100
서 론
갑상선 유두암은 가장 흔한 갑상선 악성 종양으로 갑상 선 분화암의 50∼90%를 차지하고, 여포암과는 달리 림프절 전이가 흔하게 발생한다.(1) 하지만 예후가 좋으며 림프절 전이가 생존율에 영향을 미치지 않는다고 알려져 있다.(2) 미국 이비인후과 및 두경부 외과 위원회(Committee for Head and Neck Surgery and Oncology of the American Academy of Otolaryngology-Head and Neck Surgery)에 따르면 경부 곽청술 을 근치적 경부 곽청술(radical neck dissection), 변형 근치적 경 부 곽청술(modified radical neck dissection), 선택적 경부 곽청술 (selective neck dissection) 및 확대 근치적 경부 곽청술(extended radical neck dissection)로 구분하였다.(3) 변형 근치적 경부 곽청 술은 척추부신경, 흉쇄유돌근 및 내경정맥 중 하나 이상을 보 존하는 수술이고, 선택적 경부 곽청술은 하나 이상의 경부 림 프군을 보존하는 수술이다. 확대 근치적 경부 곽청술은 근치적 경부 곽청술에서 하나 이상의 림프군이나 구조물을 추가적으 로 절제하는 수술이다.
경부 림프군에 대한 기술은 Memorial Sloan-Kettering병원 에서 처음 사용되었으며, 제1림프군은 이하(submental) 및 악하군(submandibular group)을 의미하며, 제2, 3, 4림프군은 상, 중, 하 경부군(jugular group)을, 제5림프군은 후삼각군 (posterior triangular group)을 의미한다. 제6림프군은 이후 추 가되었으며 전경부군(anterior compartment group)을 의미한 다.(3)
다른 두경부 종양과는 달리 갑상선 암의 림프절 전이 경 로는 갑상선과 인접한 후두 주위 림프절(paratracheal node) 을 통하여 경부 림프절(jugular node)로 전이된다. 제1림프군 은 갑상선 암에서 흔한 전이 경로가 아니며, 경부 림프절이 만져져서 시행한 곽청술의 10% 이하에서 제1림프군의 전
전이성 갑상선 유두암에서 시행한 변형 근치적 경부 곽청술과 제1림프군 보존 선택적 경부 곽청술의 비교
서울대학교 의과대학 외과학교실 장 명 철․오 승 근
Comparative Results of Modified Radical Neck Dissection and Level I Preserving Selective Neck Dissection for Metastatic Papillary Car- cinoma of the Thyroid
Myung Chul Chang, M.D. and Seung Keun Oh, M.D.
Purpose: The level I lymph node group is not a usual drainage site for papillary carcinoma of the thyroid. Dissec- tion of the level I lymph nodes may result in injury to the marginal mandibular branch of the facial nerves and the submandibular gland. The aim of this study was to clarify the possibility of a conservative neck dissection without per- forming a level I dissection.
Methods: From January 1985 to December 1989 a total of 244 patients underwent an operation for papillary carcinoma of the thyroid at Seoul National University Hospital. Eighty- two out of 244 patients who had palpable lateral cervical nodes were treated by a modified radical neck dissection.
Between January 1985 and December 1986, a level I dissection was performed. However, in the latter three years, selective neck dissection that preserved the level I lymph nodes was carried out. Thirty-three patients who underwent a classical modified radical neck dissection were compared with 49 patients who underwent a selective neck dissection without a level I dissection.
Results: There were no differences in gender and the extent of disease between the groups. One case of injury to the marginal mandibular branch of the facial nerve occurred in the level I dissected group. There were no differences in the recurrence rate and survival rate.
Conclusion: We concluded that a level I lymph node dissection is not necessary in a modified radical neck dissec- tion for treating metastatic papillary carcinoma of the thyroid.
(J Korean Surg Soc 2006;71:100-104)
Key Words:Papillary thyroid cancer, Level I, Neck dissection 중심 단어: 갑상선 유두암, 제1림프군, 경부 곽청술 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, Seoul National University College of Medicine, Seoul, Korea
책임저자:오승근, 서울시 종로구 연건동 28번지 ꂕ 110-744, 서울대학교병원 외과 Tel: 02-2072-2325, Fax: 02-766-3975 E-mail: [email protected]
접수일:2006년 4월 18일, 게재승인일:2006년 7월 13일
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 이가 발견된다.(4) 또한 제1림프군 주위에 안면신경의 악하
분지(submandibular branch)가 위치하여 손상 시 입꼬리내림 근(depressor anguli oris)의 약화로 입모양의 변형이 발생할 수 있다. 또한 제1림프군의 곽청을 생략하였을 경우 미용상 우수한 절개선을 이용하여 수술 시간을 단축시킬 수 있는 효과를 기대할 수 있다. 따라서 본 연구에서는 갑상선 유두 암에서 경부 림프절 전이가 존재할 경우 제1림프군의 곽청 이 생략 가능한지를 조사하였다.
