있으며 음성 예측치가 94%로 보고되어,21) 골주사 검사상 음성일 때 골연골 병변을 배제할 수 있는 장점이 있 다. 자기 공명 영상은 병변의 위치와 크기, 낭종의 유무, 안 정성을 평가하는 데 큰 도움이 되며, 관절 연골 및 연골하 골 병변 모두를 확인할 수 있고, 주변 연부 조직의 이상 소 견까지도 확인할 수 있다는 장점이 있으나,18) 골 병변의 정 도를 과대 평가할 가능성이 있다.
수술 전 평가 및 계획
관절 연골은 손상된 경우에 복원력이 매우 약하므로 손 상 받은 관절 연골은 제거 후 연골 결손 부위를 복구하여야 한다. 골연골 병변의 상태에 따라서 수술적 치료의 목표는 유리체를 제거할 것인지, 해부학적으로 큰 골편을 보전할 것인지, 섬유 연골의 재생을 유도할 것인지 또는 초자 연골 편 치환술을 시행할 것인지가 결정된다. 어떤 수술 방법을 선택하던지 수술 결과에 영향을 미치는 요소들로는 병변의 위치 및 크기, 전위 정도, 체중, 연령, 술 후 처치 등이 중요 한 것으로 알려져 있다.22) 또한 수술 방법을 결정하는 데 있 어 족근 관절의 불안정성 및 퇴행성 변화 유무, 관절의 부 정 정렬 등을 사전에 평가해 추가 술식이 필요한지를 결정 해야 한다. 단순 방사선 사진상 골연골 병변이 보이고 환자
Table 7. Surgical Treatment Options for Osteochondral Lesion of the Talus
Marrow stimulstion
A. Abrasion chondroplasty B. Curettage
C. Debridement and microfracture D. Drilling: antegrade or retrograde Osteochondral autograft
A. Single cylinder
B. Multiple cylinders (mosaicplasty) Osteochondral allograft
Autologous chondrocyte implantation (ACI)
Concomitant procedures (i.e. lateral ligament reconstruction, hindfoot realignment)
의 증상과 일치하면 컴퓨터 단층 촬영이나 자기 공명 영상 촬영이 권장되며 이는 삼차원적으로 병변의 위치와 크기, 낭종의 유무, 안정성등을 평가하는 데 큰 도움을 준다.
치 료
1. 비수술적 치료
무증상이거나 우연히 발견된 병변일 경우에는 비수술적 치료를 시행하여 볼 수 있다. 일반적인 방법은 석고 고정후 물리 치료를 시행하는 것이며, 연골 치유를 목적으로 경구 또는 주사용 연골 영양 제재(chondroprotective agents)를 사용할 수 있다. 경구 연골 영양 제재로는 glucosamine hy- drochloride, chondrotin sulfate, vitamin 등이 있으나 이들 제재들은 국소 연골 병변에는 효과가 없는 것으로 알려져 있다.23) 주사용 제재로는 hyaluronate 유도체가 있으며 초 기 증상이 있는 퇴행성 슬관절염에서 효과를 보고하고 있 으나 거골에 발생한 국소 연골 병변에 대한 치료 효과는 보 고된 바가 없다.
Berndt와 Harty2)는 비수술적 치료를 시행하였을 때 75%
에서 좋지 않은 결과를 보인다고 하였고 Flick과 Gould6)도 비슷한 결과를 보고하였다. Canale과 Belding24)은 I기와 II 기의 병변은 비수술적으로 치료해야 하며, III기는 수술적 치료 전 석고 고정을 시도해야 하고, III기 중 외측 병변 및 모든 IV기의 환자는 수술적 치료를 권장하였다. 그러나 최 근에는 관절경을 이용한 치료가 발전하면서 조기에 좀 더 적극적인 치료가 시도되고 있다. 방사선 소견으로는 II기로 분류되더라도 관절경하에서는 불안정한 경우도 있는데 이 러한 경우에는 III기에 준하여 치료하여야 한다. 또한 방사 선 사진에서는 발견되지 않고 자기 공명 영상에서 신호 강 도의 변화만 보이는 병변이라도 통증이 지속될 경우엔 좀 더 적극적인 관절경 검사가 필요할 수 있다.
