bloodresearch.or.kr Blood Res 2019;54:229-240.
Letters to the Editor 231
AuthorsÊ Disclosures of Potential Conflicts of Interest No potential conflicts of interest relevant to this article were reported.
REFERENCES
1. Kyle RA, Garton JP. The spectrum of IgM monoclonal gammop- athy in 430 cases. Mayo Clin Proc 1987;62:719-31.
2. Owen RG, Parapia LA, Higginson J, et al. Clinicopathological cor- relates of IgM paraproteinemias. Clin Lymphoma 2000;1:39-43.
3. Lin P, Hao S, Handy BC, Bueso-Ramos CE, Medeiros LJ.
Lymphoid neoplasms associated with IgM paraprotein: a study of 382 patients. Am J Clin Pathol 2005;123:200-5.
4. Witzig TE, Maurer MJ, Stenson MJ, et al. Elevated serum mono- clonal and polyclonal free light chains and interferon inducible protein-10 predicts inferior prognosis in untreated diffuse large B-cell lymphoma. Am J Hematol 2004;89:417-22.
5. Lenz G, Staudt LM. Aggressive lymphomas. N Engl J Med 2010;362:1417-29.
6. Huan W, Xiao-ge Z, Mei X, Zhao W. Nodal marginal zone B-cell lymphoma with monoclonal IgM: 2 cases report and review of literatures. J Leuk Lymphoma 2009;18:160-2.
Bone marrow metastasis of small cell lung carcinoma with spontaneous tumor lysis syndrome without hepatic metastasis at diagnosis: first case report in Korea and review of literature
TO THE EDITOR: Tumor lysis syndrome (TLS) is a severe metabolic and electrolytic disturbance caused by rapid lysis of neoplastic cells, and resulting in various end-organ damages. TLS is frequently encountered in tumors with high cell turnover and growth rates such as hematologic malignancies including acute leukemias, Burkitt lymphoma, and high-grade lymphomas, and is commonly observed in these patients after administration of induction chemo- therapy, radiotherapy, or cytolytic antibody therapy [1, 2].
TLS unrelated to therapy is defined as spontaneous TLS (STLS), which can be observed in patients with the afore- mentioned hematologic malignancies, but the incidence of STLS is lower than that of TLS associated with prior therapy [3, 4]. TLS is also rarely encountered in patients with solid cancers. STLS in small cell lung carcinoma (SCLC) was first reported in 2008, and since then, only five other cases have been reported up to present time [3-7]. We report here a case of STLS associated with bone marrow (BM) metastatic SCLC without hepatic metastasis at diagnosis, and to our best knowledge, this is the first case report of STLS with BM metastatic SCLC in Korea.
A 71-year-old man visited our institution in January 2019 with increased nodule size in the right lower lobe (RLL) of the lungs. The RLL nodule was initially found five years prior, but its size had decreased at follow-up and it was regarded as an inflammatory nodule. Computed tomography (CT) showed the development of ill-defined ground-glass opacities in the right upper lobe of the lungs accompanied by multiple lymphadenopathies in the right supraclavicular, prevascular, upper paratracheal, both lower paratracheal, subcarinal, and left paraesophageal lymph nodes, but evi- dence of hepatic or renal metastasis of solid cancer was not found. The hemogram and peripheral blood smear results of the patient at the first visit were as follows: white blood cells, 6.09×109/L; hemoglobin, 10.3 g/dL; and platelets, 7.0×109/L. The complete blood cell differential count results of the patient at the first visit were as follows: meta- myelocytes, 3%; band neutrophils, 12%; segmented neu- trophils, 44%; lymphocytes, 33%; monocytes, 7%; basophils, 1%; and the presence of nucleated red blood cells (nRBCs) with a frequency of 5 nRBCs/100 white blood cells. At initial workup, the patient showed increased inorganic phos- phate (6.9 mg/dL, reference range, 2.9–4.3), uric acid (11.9 mg/dL, reference range, 2.1–7.4), fibrinogen degradation product (81.99 g/mL, reference range, <5.00), D-dimer (6.53 g/mL, reference range, <0.50), lactate dehydrogenase (3922 IU/L, reference range, 106–230), and creatinine (1.77 mg/dL, reference range, 0.60–1.50) levels and prolonged prothrombin time (13.3 s, reference range, 9.3–13.2). The patient also showed normal potassium (4.10 mM/L, reference range, 3.50–5.30) and calcium (8.6 mg/dL, reference range, 7.8–10.0) levels and a decreased fibrinogen (146.0 mg/dL, reference range, 200.0–400.0) level. At the previous visit to another hospital 2 months prior, the patient showed normal uric acid (3.7 mg/dL, reference range, 2.5–8.3) and creatinine (0.78 mg/dL, reference range, 0.6–1.2) levels. For the pathologic diagnosis, endobronchoscopic ultrasound- guided transbronchial needle aspiration (EBUS-TBNA) and liquid-based aspiration cytology from the lymph nodes, BM aspiration, and biopsy were performed.
