서론
CMV의 감염은 고형장기 이식 및 골수이식 후 1-6 개월사이에 흔히 발생하며, virus가 면역억제제 사 용으로 인해 재활성화 되는 것으로, 면역이 억제된 환자에서는 감염 발생시 CMV 질환으로 진행하여 심각한 morbidity와 mortality를 나타낸다.
1)CMV 감염의 고위험군은 혈청학적 양성 공여자(donor)와 음성 수여자(recipient) (D+/R-), 노인, Antilymphocyte
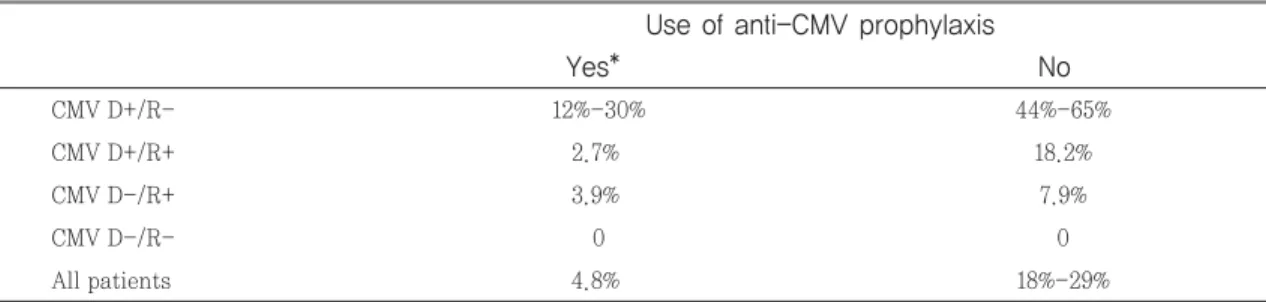
antibodies 투여 환자, 면역억제제 과량 투여 환자 이며, 효과적인 예방요법이 시행되지 않았을 경우 일반적으로 이식 후 3개월이내에 CMV 감염 증상이 나타나며, 발생 빈도는 공여자와 수혜자의 혈청학적 상태에 따라 다르다(Table 1).
2)간이식환자의 18%- 29%에서 CMV질환이 나타나는 것으로 보이며, 특 히 CMV D+/R- 환자에서 44%-65%로 가장 높다.
CMV감염의 일반적인 임상증상은 발열, 골수억제, 기관 침습성 질환 등이며, 이식 거부반응으로 진행
장기이식환자의 CMV 감염의 예방 및 치료 경향 및 항바이러스 제제에 의한 부작용 관리
서울대학교병원 약제부
약물부작용모니터링 특수연구회 운영위원, 장기이식 특수연구회 운영위원
특집
CMV D+/R- 12%-30% 44%-65%
CMV D+/R+ 2.7% 18.2%
CMV D-/R+ 3.9% 7.9%
CMV D-/R- 0 0
All patients 4.8% 18%-29%
Use of anti-CMV prophylaxis
Yes* No
Table 1. Estimated incidence of CMV disease during the first 12 mo after liver transplantation
D: Donor; R: Recipient. �Most cases occur as delayed-onset CMV disease. CMV disease occurs rarely during prophylaxis with oral valganciclovir.
Data adapted from[3,4,5].
할 수 있어 면역이 억제된 환자에서는 생명을 위협할 수 있다. 본서에서는 장기이식환자의 CMV 감염에 대한 예방 및 치료 경향에 대한 자료를 검토하고, CMV 감염에 사용하는 항바이러스 제제에 의한 부작 용을 예방하기 위한 방안에 대하여 살펴보고자 한다.