2. 수술적 치료
급성 골절에서 전위된 작은 골연골편은 절제하고, 큰 골 연골편은 정복 후 고정하는 방법으로 치료한다. 만성적인 병변은 증세가 있는 경우에 치료를 한다. 이 경우 수술적 치료의 목적은 혈관이 없어 재생 능력이 떨어지는 관절 연 골을 제거하고 골연골 결손 부위에 재 혈관화를 시켜주어 치료를 도모하는 것이다.22,25)
외측 병변인 경우 주로 외상에 의해 발생하며 자연 치유 되는 경우가 드물고, 증세를 유발하는 경우가 많으므로 조
기에 수술적 치료를 하는 것이 좋다. 내측 병변인 경우에는 외상과 관계없는 경우가 많고, 증세를 유발하는 경우가 적 으며, 퇴행성 관절염을 일으키는 경우도 적으므로 증세를 일으킬 때까지 기다려 수술하는 것이 좋다.
수술적 치료 방법으로는 관절경을 이용한 소파술, 연마, 변연 절제술 및 다발성 천공, 미세 골절술 등의 골수 자극 요법이 있으며 연골 결손 부위를 초자연골 대신 섬유연골 로 복원시키는 방법들이다. 관절면의 초자연골을 복원시키 기 위한 방법으로는 자가 골연골편 또는 동종 골연골편 이 식법이나 자가 연골 세포 이식법 등이 있다(Table 7).
1) 관절경적 수술 방법
어떠한 수술 방법을 시행할 것인지를 결정하는 데 있어 서 관절경적 소견이 매우 중요하며, 관절경적 수술법은 수술 합병증이 적고 기능적 회복이 매우 빠르다는 장점이 있다. 일반적으로 전내방, 전외방 삽입구를 이용하며 경우에 따라 서 후내방 및 후외방 삽입구를 추가적으로 사용할 수 있다.
가) 연골 안정화/고정술
전위되지 않은 외상성 골연골편은 고정술을 시행하기에 적합한 경우로, 골편이 크면서 불안정성을 보이는 경우 변 연 절제술을 시행하는 것보다 고정술을 시행하는 것이 좋 다.26) 최근에는 polyglycolic acid (PGA)나 polylactic acid (PLLA) 같은 생체 흡수성 재료를 이용한 고정물을 사용하 기 때문에 금속 고정물의 제거를 위한 수술을 할 필요가 없 으며 좋은 결과가 보고되고 있다.27)
나) 역행성 천공술(retrograde drilling)
연골부위 손상 없이 연골하 병변만 존재하는 경우에는 연골의 손상을 줄이기 위해 순행성 천공술보다는 역행성 천공술을 시행하는 것이 좋다.14) 이때 주의할 점은 병변의
Figure 4. (A) Arthroscopic pho- tographs showing that micro- fractures were performed using arthroscopic awl. (B) Adequate bleeding occurred from the mi- crofracture holes after tourniquet release.30)
Figure 5. (A) T2-weighted coro- nal MR images showing medial osteochondral lesion with sub- chondral cyst. (B) Two osteochon- dral autograft cylinders were transplanted into the lesion.74)
A B
A B
감압도 중요하지만 관절 부위의 붕괴를 막기 위하여 골이 식술 또는 골이식 대체물(surgical-grade calcium sulfate 등)을 이용한 시술이 필요하다.28)
다) 변연 절제술(debridement), 소파술(curettage), 연마 (abrasion), 연골하 천공술(subchondral drilling), 미 세 골절술(microfracture)
골수 자극 치료방법은 골의 출혈을 일으켜 섬유 연골로 의 치유를 유도하는 방법으로 초자 연골이 아닌 섬유 연골 로 치유되어 역학적인 질은 떨어지지만 족근 관절로 통하 는 무게를 견디는 데는 충분한 것으로 보고되고 있다.29) 다 발성 천공술과 미세 골절술 중 어느 방법이 더 좋은가에 대 해서는 아직 논란이 있지만 천공술 시 발생하는 열에 의한 골세포의 손상과 병변에 수직으로 천공하기 위해서는 정상 내측과를 통해야 하는 등의 단점이 제기되어 미세 골절술 이 좀 더 선호되고 있는 추세이다(Fig. 4).25,30,31)
Flick과 Gould6)는 21명의 환자에서 변연절제술 및 미세
골절술을 시행한 결과에서 79%에서 우수, 21%에서 양호 의 결과를 얻었으며 불량의 결과는 없었다고 보고하였다. 또한 Chuckpaiwong 등32)은 미세 골절술을 시행한 105예 중 15 mm 미만의 병변 73예는 모두 결과가 좋았으나, 15 mm 이상의 32예에서는 1예만 결과가 좋았음을 보고하였 으며, 고령, 높은 체질량 지수, 외상의 과거력, 골극을 동반 한 경우 등에서 더 나쁜 결과를 보였다고 보고하였다. 연 골하 다발성 천공술에 대해서는 Angermann과 Jensen33)이 20명에서 유리된 골편을 제거하고 천공술을 시행하여 좋 은 결과를 얻었다고 보고하였다. 하지만 연골하골의 낭종 을 가진 만성 골연골 결손에서는 천공술이 덜 효과적이었 다는 보고도 있다.34) Second-look 관절경술은 연골 손상이 어느 정도 복구되어 있는지를 확인할 수 있는 방법으로, Lee 등29)은 미세 골절술 후 12개월에 시행한 second-look 관절경 소견상 약 40%에서 불완전한 연골 재생 상태를 보였 으나, 대부분의 환자에서 양호한 임상 결과를 보였다고 보고 하였다.