The BM aspiration showed hypocellular marrow due to dilution by peripheral blood with infiltration of small to medium-sized neoplastic cells at a frequency of 56.0%, which showed deeply stained nuclei, finely dispersed nu- clear chromatin without distinct nucleoli, scanty amount of cytoplasm, and frequent nuclear moulding defined as conformity of adjacent cell nuclei to one another (Fig. 1A–C).
BM biopsy showed hypercellular marrow (cellularity 90%) with proliferation of neoplastic cells in a diffuse and patched pattern accompanied with frequent nuclear moulding (Fig.
1D–F). Subsequently performed immunohistochemical (IHC) staining in BM biopsy sections showed the presence of neoplastic cells with positivity for cluster of differ- entiation (CD)56 (Fig. 1G), cytokeratin (Fig. 1H), and chro- mogranin (Fig. 1I). Both CD3 and CD20 IHC stains showed the presence of a few reactive T and B lymphocytes, without evidence of neoplastic lymphoid cell infiltrations. Based
Blood Res2019;54:229-240. bloodresearch.or.kr
232 Letters to the Editor
Fig. 1. Bone marrow aspiration, biopsy, and immunohistochemical stain results of the patient. The bone marrow aspiration (A–C) showed hypocellular marrow due to dilution by peripheral blood with increased infiltration of small to medium-sized neoplastic cells, which showed deeply stained nuclei, finely dispersed nuclear chromatin without distinct nucleoli, scanty amount of cytoplasm, and frequent nuclear moulding defined as conformity of adjacent cell nuclei to one another (Wright stain, ×400). The bone marrow biopsy (D–F) showed hypercellular marrow with proliferation of neoplastic cells in a diffuse and patched pattern accompanied by frequent nuclear moulding (Hematoxylin and Eosin stains, ×200 in D, ×200 in E, ×400 in F). Subsequently performed immunohistochemical stains showed the presence of neoplastic cells with positivity for CD56 (G, ×400), cytokeratin (H, ×400), and chromogranin (I, ×400).
on these results, the diagnosis of BM metastasis of SCLC was made. Liquid-based aspiration cytology showed the presence of neoplastic cells favoring metastatic SCLC, and lymph node specimens obtained from EBUS-TBNA also showed positivity for CD56, cytokeratin, and chromogranin IHC stains, which corresponded with the IHC staining re- sults of the BM biopsy sections. Based on these results, the pathologic diagnosis of SCLC was confirmed. Since the patient showed hyperuricemia (11.9 mg/dL) and hyper- phosphatemia (6.9 mg/dL), and these results fulfilled the diagnostic criteria for laboratory TLS [1, 8], which requires two or more of four metabolic abnormalities (defined as hyperuricemia ≥8.0 mg/dL or >25% increase from base- line, hyperkalemia ≥6.0 mM/L or >25% increase from baseline, hyperphosphatemia ≥4.49 mg/dL or >25% in- crease from baseline, and hypocalcemia ≤7.0 mg/dL or
>25% decrease from baseline) within 3 days before or up to 7 days after induction of therapy, our patient was finally diagnosed with BM metastatic SCLC with STLS; he also showed a typical laboratory finding of disseminated intra- vascular coagulation. At present, our patient is awaiting palliative chemotherapy for SCLC.
