INTRODUCTION
The extent of fatty degeneration is a useful marker to assess atrophy, function, and integrity of the rotator cuff muscles. Preoperative fatty degeneration of the rotator cuffs marks a poor prognosis after a rotator cuff repair;
because it is associated with a higher rate of re-tear. As well as being a prognostic marker, fatty degeneration is one of the prominent complications of rotator cuff tears, despite our lack of knowledge of the physiology of fatty degeneration [1]. Interestingly, Pfirrmann et al. [2]
found that individuals without cuff tears have slight fatty
degeneration around the rotator cuff muscles, showing the widespread prevalence of fatty degeneration even in the asymptomatic population. Regarding whether fatty degeneration improves or deteriorates after rotator cuff repairs, Goutallier et al. [3] found that fatty degeneration of the supraspinatus partially improves provided that the cuffs are anatomically repaired. Conversely, Gerber et al. [4] found that despite a successful cuff repair, fatty degeneration progressed. Further, they found a preoperative grade 3, 4 fatty degeneration of the infraspinatus muscles tends to lead to irreparability of the tears. Based on this observation, Gerber et al. [4] re- Background: To evaluate fatty degeneration and atrophy of rotator cuff muscles in patients with normal cuffs and in patients who received repairs of rotator cuff tears.
Methods: We chose 328 patients with normal cuffs, henceforth called the “normal group”. The normal group was subcategorized according to age. Further, we chose 41 patients with cuff tears, henceforth called the “cuff tear group”, who had received reparative surgeries. The cuff tear group was divided into 2 subgroups: a cuff “repaired group” that rotator cuff tears were successfully repaired and a “re-tear group” that cuff repairs were unsuccessful and led to a re- tear. The repaired group included 30 patients and the re-tear group included 11 patients. The radiological parameters (fatty degeneration and atrophy) and clinical outcomes (visual analogue scale, UCLA, Constant, and Oxford scores) were evaluated.
Results: We found that the extent of fatty degeneration and atrophy of the cuff muscles was irrespective of the aging process. Compared to the normal group, we found the cuff tear group had a significantly greater fatty degeneration and atrophy of the rotator cuff muscles. Within the cuff tear group, the re-tear group had a significantly more deteriorated fatty degeneration at the follow-up magnetic resonance imaging (MRI) than at the initial MRI (P = 0.024) and more muscle atrophy than the repaired group; there was no statistical significance. Although the clinical markers were more satisfactory in the repaired group than the re-tear group after surgery, there was no statistical significance.
Conclusion: Fatty degeneration and atrophy of the rotator cuff muscles were not affected by the normal aging process.
However, we found that fatty degeneration was accelerated following cuff tears even when the tear had been repaired.
Lastly, we found that a preoperative fatty degeneration of more than grade 3 was associated with a higher re-tear rate of the rotator cuffs.
Keywords: Rotator cuff; Tear; Fatty; Degeneration; Atrophy
Progression of fatty degeneration of rotator cuff muscles after cuff repairs
Young Lae Moon, Bo Seon Kim, Sang Ha Park
Department of Orthopaedics, Chosun University Hospital, Gwangju, Korea
Copyright © 2015 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received August 1, 2013; Revised September 19, 2014; Accepted October 1, 2014
Correspondence to: Young Lae Moon, Department of Orthopaedics, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, Gwangju 501-717, Korea. Tel: +82-62-220-3147, Fax: +82-62-226-3379, E-mail: [email protected]
Arthroscopy and Orthopedic Sports Medicine
AOSM
commend tendon transplants over arthroscopic repairs for muscle tears with fatty degeneration of greater than grade 3.
To gain a better understanding of the pathophysiology of rotator cuff tears, we performed two studies. First, we assessed the age-dependent development of fatty degeneration in asymptomatic individuals, i.e., those without rotator cuff tears, to see the effect of aging on fatty degeneration. Second, through shoulder magnetic resonance imaging (MRI) examination, we assessed the development of fatty degeneration in patients who received rotator cuff repairs by comparing the outcomes of those who showed a successful repair and those who showed re-tears.