본론
1. CMV 감염의 예방 및 치료 경향 (1) 예방(prevention)
1) universal prophylaxis와 preemptive 치료 장기이식 후 CMV 감염을 적절하게 예방하는 것은 이식 후 장기 생존에 있어서 매우 중요하다. CMV 감염을 예방하는 방법은 universal prophylaxis와 preemptive therapy로 나누어 볼 수 있다. Universal prophylaxis는 CMV replication 여부와 관계 없 이 이식 후 일정 기간 동안 항바이러스제를 투약하는 방법이며, preemptive therapy는 정기적인 검사를
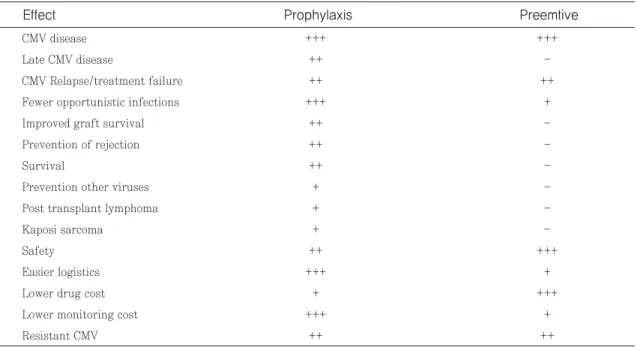
통해 CMV replication이 확인된 경우 치료를 시작 하는 방법이다. Universal prophylaxis는 CMV 감 염 여부와 관계없이 항바이러스제를 투약하기 때문 에 D+/R-와 같은 고위험군의 CMV 질환 예방으로 서 유용하지만, 약물의 비용이 많이 들며, 예방 요법 종료 후 delayed CMV infection의 발생 빈도가 다 소 높은 단점을 가지고 있다. Preemptive therapy 의 경우 정기적인 검사를 통해 감염이 확인된 환자들 을 치료하므로 약제 비용은 절감되는 장점이 있지만, 검사가 외래를 통해 이루어지는 경우, 환자의 순응도 에 따라 효과를 예측하기 어렵다는 단점이 있다. 또 한, 치료를 시작하는 cut-off에 대한 기준이 마련되 어있지 않아 각 센터마다 다른 기준을 둘 수 밖에 없 는 문제점도 있다. 그러나 두 방법에서 CMV 질환의 발생 빈도는 유의한 차이를 보이지 않는다는 결과가 보고되어 있으므로, 환자의 혈청학적 상태에 따라 적 합한 방법을 적용하는 것이 필요하다. 두 가지 예방 요법의 장단점을 비교한 내용은 다음의 표에 나타내 었다(Table 2).
3)2) 예방요법에 사용하는 항바이러스 제제
3)-5)CMV disease +++ +++
Late CMV disease ++ -
CMV Relapse/treatment failure ++ ++
Fewer opportunistic infections +++ +
Improved graft survival ++ -
Prevention of rejection ++ -
Survival ++ -
Prevention other viruses + -
Post transplant lymphoma + -
Kaposi sarcoma + -
Safety ++ +++
Easier logistics +++ +
Lower drug cost + +++
Lower monitoring cost +++ +
Resistant CMV ++ ++
Effect Prophylaxis Preemtive
Table 2. Comparison of known benefits and limitations of prophylaxis versus preemptive therapy
+ 는 evidence의 크기, -는 evidence가 없음(modified from Kotton et al.)
일반적으로, CMV 예방에 효과가 있는 약물은 세 가지로 IV ganciclovir, 경구용 valganciclovir, 경 구용 ganciclovir가 있다. Universal prophylaxis 에서는 세 가지 제제 모두 효과가 유사한 것으로 알 려져 있다. 다만, 경구용 gancyclovir의 경우 bioavailability가 낮은 약물로 투약 용량이나 횟수 를 높여 (1 g tid) 사용해야 하는 단점이 있어 최근에 는 valganciclovir의 사용량이 늘고 있는 추세이다.
Preemptive therapy는 증식된 virus를 치료하는 개념으로, 국내에서 치료 목적으로서는 IV ganci- clovir 제제만 유효한 것으로 승인을 받았다. 다만, VICTOR trial로 알려진 연구에서는, 경구 제제인
valganciclovir와 IV ganciclovir의 CMV 감염 치 료 반응의 차이가 통계적으로 유의하지 않다는 결론 을 보여, 향후 경구 제제인 valganciclovir가 CMV 감염 치료에 사용되는 것이 기대되는 상황이다.
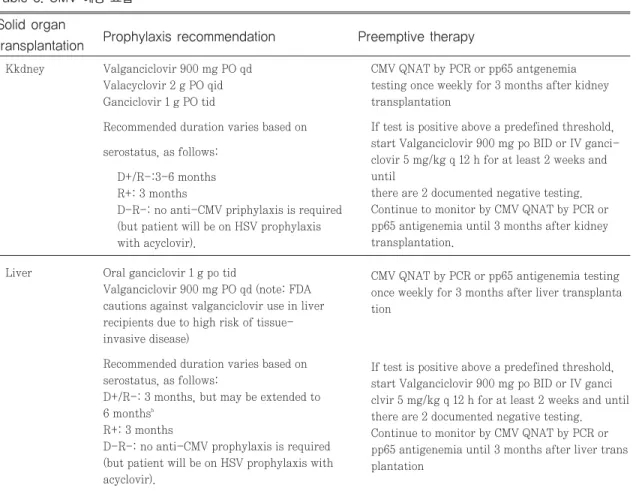
Foscarnet과 cidofovir는 심각한 부작용 때문에 적 극적인 모니터링이 필요하며 IV제제만 있어 ganci- clovir에 내성을 보이는 등 매우 드문 경우에만 사용 된다. Acyclovir와 valaciclovir도 CMV 예방으로 고려해 볼 수 있으나, 높은 내성률을 보이고 있어 최 근의 가이드라인에서는 1차 선택약으로 추천하지 않 는다(Table 3).