2) 조직 이식술
거골에 골연골을 이식하기 위하여, 병변 부위에 수직으 로 접근함이 필요하며, 이를 위해 다양한 내과 절골술의 방 법들이 보고되어 있으며,35-37) 거골 체 대부분의 부위에서 외과 절골술은 필요 하지 않다. Muir 등38)은 대부분의 거골 원개는 절골술이 없이도 수직으로 접근할 수 있다고 하였 으나, 내측 거골 원개의 17%, 외측 거골 원개의 20%에서 는 절골술 없이는 접근할 수 없다고 하였다.
가) 자가 골연골 이식술(autologous osteochondral graft, mosaicplasty)
자가 골연골 이식술은 동측의 슬관절에서 골연골을 떼어 내어 거골의 연골 결손 부위에 이식하는 방법으로 골수 자 극 치료를 시행한 경우에서 초자 연골이 아닌 섬유 연골로 치유되어 생역학적 특성이 떨어지는 단점을 극복할 수 있 는 방법으로 고안되었다(Fig. 5). 일반적으로 병변의 크기 가 1.5 cm2 이상으로 큰 경우나, 이전의 수술에 실패한 경 우, 또는 큰 연골하 골낭종을 가진 경우 등에서 시행된다.
하지만 건강한 슬관절에서 골 연골 편을 채취하여야 한다 는 점, 절골술을 필요로 하는 복잡한 술식, 슬관절과 족근 관절의 연골 두께의 차이가 나는 점 등의 단점이 있다.
Scranton 등39)은 직경 8-20 mm의 병변을 가진 50명의 환 자에 대하여 자가 골연골 이식 후 90%에서 술 후 양호한 결과를 보고하였고, Al-Shaikh 등40)도 평균 직경 12×10 mm의 병변을 가진 19명에서 술 후 AOFAS 88점의 우수 한 결과를 보고하였다.
1993년 Draper와 Fallet41)은 무릎의 연골 병변에 대해 여 러 개의 작은 이식을 하는 새로운 방법(mosaicplasty)을 보 고하였으며, 이 방법은 결손부의 모양에 맞추기가 쉽고 공 여부의 합병증을 줄일 수 있다는 장점이 있으나 이식 골연 골편 사이가 섬유성 조직으로 치유된다는 단점이 있다. Hangody 등42)은 직경 10 mm 이상의 거골 골연골 병변을 가진 36명의 환자에 대하여 대퇴골 내, 외측과의 골연골편 을 이용한 mosaicplasty 시행 후 2-7년 추시상 94% (34명) 에서 양호한 결과를 보고하였으며, 공여부의 합병증도 관찰 되지 않았다고 하였다.43) 다른 방법으로 Sammarco와 Makwana44)는 병변이 있는 거골 자체에서 골연골을 채취 하여 이식하는 방법을 보고하기도 하였다.
나) 동종 골연골 이식술(osteochondral allograft transplantation)
동종 골연골 이식술은 동종골로부터 큰 골연골편을 이식 하는 방법으로 골연골 병변이 매우 클 때 고려할 수 있다.