METHODS
Study subjects and groups
Of the 2,207 patients, who were suffering from shoulder joint pain and had underwent diagnostic shoulder MRI examination from May 2005 to December 2011, we selected 328 patients (160 males and 168 females) conforming to our selection criterion. This group was called the “normal” group. The selection criterion was a radiological assessment of an intact rotator cuff with or without bicipital tendinitis or bone contusion. The exclusion criterion was a presence of shoulder fractures, dislocation, or infectious diseases. The normal group was subcategorized into age: 20 to 29 year olds as A1 subgroup (23 patients); 30 to 39 year olds as A2 subgroup (36 patients); 40 to 49 year olds as A3 subgroup (107 patients);
50 to 59 year olds as A4 subgroup (120 patients); 60 to 69 year olds as A5 subgroup (35 patients); and lastly 70 to 79 year olds as A6 subgroup (7 patients) (Table 1). The extent of fatty degeneration and atrophy of the rotator cuff muscles were tabulated according to these age groups and compared.
A total of 41 out of 384 patients who underwent repairs of their rotator cuff tears from September 2009 to December 2011 and were assessed over time using a high resolution MRI system (MAGNETOM Avanto; Siemens, Erlangen, Germany) were selected for this study. This group was called the “cuff tear group”. The cuff tear group was further subcategorized according to their treatment outcome: the
“repaired group” and the “re-tear group”. The 30 patients whose cuff tears were successfully repaired were placed in the repaired group (13 males and 17 females), whereas the 11 patients whose cuffs repair ended as a re-tear were placed in the re-tear group (4 males and 7 females). The change in the fatty degeneration and muscle atrophy of the rotator cuff muscles after their repair were measured (Table 2). This study was approved by the institutional review board of Chosun University Hospital (No. CHOSUN 2013-06-009-001).
Radiological assessment
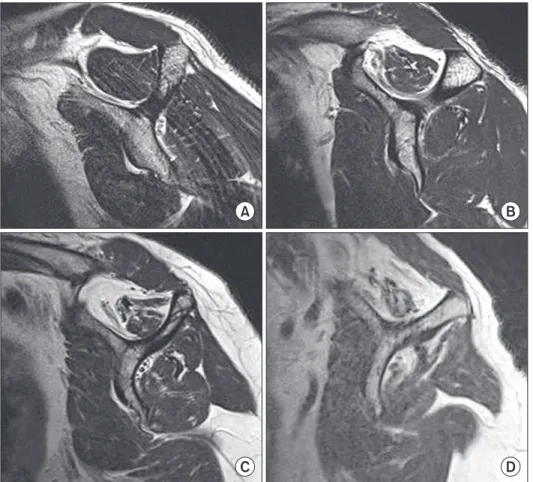
An oblique T1-weighted MRI radiographs of the shoul- ders from the sagittal view were taken. The scan wherein the scapular spine, scapular body, and the coracoid pro cess join to form a “Y”-shape was chosen for exami- nation. When a T1-weighted image was not useful, a fat suppressed T2-weighted image was used. Using the Goutallier classification [3], the extent of fatty degeneration in the supraspinatus muscle, infraspinatus muscle, and the subscapular muscle were assessed (Fig. 1). The classification system is as follows: grade 0, when no fatty cells are seen; grade 1, when a fatty streak is seen;
grade 2, when substantial fatty cells but still less in proportion than muscle cells is seen; grade 3, when equal proportions of fatty and muscle cells are seen; and lastly grade 4, when the proportion of fatty cells is greater than muscle cells. Once the three muscle types are classified accordingly to the Goutallier classification, a mean of the 3 values is taken to get the global fatty degeneration
Table 1. Demographic data of normal group (study #1)
Normal group Age (yr) Total patients
A1 A2 A3 A4 A5 A6 Sum
23.5 (21–29) 35.6 (30–39) 44.9 (41–49) 53.4 (50–58) 63.5 (60–67) 74.7 (71–78) 48.1 (21–78)
23 (20/3) 36 (19/17) 107 (42/65) 120 (53/67) 35 (24/11) 7 (2/5) 328 (160/168) A1, 20 to 29 yr group; A2, 30 to 39 yr group; A3, 40 to 49 yr group; A4, 50 to 59 yr group; A5, 60 to 69 yr group; A6, 70 to 79 yr group.
