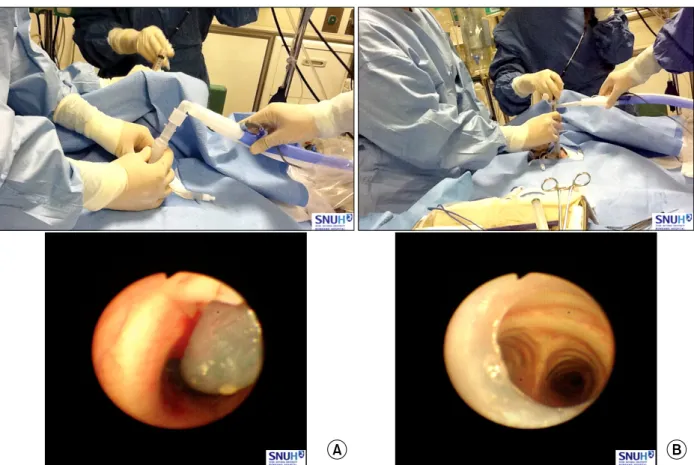
Percutaneous Dilatational Tracheostomy
14
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(12)
(13)
(14)
수치
+7
관련 문서
Prospective randomized study of open versus laparoscopy-assisted distal gastrectomy with extraperigastric lymph node dissection for early gastric cancer.. The
A prospective, randomized, double- blind, placebo-controlled multicenter trial comparing early (7 day) corticosteroid cessation versus long-term, low- dose corticosteroid
Early versus delayed treatment with ticagrelor on residual thrombus after percutaneous cor- onary intervention in patients presenting with non-ST-elevation acute
Open re- duction internal fixation versus percutaneous pinning with external fixation of distal radius fractures: a prospective, randomized clinical trial.. 대부분의