장점으로는 관절 표면을 복구할 수 있고, 공여부를 필요로 하지 않으며, 여러 개의 이식물 대신 하나의 골연골편을 사 용함으로써 이식 골연골편 사이의 섬유 연골로의 치유를 최소화할 수 있다는 점 등이 있으나, 면역거부반응 및 연골 세포의 생존율에서 제한점을 가지고 있다. Raikin45)은 6예 의 심한 골연골 결손에 대하여 동종 골연골 이식술을 시행 후 AOFAS 족관절-후족부 점수가 술 전 42점에서 술 후 86 점으로 향상되었음을 보고하였다. Gross 등46)도 거골의 골 연골 병변을 가진 9명의 환자에 대해서 동종 골연골 이식술 을 시행하여 추시상 6명의 환자에서 평균 11년의 생존을 보였고 3명의 환자는 유합술을 시행하였다고 보고하였다.
다) 자가 연골세포 이식(autologous chondrocyte transplantation)
자가 연골 세포 이식술은 슬관절의 연골을 일부 채취하 여 시험관 내에서 연골 세포를 분리한 후 3주간 배양 증폭 한 다음 거골의 골연골 결손부에 이식하는 방법으로 초자 연골로 재생시켜 줄 수 있는 방법으로 각광받고 있다. Giannini 등47)은 거골의 골 연골 병변에 대하여 자가 연골 세포 이식술을 시행하여 건강한 주변 연골을 닮은 새로운 초자 연골이 형성되는 것을 관찰하였다고 하였다. 자가 연 골 세포 이식술은 작은 연골 표본을 가지고 연골을 배양할 수 있으므로 공여부의 크기나 상태에 제한을 받지 않는다 는 장점이 있으나 2번의 수술이 필요하고 술기가 복잡하며 비용이 많이 들고, 장기간의 추시 결과가 없다는 단점이 있다.
3. 부가적인 치료/향후 치료 방향
거골의 골연골 병변에 대한 치료로는 물리치료를 포함한 비수술적 치료, 또는 병변의 크기, 환자의 성별, 나이 등을 고려한 수술적 치료가 널리 이용되고 있으나, 최근 새로운 치료법들이 소개되고 있다.
1) 점성 관절액 보충 치료(viscosupplementation therapy)
점성 관절액 보조물로 알려진 히알루론산(hyaluronic acid)의 관절 내 주사는 관절염이나 다른 관절 내에 발생하 는 다양한 병변에 치료를 위하여 그 사용이 증가하고 있는 추세이다. 다양한 연구에서 관절 내 연골 병변에 대하여 점 성 관절액 주사 치료는 좋은 결과를 보고하고 있으며, 또한 족근 관절 골관절염 환자에서도 안정성과 좋은 효과를 나 타내고 있다.48-50)
2) 전기/전자기 자극 치료(electrical/electromagnetic stimulation)
연골 손상의 치유에 있어서 전기 또는 전자기 자극 치료 의 효용성에 대해서는 아직 논란이 있으나, 일부 연구에서 는 이러한 치료가 형질전환성장인자-베타(TGF-β)나 다양 한 골형성 단백질(BMPs)의 분화에 기여한다고 보고되고
있다.51-55) 펄스 전자기장이 연골세포의 분화를 유도한다는
것이다. Benazzo 등56)은 동물 모델을 이용한 연구에서 자 가 골연골 이식 후 펄스 전자기 치료를 병행한 경우 골형성 및 이식물의 안정성이 향상되었다고 보고하였다.
3) 초음파 자극 치료(ultrasound stimualtion) 저강도의 초음파는 골과 연골의 치유를 촉진하고 유도하 는 것으로 알려져 있다.57-60) 최근 동물 모델을 이용한 연구 에서 양측 슬관절의 골연골 병변에 대하여 초음파 치료를 시행한 병변이 반대측에 비하여 더 우수한 결과를 보였다 는 보고가 있다.61) 그러나 이러한 초음파 치료의 효용성에 대해서는 더 많은 연구가 필요하다.