Values are presented as mean (range) or number (male/female).
Table 2. Demographic data of rotator cuff tear group (study #2) Tear group Repaired group Re-tear group P-value Number of patients
Male Female Age (yr) Male Female
Body mass index (kg/m2) Follow-up period (mo)
30 13 (43) 17 (57) 57.2 (42–66) 55.1 ± 8.87 58.8 ± 10.30 24.1 ± 2.86 23.6 ± 4.22
11 4 (36) 7 (64) 61.5 (54–68)
58.8 ± 8.12 63.0 ± 10.17 24.2 ± 3.32 24.2 ± 5.85
0.229
0.591 0.142 Values are presented as number only, number (%), mean (range), or mean ± standard deviation.
index (GFDI) [5]. To assess the proportion of fat and muscle, we drew hypothetical lines joining the upper and lower subscapular bone and the subscapular spine on an oblique sagittal T1-weighted image. If muscle mass extended over the border that the hypothetical lines make up, we considered it as no muscle atrophy, grade 0; if muscle mass superimposed the lines we considered as grade 1; if the muscle mass did not extend to the lines we considered as a moderate grade 2; and lastly if it was substantially far from reaching the lines, we considered it as a grade 3 fatty degeneration. The averages of these classification grades of the three muscles were taken (Fig. 2) [6].
Clinical assessment of outcomes
At the postoperative follow-up, the 41 patients of the cuff tear group who had received an arthroscopic repair of the rotator cuff were not only assessed by MRI examination, but also by the following clinical scores: visual analogue scale (VAS), UCLA, Constant, and Oxford scores. These clinical outcomes were compared between the repaired group and the re-tear group. The first follow-up was made
6 weeks postoperation and then at 3 month intervals.
Rotator cuff repairs
All symptomatic patients underwent arthroscopic repair of their rotator cuff tears. Under general anesthesia, anterior, posterior, and lateral portals were made around the affected tendon with the patient at lateral decubitus position. After an arthroscopic examination of the rotator cuffs, the humeral head was pretreated using a shaver and curette. Then, the ThRevo Suture Anchor (ConMed Linvatec, Largo, FL, USA) system was used to anatomically repair the torn rotator cuffs. If necessary, a synovectomy or a debridement was performed, and in the case of acromioclavicular joint tenderness, an acromioplasty was performed.
Rehabilitation
An abduction arm sling was fastened at around 20o for 2 weeks after the anatomic operation; and a normal arm sling for 4 weeks thereafter. From the next day of surgery, passive forward elevation, pendulum motion, and external rotation of the shoulders were performed to the
A B
C D
Fig. 1. Classification of fatty degene- ration using Goutallier’s grading systems.
Examples show each stage of fatty dege- neration in supraspinatus. (A) Grade 1, some fatty streaks in the muscle. (B) Grade 2, pronounced fatty infiltration, but muscle area still exceeding the fat area. (C) Grade 3, fat area equal to muscle area. (D) Grade 4, fat area exceeding the muscle area.
extent that the patient could tolerate. From 7 weeks after the operation, the patients began exercises to strengthen the rotator cuff muscles and scapular muscles. Further restrictions on daily activities were removed. The same rehabilitation procedure was performed irrespective of the patients’ tear size.
Statistical analysis
The change in fatty degeneration and muscle atrophy, deduced by shoulder MRI radiographs, were evaluated using the correlation analysis of one-way ANOVA (IBM
SPSS Statistics version 21.0; IBM Co., Armonk, NY, USA).
Spear man correlation coefficient was used to compare the values of the re-tear group. A P-value of less than 0.05 was considered as statistically significant.
RESULTS
Fatty degeneration and muscle atrophy in the normal group
In the normal group, we found that as age increased GFDI also increased. For example, GFDI increased by 0.01 in
A B
C D
Fig. 2. Grading for muscle atrophy ba- sed on a T1-weighted oblique sagittal magnetic resonance image. (A) Grade 0, supraspinatus tendons (SST) crossing a tangent (line) drawn between the superior borders of the scapular spine and the superior margin of the coracoid process. (B) Grade 1, SST did not extend to the tangent (line). (C) Grade 2, SST lies entirely below the tangent (line). (D) Grade 3, SST lies substantially far from tangent (line).