Although TLS is frequently observed in hematologic ma- lignancies, such as acute leukemias or high-grade lympho- mas, the incidence of TLS associated with solid tumors re-
mains relatively low because they have such a low pro- liferative index, and a few case reports of TLS associated with solid cancer support this speculation [3, 9]. In addition, STLS in solid tumors is an extremely rare situation and has been reported in only a few cases [3]. Although only a few cases of STLS in SCLC have been reported previously [3-7], SCLC shows higher cell turnover rates in neoplastic cells and different characteristics from most solid cancers, and therefore, may show TLS more frequently than expected or reported up to present time. A previous study demon- strated that TLS associated with therapy involves higher levels of phosphorus due to cell destruction and STLS in- volves lower levels of phosphorus due to its reutilization in the synthesis of new tumor cells [8]. However, our patient showed hyperphosphatemia without a prior history of ther- apy despite STLS, which did not correspond with the pre- vious concept of phosphate levels as a discriminating tool between STLS and TLS associated with therapy.
A recent study [4] demonstrated that the striking charac- teristics of STLS in SCLC include a high incidence of hepatic metastasis, which is found in most cases of STLS in SCLC, that predispose the patient to develop STLS because of a high tumor burden, high purine levels, or decreased uric acid clearance. However, they reported a case of STLS in SCLC in a patient presenting with hyperphosphatemia and
bloodresearch.or.kr Blood Res 2019;54:229-240.
Letters to the Editor 233
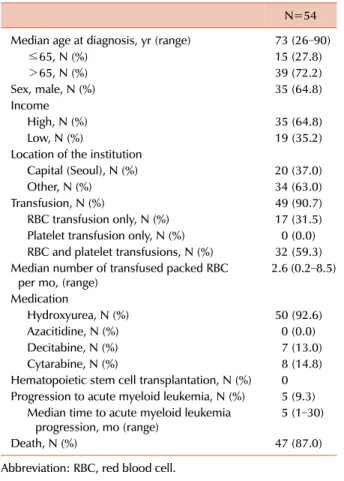
Table 1. Characteristics of atypical chronic myeloid leukemia patients.
N=54 Median age at diagnosis, yr (range) 73 (26–90)
≤65, N (%) 15 (27.8)
>65, N (%) 39 (72.2)
Sex, male, N (%) 35 (64.8)
Income
High, N (%) 35 (64.8)
Low, N (%) 19 (35.2)
Location of the institution
Capital (Seoul), N (%) 20 (37.0)
Other, N (%) 34 (63.0)
Transfusion, N (%) 49 (90.7)
RBC transfusion only, N (%) 17 (31.5) Platelet transfusion only, N (%) 0 (0.0) RBC and platelet transfusions, N (%) 32 (59.3) Median number of transfused packed RBC
per mo, (range) 2.6 (0.2–8.5)
Medication
Hydroxyurea, N (%) 50 (92.6)
Azacitidine, N (%) 0 (0.0)
Decitabine, N (%) 7 (13.0)
Cytarabine, N (%) 8 (14.8)
Hematopoietic stem cell transplantation, N (%) 0 Progression to acute myeloid leukemia, N (%) 5 (9.3) Median time to acute myeloid leukemia
progression, mo (range) 5 (1–30)
Death, N (%) 47 (87.0)
Abbreviation: RBC, red blood cell.
hyperuricemia, but without hepatic metastasis [4]; our pa- tient also showed identical results. Therefore, it cannot be precisely stated that the typical STLS in SCLC shows hepatic metastasis at diagnosis, and further studies are required to confirm the previous concept.