4) 중간엽 줄기세포(mesenchymal stem cells)
현재까지 골수에서 기원하는 중간엽 줄기세포를 이용한 연골 치료는 초기 단계에 있으나, 최근 동물 모델 연구들에 서 골연골 결손 부위에 지지체를 이용한 중간엽 줄기세포 이식의 성공적인 결과가 보고되고 있다.62-64)
5) 혈소판 풍부 혈장(platelet-rich plasma)
혈소판에는 다양한 성장 인자 및 형질전환성장인자-베타 (TGF-ß)와 같은 외인성 인자가 함유되어 있어 조직 재생 및 골 치유 과정에 관여하는 것으로 알려져 있다.65,66) 따라 서 연골 손상 이외에도 주관절의 상과염, 슬개건염 및 인대 손상, 근육 손상 등에도 이용되고 있다. 최근 자가 연골 세 포 이식과 혈소판 풍부 혈장을 함께 사용하여 더 성공적인 효과를 얻고자 하는 연구들이 진행되고 있다.67,68)
6) 네비게이션과 로봇의 이용(computer-aided navigation and robot-assisted surgery)
정형외과 영역에서 네비게이션 또는 로봇을 이용한 수술 이 점차 증가하고 있으며, 최근에는 족관절 영역에서도 네 비게이션 및 로봇을 이용한 수술적 치료가 시도되고 있다. 특히 병변이 작은 거골의 골연골 병변에서는 정확한 위치 파악과 최소 침습적 절개 및 술 후 결과를 극대화하기 위하 여 이러한 기술적 접근은 매우 유용해지고 있다.69,70)
요약 및 결론
거골 골연골 병변의 정확한 원인은 아직 불분명하지만 대부분 족근 관절의 외상 후에 이차적으로 발생한다. 거골 골연골 병변이 족근 관절 염좌 후에 발생 시 간과되는 경우 가 많으며, 증상이 없는 병변의 경우도 우연히 방사선적 검 사에서 발견된다. 최근 자기공명 영상 검사와 관절경술의 발달로 골연골 병변에 대한 진단은 더욱 정확해지고 있으 며, 치료 방법 또한 계속해서 진화하고 있다. 치료 방법을 결정하는 데 있어서는 병변의 크기와 위치, 병변의 안정성 및 전위정도, 연골하 낭종 유무, 환자의 나이와 활동 정도 등을 고려해야 한다. 지금까지 시행되고 있는 치료 방법들 의 전체적인 성공률은 양호한 편이지만, 지속적인 효과 및 안정성을 가지고 시행할 수 있는 방법의 확립을 위해서는 꾸준한 연구와 더 많은 증례의 결과들이 필요하다.
REFERENCES
1. Saxena A, Eakin C. Articular talar injuries in athletes: results of microfracture and autogenous bone graft. Am J Sports Med.
2007;35:1680-7.
2. Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 1959;41-A:
988-1020.
3. Monro A. Part of the cartilage of the joint separated and ossified. In: Medical essays and observations, 2nd ed. Edinburgh:
Ruddimans; 1737. 305.
4. König F. Uber freie Korper in den Gelenken [On the presence of loose bodies in joints]. Dtsch Z f Chir. 1888;27:90-109.
5. Clanton TO, DeLee JC. Osteochondritis dissecans. History, pathophysiology and current treatment concepts. Clin Orthop Relat Res. 1982;(167):50-64.
6. Flick AB, Gould N. Osteochondritis dissecans of the talus (transchondral fractures of the talus): review of the literature and new surgical approach for medial dome lesions. Foot Ankle. 1985;5:165-85.
7. Thompson JP, Loomer RL. Osteochondral lesions of the talus in a sports medicine clinic. A new radiographic technique and surgical approach. Am J Sports Med. 1984;12:460-3.
8. Bosien WR, Staples OS, Russell SW. Residual disability following acute ankle sprains. J Bone Joint Surg Am. 1955;37:
1237-43.
9. Schenck RC Jr, Goodnight JM. Osteochondritis dissecans. J Bone Joint Surg Am. 1996;78:439-56.
10. Tol JL, Struijs PA, Bossuyt PM, Verhagen RA, van Dijk CN.
Treatment strategies in osteochondral defects of the talar dome: a systematic review. Foot Ankle Int. 2000;21:119-26.
11. Loomer R, Fisher C, Lloyd-Smith R, Sisler J, Cooner T.
Osteochondral lesions of the talus. Am J Sports Med. 1993;21:
13-9.