Table 3. Radiologic assessment of normal group (study #1)
Variable Normal group
A1 A2 A3 A4 A5 A6 P-value
Fatty degeneration (mm3) Supraspinatus Infraspinatus Subscapularis GFDI
Atrophy (%)
0.00 0.04 0.00 0.01 0.00
0.00 0.06 0.00 0.02 0.03
0.07 0.01 0.01 0.03 0.07
0.09 0.10 0.03 0.07 0.18
0.23 0.11 0.29 0.21 0.11
0.29 0.29 0.14 0.24 0.29
0.064 0.127 0.052 0.061 0.114 A1, 20 to 29 yr group; A2, 30 to 39 yr group; A3, 40 to 49 yr group; A4, 50 to 59 yr group; A5, 60 to 69 yr group; A6, 70 to 79 yr group.
GFDI, global fatty degeneration index.
the A1 subgroup (20–29 year olds) and by 0.24 in the A6 subgroup (70–79 year olds). However, the difference in the increase seen in the GFDI value between the two age groups was not statistically significant (P = 0.061). The fatty degeneration in muscle atrophy at the final follow-up was grade 0 for A1 and grade 0.29 for A6 subgroup. Again, there was no statistically significant difference between the results of the subgroups (P = 0.114) (Table 3).
Radiological assessment of the cuff tear group
We did not find statistically significant differences between the age, body mass index, duration of follow-up, and rotator cuff tear-size between the repaired group and the re-tear group (Table 2). We found the value of GFDI of the repaired group, which increased from a preoperative 0.59 to a postoperative 0.74, was not significant (P = 0.165).
However, we found that the same value for the re-tear group increased from 1.42 to 1.73 and was significant (P = 0.024). Although we found that muscle atrophy worsened
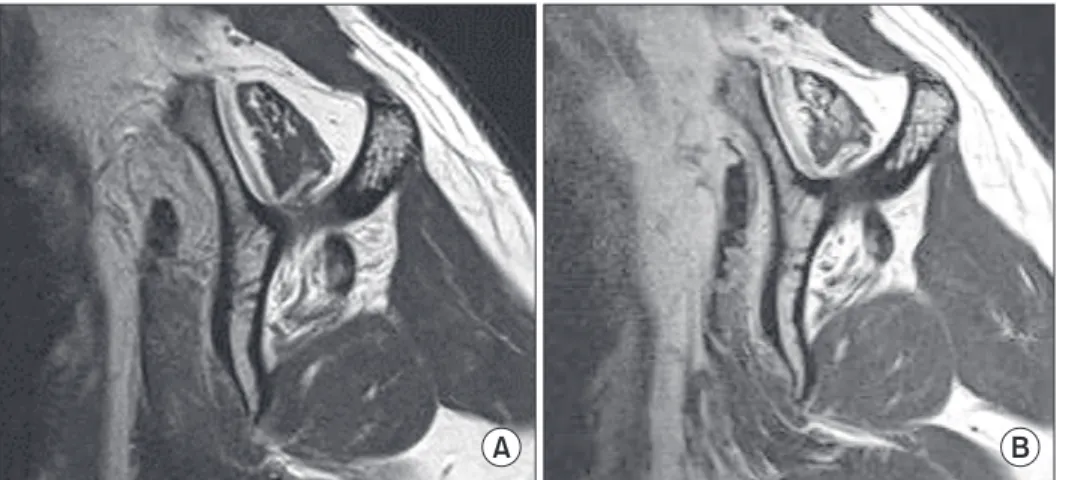
after surgery in both groups from their preoperative values, these changes were not statistically significant. In the repaired group this value altered from 0.54 to 0.62 (P = 0.337), and in the re-tear group, from 1.45 to 1.64 (P = 0.167) (Table 4). In the repaired group, we noted that one patient had a preoperative grade 3 fatty degeneration in the rotator cuff muscles (supraspinatus muscles). In the re- tear group, we noted that 4 cases had a preoperative grade 3 or higher degeneration (2 in supraspinatus muscles, 1 in infraspinatus muscles, and 1 in both supra- and infra- spinatus muscles). At the final MRI follow-up, we found that all 4 cases progressed to a grade 4 fatty degeneration and only one remained at the same classification (Fig. 3).