Kkdney Valganciclovir 900 mg PO qd Valacyclovir 2 g PO qid Ganciclovir 1 g PO tid
Recommended duration varies based on serostatus, as follows:
D+/R-:3-6 months R+: 3 months
D-R-: no anti-CMV priphylaxis is required (but patient will be on HSV prophylaxis with acyclovir).
Liver Oral ganciclovir 1 g po tid
Valganciclovir 900 mg PO qd (note: FDA cautions against valganciclovir use in liver recipients due to high risk of tissue- invasive disease)
Recommended duration varies based on serostatus, as follows:
D+/R-: 3 months, but may be extended to 6 months
bR+: 3 months
D-R-: no anti-CMV prophylaxis is required (but patient will be on HSV prophylaxis with acyclovir).
Solid organ
Prophylaxis recommendation Preemptive therapy transplantation
Table 3. CMV 예방 요법
CMV QNAT by PCR or pp65 antgenemia testing once weekly for 3 months after kidney transplantation
If test is positive above a predefined threshold, start Valganciclovir 900 mg po BID or IV ganci- clovir 5 mg/kg q 12 h for at least 2 weeks and until
there are 2 documented negative testing.
Continue to monitor by CMV QNAT by PCR or pp65 antigenemia until 3 months after kidney transplantation.
CMV QNAT by PCR or pp65 antigenemia testing once weekly for 3 months after liver transplanta tion
If test is positive above a predefined threshold, start Valganciclovir 900 mg po BID or IV ganci clvir 5 mg/kg q 12 h for at least 2 weeks and until there are 2 documented negative testing.
Continue to monitor by CMV QNAT by PCR or
pp65 antigenemia until 3 months after liver trans
plantation
3) 백신과 면역학에 의한 맞춤형 예방
CMV에 대한 백신요법은 CMV 음성인 경우 가장 중요한 면역 반응을 유발시킬 수 있으며, 혈청 CMV 양성인 수여자의 경우에도 면역을 증강시킬 수 있는 방법으로 이에 대한 결과에 관하여 최근 활발한 연구 가 진행되고 있다.
(2) 치료
6)-9)CMV 감염의 치료 약제는 항바이러스 제제, 면역 억제제 감량, CMV면역글로불린 사용 등 3가지가 있 다. 가장 일반적인 항바이러스 치료제는 경구용 valganciclovir 또는 IV ganciclovir, 경구용 ganciclovir이다. 국내에서는 경구용 ganciclovir 는 생체이용율이 매우 낮아 흡수율이 높은 prodrug SAE, n(%)
All patients D+/R+
D-/R+
Patients with leukopenia, n(%) All patients
D+/R+
D-/R+
Patients with neutropenia, n(%) All patients
D+/R+
D-/R+
Opportunistic infections, n(%) All patients
D+/R+
D-/R+
Posttransplant diabetes, n(%) All patients
D+/R+
D-/R+
Unresponsive CMV infection, n(%) All patients
D+/R+
D-/R+
Deaths, n(%) All patients D+/R+
D-/R+
Variable
83 (56.8) 46 (51.1) 37 (66.1)
52 (35.6) 37 (41.1) 15 (26.8)
14 (9.6) 9 (10.0) 5 (8.9)
46 (31.5) 24 (26.7) 22 (39.3)
5 (3.4) 3 (3.3) 2 (3.6)
2 (11.8) 2 (12.5) 0 (0.0)
2 (1.4) 2 (2.2) 0 (0.0)
General prophylaxis using oral valganciclovir ITT/safety population (N=146)
88 (58.7) 46 (59.0) 42 (58.3)
40 (26.7) 27 (34.6) 13 (18.1)
8 (5.3) 4 (5.1) 4 (5.6)
51 (34.0) 23 (29.5) 28 (38.9)
1 (0.7) 0 (0.0) 1 (1.4)
15 (18.5) 13 (21.0) 2 (10.5)
2 (1.3) 0 (0.0) 2 (2.8)
Preemptive therapy using oral valganciclovir ITT/safety population (N=150)
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05
>0.05 P Table 4. 경구용 Valganciclovir를 사용하여 Prophylaxis와 Preemtive 치료를 시행한 환자에서 발생한 부작용
SAE, serious asvers event; ITT, intent-to-treat; D+, donor CMV lgG positive; D-, donor CMV lgG negative; R+, recipient CMV lgG positive;
leukopenia ≤3500/μL; neutropenia, < 750μL; all P values are determined using the Fisher exact test.