12. Ferkel RD, Sgaglione NA, Del Pizzo W, et al. Arthroscopic treatment of osteochondral lesions of the talus: technique and results. Orthop Trans. 1990;14:172.
13. Anderson IF, Crichton KJ, Grattan-Smith T, Cooper RA, Braizer D. Osteochondral fractures of the dome of the talus. J Bone Joint Surg Am. 1989;71:1143-52.
14. Taranow WS, Bisignani GA, Towers JD, Conti SF. Retrograde drilling of osteochondral lesions of the medial talar dome.
Foot Ankle Int. 1999;20:474-80.
15. Hepple S, Winson IG, Glew D. Osteochondral lesions of the talus: A revised classification. Foot Ankle Int. 1999;20:789-93.
16. Pritsch M, Horoshovski H, Farine I. Arthroscopic treatment of osteochondral lesions of the talus. J Bone Joint Surg Am.
1986;68:862-5.
17. Ferkel RD, Cheng JC. Ankle and subtalar arthroscopy. In:
Kelikian AS, ed. Operative treatment of the foot and ankle.
Stamford (CT): Appleton & Lange; 1999. 321.
18. Chew KT, Tay E, Wong YS. Osteochondral lesions of the talus.
Ann Acad Med Singapore. 2008;37:63-8.
19. Santrock RD, Buchanan MM, Lee TH, Berlet GC.
Osteochondral lesions of the talus. Foot Ankle Clin. 2003;8:
73-90.
20. Ferkel RD, Flannigan BD, Elkins BS. Magnetic resonance imaging of the foot and ankle: correlation of normal anatomy with pathologic conditions. Foot Ankle. 1991;11:289-305.
21. Urman M, Ammann W, Sisler J, et al. The role of bone scintigraphy in the evaluation of talar dome fractures. J Nucl Med. 1991;32:2241-4.
22. Kumai T, Takakura Y, Higashiyama I, Tamai S. Arthroscopic drilling for the treatment of osteochondral lesions of the talus.
J Bone Joint Surg Am. 1999;81:1229-35.
23. Bourgeois P, Chales G, Dehais J, Delcambre B, Kuntz JL, Rozenberg S. Efficacy and tolerability of chondroitin sulfate 1200 mg/day vs chondroitin sulfate 3 x 400 mg/day vs placebo.
Osteoarthritis Cartilage. 1998;6 Suppl A:25-30.
24. Canale ST, Belding RH. Osteochondral lesions of the talus. J Bone Joint Surg Am. 1980;62:97-102.
25. Gobbi A, Francisco RA, Lubowitz JH, Allegra F, Canata G.
Osteochondral lesions of the talus: randomized controlled trial comparing chondroplasty, microfracture, and osteochondral autograft transplantation. Arthroscopy. 2006;22:1085-92.
26. O’Driscoll SW. The healing and regeneration of articular cartilage. J Bone Joint Surg Am. 1998;80:1795-812.
27. Larsen MW, Pietrzak WS, DeLee JC. Fixation of osteochondritis dissecans lesions using poly(l-lactic acid)/
poly(glycolic acid) copolymer bioabsorbable screws. Am J Sports Med. 2005;33:68-76.
28. Kennedy JG, Suero EM, O’Loughlin PF, Brief A, Bohne WH.
Clinical tips: retrograde drilling of talar osteochondral defects. Foot Ankle Int. 2008;29:616-9.
29. Lee KB, Bai LB, Yoon TR, Jung ST, Seon JK. Second-look arthroscopic findings and clinical outcomes after microfracture
for osteochondral lesions of the talus. Am J Sports Med.
2009;37 Suppl 1:63S-70.
30. Lee KB, Bai LB, Chung JY, Seon JK. Arthroscopic microfracture for osteochondral lesions of the talus. Knee Surg Sports Traumatol Arthrosc. 2010;18:247-53.
31. Jung HG, Carag JA, Park JY, Kim TH, Moon SG. Role of arthroscopic microfracture for cystic type osteochondral lesions of the talus with radiographic enhanced MRI support.
Knee Surg Sports Traumatol Arthrosc. 2011;19:858-62.
32. Chuckpaiwong B, Berkson EM, Theodore GH. Microfracture for osteochondral lesions of the ankle: outcome analysis and outcome predictors of 105 cases. Arthroscopy. 2008;24:106-12.