Subgroups (repaired and re-tear groups) of the cuff tear group
We found that the preoperative GFDI was greater by 0.83 in the re-tear group than the repaired group, and so was the postoperative GFDI but by 0.98. However, the differences between either the preoperative and postoperative GFDIs between the two groups did not show a statistically significant difference (P = 0.752, 0.092).
Similarly, we found that muscle atrophy was severer by 0.92 in the re-tear group than the repaired group
A B
Fig. 3. Oblique sagittal magnetic re- sonance imagings of 59 years old female before and after rotator cuff repair. Before repair of rotator cuff (A) shows fatty degeneration of supraspinatus (grade 2) and infraspinatus (grade 3) muscle and atrophy (grade 2). (B) After 18 months from the surgery, it shows progression of fatty degeneration of supraspinatus (grade 3) and infraspinatus (grade 4) muscles and atrophy (grade 3).
Table 4. Radiologic assessment of cuff tear group (study #2) Variable Preoperative Follow-up P-value Repaired group
Fatty degeneration Supraspinatus Infraspinatus Subscapularis GFDI Atrophy Re-tear group Fatty degeneration Supraspinatus Infraspinatus Subscapularis GFDI Atrophy
0.62 ± 0.65 0.69 ± 0.63 0.46 ± 0.66 0.59 ± 0.49 0.54 ± 0.78
1.45 ± 0.82 1.82 ± 0.87 1.00 ± 0.63 1.42 ± 0.54 1.45 ± 0.69
0.85 ± 0.80 0.77 ± 0.43 0.62 ± 0.65 0.74 ± 0.43 0.62 ± 0.77
2.09 ± 1.04 2.00 ± 1.00 1.09 ± 0.83 1.73 ± 0.65 1.64 ± 0.80
- - - 0.165 0.337
- - - 0.024 0.167 Values are presented as mean ± standard deviation.
GFDI, global fatty degeneration index; -, too low to be measured.
Table 5. Comparison of radiologic result between cuff tear group Variable Repaired group Re-tear group P-value Cuff tear size (mm)
Fatty degeneration #1 GFDI
Fatty degeneration #2 GFDI
Atrophy #1 Atrophy #2
16.8 ± 5.16 0.59 ± 0.49 0.74 ± 0.43 0.54 ± 0.78 0.62 ± 0.77
21.6 ± 5.22 1.42 ± 0.54 1.73 ± 0.65 1.45 ± 0.69 1.64 ± 0.80
0.464 0.752 0.092 0.531 0.614 Values are presented as mean ± standard deviation.
GFDI, global fatty degeneration index.
preoperatively, and by 1.02, postoperatively. Again, these differences were statistically insignificant (P = 0.531, 0.614) (Table 5).
Clinical outcomes of the cuff tear group
After the rotator cuff repairs, a re-tear group showed a better clinical outcome than the repaired group in terms of VAS, UCLA, and Constant score, but these differences were not statistically significant (Table 6).
DISCUSSION
Fatty degeneration of rotator cuffs is considered as one of the complications of cuff tears. Rotator cuff tears are thought to elicit substantial physiological and functional changes in the muscle and to cause muscle atrophy induced by axial and transverse reductions in tensile strength [7]. Microstructural changes such as, the de crease in the number and length of muscle fibers may occur [8]. As the number of myofibrillar proteins decrease the overall muscle mass may decrease [9]. If this continues, muscle may undergo fibrosis and accumulate fat around the region of the atrophied muscle [10]. In general, fatty degeneration of the rotator cuffs refers to a chronic condition of a cuff tear-induced intramuscular, fibrotic, fat build-up and muscle atrophy [11].
Pfirrmann et al. [2] found that a small degree of fatty degeneration occurs even in individuals without tendon tears. Through MRI radiographs, they found that around 13.7% of asymptomatic individuals in their sample of subjects had fatty degeneration of the supraspinatus muscle. However, the presence of rotator cuff tears has been shown to deteriorate fatty degeneration. In our study, we found that the extent of fatty degeneration in asymptomatic individuals was not correlated with age, implying that cuff tear over age may be the influencing marker for fatty degeneration.