In conclusion, we report here a case of STLS associated with BM metastatic SCLC without hepatic metastasis at diagnosis, and to our best knowledge, this is the first case report of STLS associated with BM metastatic SCLC in Korea.
Sang Hyuk Park1, Ji-Hun Lim1, Joseph Jeong1, Seon-Ho Lee1, Hee Jeong Cha2, Yunsuk Choi3, Jae-Cheol Jo3 Departments of 1Laboratory Medicine, 2Pathology,
3Hematology and Cellular Therapy, University of Ulsan College of Medicine, Ulsan University Hospital, Ulsan, Korea
Correspondence to: Jae-Cheol Jo Departments of Hematology and Cellular Therapy, University of Ulsan College of Medicine, Ulsan University Hospital, Bangujin-sunhwandoro 877, Dong-gu, Ulsan 44033, Korea
E-mail: [email protected]
Received on Jan. 29, 2019; Revised on Feb. 19, 2019; Accepted on Mar. 8, 2019 https://doi.org/10.5045/br.2019.54.3.231
AuthorsÊ Disclosures of Potential Conflicts of Interest No potential conflicts of interest relevant to this article were reported.
REFERENCES
1. Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol 2004;127:3-11.
2. McBride A, Westervelt P. Recognizing and managing the ex- panded risk of tumor lysis syndrome in hematologic and solid malignancies. J Hematol Oncol 2012;5:75.
3. Dean RK, Subedi R, Lee M. Spontaneous tumor lysis syndrome in small cell lung cancer. Proc (Bayl Univ Med Cent) 2017;31:79-80.
4. Kanchustambham V, Saladi S, Patolia S, Stoeckel D. Spontaneous tumor lysis syndrome in small cell lung cancer. Cureus 2017;
9:e1017.
5. Padhi P, Singh S. Spontaneous tumor lysis syndrome in a patient with metastatic small cell carcinoma of the lung. J Cancer Sci Ther 2012;4:164-6.
6. Martínez-Sáez O, Mezquita L, Caravaca-Fontán F, et al.
Spontaneous tumor lysis syndrome in the setting of small cell lung cancer: report of two cases and review of the literature.
Cancer Treat Res Commun 2016;9:92-5.
7. Jallad B, Hamdi T, Latta S, Alhosaini MN, Kheir F, Iroegbu N.
Tumor lysis syndrome in small cell lung cancer: a case report and review of the literature. Onkologie 2011;34:129-31.
8. Howard SC, Jones DP, Pui CH. The tumor lysis syndrome. N Engl J Med 2011;364:1844-54.
9. Kekre N, Djordjevic B, Touchie C. Spontaneous tumour lysis syndrome. CMAJ 2012;184:913-6.
Characteristics and survival of
patients with atypical chronic myeloid leukemia
TO THE EDITOR: BCR/ABL-negative or atypical chronic myeloid leukemia (CML; aCML) is a rare hematologic malig- nancy with an estimated incidence of 1–2% among all BCR/ABL-positive CML cases [1, 2]. Due to its rarity, no prospective study has been conducted to optimize a treat- ment strategy for BCR/ABL-negative CML; consequently, BCR/ABL-negative CML is managed with palliative therapy.
A population-based study on aCML outcome is rare. Thus, aCML characteristics and outcomes were analyzed using the National Health Information Database (NHID) [3, 4].
Patients diagnosed with aCML (International Classification of Diseases, Tenth Revision, C922) between 2004 and 2015 were included. Patients 1) aged <20 years, 2) who received chemotherapy before the aCML diagnosis, and 3) for whom C922 was recorded just once during the follow-up period were excluded. Data on age, sex, insurance premiums im- posed on patients proportionate to their income, location of the medical institution, transfusion history, prescription