Clinical Significance of National Institutes of Health-Chronic Prostatitis Symptom Index Pain Score in Patients with Benign Prostatic Hyperplasia
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
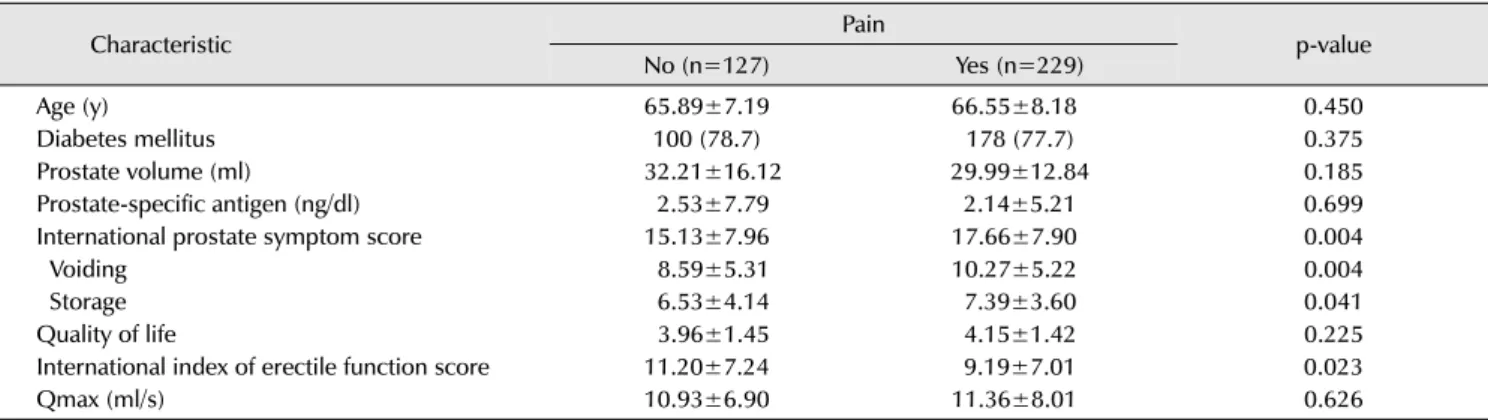
IPSS, International Prostate Symptom Score; QoL, quality of life; Qmax, maximum flow rate; PVR, postvoid residual urine volume; BPVP, bipolar plasma vaporization of
The new NIH classification for category III further defined these men as either category IIIA (inflammatory) or IIIB (noninflammatory) on the basis of the presence of
We investigated the statistical sig- nificance of an increased PUA on the International Prostate Symptom Score (IPSS) in men with benign prostatic hyperplasia (BPH)/lower urinary
Purpose: We examined the correlation between body mass index (BMI) as a marker of obesity and prostate-specific antigen (PSA), prostate volume (PV), and International Prostate
TSH: thyroid stimulating hormone, LUTS: lower urinary tract symptoms, BPH: benign prostatic hyperplasia, TPV: total prostate volume, IPSS: international prostate symptom score,
The nternational Prostate Symptom Score (IPSS), quality of life (QoL), International Index of Erectile Function (IIEF), and Male Sexual Health Questionnaire Ejaculation Function
The National Institutues of Health chronic prostatitis symptom index: development and validation of a new outcome measure. Chronic Prosatitis Collaborative Research
After 12 weeks, naftopidil 50 and 75 mg groups showed significant improvements in IPSS scores (total, obstructive/irritative subscores, QoL score) and Qmax from baseline. In both