Fatty degeneration complicates rotator cuff repairs as, for example, severe fatty degeneration negatively influences clinical outcomes [12,13]. Gladstone et al.
[14] even used fatty degeneration as a marker of poor prognosis. Although the influence of fatty degeneration on treatment outcome is widely agreed, whether fatty degeneration improves or deteriorates after cuff repairs remains controversial.
Using rabbits, Rubino et al. [15] found that if rotator cuff tears are left untreated then fatty degeneration progresses and if treated, progression of fatty degeneration is prevented [16]. Song et al. [17] also found that in indivi- duals whose rotator cuffs of preoperative grade 2 had been repaired, fatty degeneration improved in 2 patients and muscle atrophy improved in 3 patients. In this study, we also saw in two 50 year old patients fatty degeneration improved by around a third of a grade.
Conversely, Liem et al. [18,19] and others have shown that despite a rotator cuff repair, intramuscular fatty degeneration could not be reversed but deteriorated instead [14]. In agreement with this finding, except in the two patients who showed a slight improvement, we found all patients in both the repaired and re-tear groups showed a progression in fatty degeneration. We found that preoperative GFDI of 1.424 in the re-tear group significantly deteriorated to 1.727 postoperatively. But this large shift in GFDI is probably influenced by having 4 cases of grade 3 or above fatty degeneration within this group pushing the mean GDFI higher. Gerber et al. [4]
systemically selected the treatment modality on the basis of the patient’s extent of fatty degeneration. For example, when patients had fatty degeneration of the infraspinatus muscles of grade 3 or above, grades associated poor pro- gnosis, tendon transplant was used. In support of this, within the patients who had a preoperative grade 3 or above fatty degeneration in our study, 4 out of 5 patients had a re-tear.
Postoperation, the GFDI value and the extent of muscle atrophy was greater in the re-tear group than the repair group; but these differences were not statistically significant. A study with a larger sample size is needed to improve the study.
According to Park et al. [20], a fatty degeneration at a one-year follow-up does not lead to a poor prognosis on the outcome of the rotator cuff repair. Although the clinical outcomes (VAS, UCLA, Constant, and Oxford scores) were improved in the repaired group than the re- tear group, we found no statistically significance in these differences. This means that as long as the repair is done properly to prevent a re-tear, then a satisfactory clinical outcome can be attained.
Table 6. Clinical assessment of cuff tear group
Scores Repaired group Re-tear group P-value VAS
UCLA Constant Oxford
2.38 ± 1.56 28.84 ± 5.49 75.69 ± 14.2 43.69 ± 5.31
3.54 ± 2.01 24.81 ± 8.62 66.36 ± 20.6 37.63 ± 10.86
0.140 0.473 0.626 0.522 Values are presented as mean ± standard deviation.
VAS, visual analog scale.
Limitations to our study exist. First, although the indivi- duals were designated as “asymptomatic” because a radiologist could not detect peculiarities from the shoulder MRI radiographs, technically, they are not completely asymptomatic. Some patients have abnormalities such as bicipital tendinitis and notably, these patients were initially advised to take MRIs because of shoulder pain.
Secondly, only a small number of patients who underwent rotator cuff repairs underwent follow-up shoulder MRI examination. A small sample size inevitably weakens the statistical power of the study. Thirdly, as the rotator cuff muscles became atrophied in the symptomatic group, the muscles may translate medially on the scapular Y view, which can cause radiologist to overestimate the extent of fatty degeneration and muscle atrophy. Therefore, prospective studies using a greater number of case studies must be performed to overcome such limitations.
We found that fatty degeneration, as a complication of rotator cuff tear, did not increase with age as long as the rotator cuff remained intact. However, in individuals with
a history of rotator cuff tears, even a re-tear, irrespective of whether the tear has been repaired or not, fatty degene- ration progressed significantly more in these patients than patients who had never had a rotator cuff tear.
Furthermore, we found that a preoperative grade 3 fatty degeneration of the rotator cuff muscle is indicative of a postoperative re-tear.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
This work was supported by the ICT R&D program of MSIP/IITP [2014(2014-044-065-003), Development of Human Digital Multimedia Contents Generation and Service Technology].