33. Angermann P, Jensen P. Osteochondritis dissecans of the talus:
long-term results of surgical treatment. Foot Ankle 1989;10:
161-3.
34. Kumai T, Takakura Y, Higashiyama I, Tamai S. Arthroscopic drilling for the treatment of osteochondral lesions of the talus.
J Bone Joint Surg Am. 1999;81:1229-35.
35. Oznur A. Medial malleolar window approach for osteochondral lesions of the talus. Foot Ankle Int. 2001;22:841-2.
36. Thordarson DB, Kaku SK. Results of step-cut medial malleolar osteotomy. Foot Ankle Int. 2006;27:1020-3.
37. Ziran BH, Abidi NA, Scheel MJ. Medial malleolar osteotomy for exposure of complex talar body fractures. J Orthop Trauma. 2001;15:513-8.
38. Muir D, Saltzman CL, Tochigi Y, Amendola N. Talar dome access for osteochondral lesions. Am J Sports Med. 2006;
34:1457-63.
39. Scranton PE Jr, Frey CC, Feder KS. Outcome of osteochondral autograft transplantation for type-V cystic osteochondral lesions of the talus. J Bone Joint Surg Br. 2006;88:614-9.
40. Al-Shaikh RA, Chou LB, Mann JA, Dreeben SM, Prieskorn D.
Autologous osteochondral grafting for talar cartilage defects.
Foot Ankle Int. 2002;23:381-9.
41. Draper SD, Fallet LM. Autogenous bone grafting for the treatment of talar dome lesions. J Foot Ankle Surg. 2000;39:
15-23
42. Hangody L, Ráthonyi GK, Duska Z, Vásárhelyi G, Füles P, Módis L. Autologous osteochondral mosaicplasty. Surgical technique. J Bone Joint Surg Am. 2004;86-A Suppl 1:65-72.
43. Hangody L, Kish G, Módis L, et al. Mosaicplasty for the treatment of osteochondritis dissecans of the talus: two to seven year results in 36 patients. Foot Ankle Int. 2001;22:552-8.
44. Sammarco GJ, Makwana NK. Treatment of talar osteochondral lesions using local osteochondral graft. Foot Ankle Int.
2002;23:693-8.
45. Raikin SM. Stage VI: massive osteochondral defects of the talus. Foot Ankle Clin. 2004;9:737-44.
46. Gross AE, Agnidis Z, Hutchison CR. Osteochondral defects of the talus treated with fresh osteochondral allograft transplantation.
Foot Ankle Int. 2001;22:385-91.
47. Giannini S, Buda R, Grigolo B, Vannini F. Autologous chondrocyte transplantation in osteochondral lesions of the
ankle joint. Foot Ankle Int. 2001;22:513-7.
48. Cohen MM, Altman RD, Hollstrom R, Hollstrom C, Sun C, Gipson B. Safety and efficacy of intra-articular sodium hyaluronate (Hyalgan) in a randomized, double-blind study for osteoarthritis of the ankle. Foot Ankle Int. 2008;29:657-63.
49. Pleimann JH, Davis WH, Cohen BE, Anderson RB.
Viscosupplementation for the arthritic ankle. Foot Ankle Clin.
2002;7:489-94.
50. Tytherleigh-Strong G, Hurtig M, Miniaci A. Intra-articular hyaluronan following autogenous osteochondral grafting of the knee. Arthroscopy. 2005;21:999-1005.
51. Akai M, Hayashi K. Effect of electrical stimulation on musculoskeletal systems; a meta-analysis of controlled clinical trials. Bioelectromagnetics. 2002;23:132-43
52. Bodamyali T, Bhatt B, Hughes FJ, et al. Pulsed electromagnetic fields simultaneously induce osteogenesis and upregulate transcription of bone morphogenetic proteins 2 and 4 in rat osteoblasts in vitro. Biochem Biophys Res Commun. 1998;250:
458-61.
53. Chang K, Chang WH, Huang S, Huang S, Shih C. Pulsed electromagnetic fields stimulation affects osteoclast formation by modulation of osteoprotegerin, RANK ligand and macrophage colony-stimulating factor. J Orthop Res. 2005;23:1308-14.
54. Lippiello L, Chakkalakal D, Connolly JF. Pulsing direct current-induced repair of articular cartilage in rabbit osteochondral defects. J Orthop Res. 1990;8:266-75.