1. Kang JR, Gupta R. Mechanisms of fatty degeneration in massive rotator cuff tears. J Shoulder Elbow Surg 2012;21:175-80.
2. Pfirrmann CW, Schmid MR, Zanetti M, Jost B, Gerber C, Hodler J.
Assessment of fat content in supraspinatus muscle with proton MR spectroscopy in asymptomatic volunteers and patients with supraspinatus tendon lesions. Radiology 2004;232:709-15.
3. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res 1994;(304):78-83.
4. Gerber C, Wirth SH, Farshad M. Treatment options for massive rotator cuff tears. J Shoulder Elbow Surg 2011;20(2 Suppl):S20-9.
5. Goutallier D, Postel JM, Gleyze P, Leguilloux P, Van Driessche S.
Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg 2003;12:550-4.
6. Morag Y, Jacobson JA, Miller B, De Maeseneer M, Girish G, Jamadar D. MR imaging of rotator cuff injury: what the clinician needs to know. Radiographics 2006;26:1045-65.
7. Ward SR, Sarver JJ, Eng CM, et al. Plasticity of muscle archi- tecture after supraspinatus tears. J Orthop Sports Phys Ther 2010;40:729-35.
8. Jamali AA, Afshar P, Abrams RA, Lieber RL. Skeletal muscle response to tenotomy. Muscle Nerve 2000;23:851-62.
9. Safran O, Derwin KA, Powell K, Iannotti JP. Changes in rotator cuff muscle volume, fat content, and passive mechanics after chronic detachment in a canine model. J Bone Joint Surg Am 2005;87:2662-70.
10. Nakagaki K, Ozaki J, Tomita Y, Tamai S. Fatty degeneration in the
supraspinatus muscle after rotator cuff tear. J Shoulder Elbow Surg 1996;5:194-200.
11. Burkhart SS. The principle of margin convergence in rotator cuff repair as a means of strain reduction at the tear margin. Ann Biomed Eng 2004;32:166-70.
12. Goutallier D, Postel JM, Lavau L, Bernageau J. Impact of fatty degeneration of the suparspinatus and infraspinatus msucles on the prognosis of surgical repair of the rotator cuff. Rev Chir Orthop Reparatrice Appar Mot 1999;85:668-76.
13. Oh JH, Kim SH, Ji HM, Jo KH, Bin SW, Gong HS. Prognostic factors affecting anatomic outcome of rotator cuff repair and correlation with functional outcome. Arthroscopy 2009;25:30-9.
14. Gladstone JN, Bishop JY, Lo IK, Flatow EL. Fatty infiltration and atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with poor functional outcome. Am J Sports Med 2007;35:719-28.
15. Rubino LJ, Stills HF Jr, Sprott DC, Crosby LA. Fatty infiltration of the torn rotator cuff worsens over time in a rabbit model.
Arthroscopy 2007;23:717-22.
16. Rubino LJ, Sprott DC, Stills HF Jr, Crosby LA. Fatty infiltration does not progress after rotator cuff repair in a rabbit model.
Arthroscopy 2008;24:936-40.
17. Song JS, Chun JM, Park JB, Chung SJ, Kim TH. Analysis of the change in fatty degeneration of the rotator cuff and its influence on the outcome of rotator cuff repair. J Korean Orthop Assoc 2009;44:556-64.
18. Liem D, Bartl C, Lichtenberg S, Magosch P, Habermeyer P. Clinical outcome and tendon integrity of arthroscopic versus mini-open
REFERENCES
supraspinatus tendon repair: a magnetic resonance imaging- controlled matched-pair analysis. Arthroscopy 2007;23:514-21.
19. Liem D, Lichtenberg S, Magosch P, Habermeyer P. Magnetic resonance imaging of arthroscopic supraspinatus tendon repair.
J Bone Joint Surg Am 2007;89:1770-6.
20. Park JB, Jung HJ, Ahn TS, Chun JM. Follow-up results in patient with the progressive fatty degeneration of the rotator cuff. J Korean Orthop Assoc 2011;46:28-34.