55. Wang Z, Clark CC, Brighton CT. Up-regulation of bone morphogenetic proteins in cultured murine bone cells with use of specific electric fields. J Bone Joint Surg Am. 2006;88:1053-65.
56. Benazzo F, Cadossi M, Cavani F, et al. Cartilage repair with osteochondral autografts in sheep: effect of biophysical stimulation with pulsed electromagnetic fields. J Orthop Res.
2008;26:631-42.
57. Heckman JD, Ryaby JP, McCabe J, Frey JJ, Kilcoyne RF.
Acceleration of tibial fracture-healing by non-invasive, low-intensity pulsed ultrasound. J Bone Joint Surg Am. 1994;
76:26-34.
58. Khan Y, Laurencin CT. Fracture repair with ultrasound:
clinical and cell-based evaluation. J Bone Joint Surg Am.
2008;90 Suppl 1:138-44.
59. Ebisawa K, Hata K, Okada K, et al. Ultrasound enhances transforming growth factor beta-mediated chondrocyte differentiation of human mesenchymal stem cells. Tissue Eng.
2004;10:921-9.
60. Parvizi J, Parpura V, Greenleaf JF, Bolander ME. Calcium signaling is required for ultrasound-stimulated aggrecan synthesis by rat chondrocytes. J Orthop Res. 2002;20:51-7.
61. Jia XL, Chen WZ, Zhou K, Wang ZB. Effects of low-intensity pulsed ultrasound in repairing injured articular cartilage.
Chin J Traumatol. 2005;8:175-8.
62. Han SH, Kim YH, Park MS, et al. Histological and biomechanical properties of regenerated articular cartilage using chondrogenic bone marrow stromal cells with a PLGA scaffold in vivo. J Biomed Mater Res A. 2008;87:850-61.
63. Jeong WK, Oh SH, Lee JH, Im GI. Repair of osteochondral defects with a construct of mesenchymal stem cells and a polydioxanone/poly (vinyl alcohol) scaffold. Biotechnol Appl Biochem. 2008;49(Pt 2):155-64.
64. Kobayashi T, Ochi M, Yanada S, et al. A novel cell delivery system using magnetically labeled mesenchymal stem cells and an external magnetic device for clinical cartilage repair.
Arthroscopy. 2008;24:69-76.
65. Gandhi A, Bibbo C, Pinzur M, Lin SS. The role of platelet-rich plasma in foot and ankle surgery. Foot Ankle Clin. 2005;10:
621-37.
66. Joyce ME, Jingushi S, Scully SP, Bolander ME. Role of growth factors in fracture healing. Prog Clin Biol Res. 1991;365:
391-416.
67. Brehm W, Aklin B, Yamashita T, et al. Repair of superficial osteochondral defects with an autologous scaffold-free cartilage construct in a caprine model: implantation method and short-term results. Osteoarthritis Cartilage. 2006;14:1214-26.
68. Munirah S, Samsudin OC, Chen HC, Salmah SH, Aminuddin BS, Ruszymah BH. Articular cartilage restoration in load-bearing osteochondral defects by implantation of autologous chondrocyte-fibrin constructs: an experimental study in sheep. J Bone Joint Surg Br. 2007;89:1099-109.
69. Kendoff D, Geerling J, Mahlke L, et al. Navigated Iso- C(3D)-based drilling of a osteochondral lesion of the talus.
Unfallchirurg. 2003;106:963-47.
70. Kendoff D, Hüfner T, Citak M, et al. Navigated Iso-C3D-based percutaneous osteoid osteoma resection: a preliminary clinical report. Comput Aided Surg. 2005;10:157-63.
71. McGahan PJ, Pinney SJ. Current concept review:
osteochondral lesions of the talus. Foot Ankle Int. 2010;
31:90-101.
72. Coughlin MJ, Mann RA, Saltzman CL. Fractures and fracture-dislocations of the talus. Surgery of the foot and ankle.
8th ed. Philadelphia: Mosby; 2007. 2122.
73. Ferkel RD. Arthroscopic Surgery: The Foot and Ankle.
Philadelphia: JB Lippincott; 1999:145-69.
74. Lee KB, Yang HG, Moon ES, Song EK. Modified step-cut medial malleolar osteotomy for osteochondral grafting of the talus. Foot Ankle Int. 2008;29:1107-10.