방 법
1985년 1월부터 1989년 12월까지 서울대학교병원 외과에 서 갑상선 유두암으로 수술 받은 244명 중 136명에서 경부 림프절 전이가 있었고, 이 중 외측 경부(lateral cervical) 림프 절 전이가 있는 82명을 대상으로 하였다. 제1림프 곽청군은 82명 중 1985년부터 1986년까지의 33명의 환자로 제1림프 군을 포함한 고전적인 변형 근치적 경부 곽청술을 시행하 였다. 이후 1987년부터 1989년까지는 촉진 또는 초음파 검 사상 제1림프군 전이가 의심되지 않는 환자에 대하여 제1 림프군 곽청술을 생략하였으며 49명의 환자가 제1림프 보 존군에 포함되었다. 절개선은 제1림프 곽청군에서는 McFee 절개를 이용하였고, 제1림프 보존군에서는 low collar 절개 를 이용하였다(Fig. 1). 갑상선 절제술은 원발 병소의 크기 와 침윤 정도에 따라 일엽절제술, 아전절제술, 전절제술을 시행하였다.
환자는 2000년 9월까지 추적 관찰하였으며 추적 관찰 기 간은 10년에서 15년이었다. 두 군 간의 성별, 침윤 정도를 비교하였으며 절제된 림프절의 수, 전이 림프절의 수, 수술 후 부작용, 재발 및 생존 유무를 비교하였다. 두 군의 비교 는 Chi-square test를 이용하였으며 P값이 0.05 이하인 경우 에 유의한 차이가 있다고 해석하였다.
결 과
1) 림프절 전이 빈도
총 244명의 환자 중 136명(55.7%)에서 경부 림프절 전이 가 있었다. 성별에 따른 림프절 전이의 빈도를 살펴보면 남 자 환자는 48명 중 34명(70.8%)에서 림프절 전이가 있는 반 면, 여자 환자는 196명 중 102명(52.0%)에서 림프절 전이가 있어 남자 환자에서 여자 환자에 비해 유의하게 림프절 전 이 빈도가 높았다(P=0.02). 갑상선암의 침윤 정도에 따라 갑 상선 내에 국한된 암과 주위로 침윤된 암으로 나누었을 경 우 갑상선 내에 국한된 암의 경우 115명 중 44명(38.3%)에 서 림프절 전이가 있는 반면, 주위로 침윤된 암의 경우 129 명 중 92명(71.3%)에서 전이가 있어 주위로 침윤된 경우에 림프절 전이의 빈도가 높았다(P<0.001).
외측 경부 림프절 전이는 82명(33.6%)이었다. 남자 환자 는 27명(56.3%), 여자 환자는 55명(28.1%)으로 외측 경부 림 프절 전이도 남자 환자에서 유의하게 높았다(P<0.001). 갑 상선 내에 국한된 암 중 24명(20.9%), 주위로 침윤된 암 중 58명(45.0%)에서 외측 경부 림프절 전이가 있어 마찬가지 로 주위로 침윤된 경우에 외측 경부 림프절 전이의 빈도가 높았다(P<0.001).
2) 제1림프 곽청군과 보존군의 비교
제1림프 곽청군과 보존군에서 남녀의 비율은 곽청군에 서 남성은 12예, 여성은 21예로 남녀비는 1:1.8이었고, 보 존군에서 남성은 15예, 여성은 34예로 남녀비는 1:2.3으로 두 군 간에 차이가 없었다(P=0.59). 주위 조직으로 침윤이 진행된 예는 곽청군이 22명(66.7%)이었고, 보존군이 36명 (73.5%)으로 두 군 간에 차이가 없었다(P=0.51).
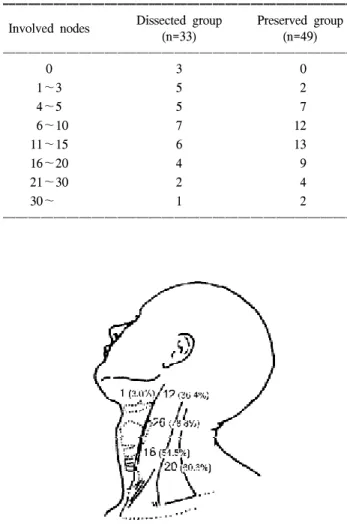
수술 후 병리조직검사에서 확인된 전이 림프절 개수는 곽청군이 평균 10개로 보존군의 평균 13개와 통계적으로 유의한 차이가 없었다(P=0.09)(Table 1). 각 림프군에서 림프 절 전이 빈도를 살펴보면 양 군 모두에서 제3림프군이 가장
Fig. 1. Skin incisions used in this study. (A) McFee incision, (B) low collar incision with cervical extension.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
많았다. 곽청군에서는 제3림프군이 78.8%, 제5림프군 60.6%, 제4림프군 54.5%, 제2림프군 36.4% 순서였고, 제1림프군은 1예(3%)에서만 전이가 발견되었다(Fig. 2). 보존군에서는 제 3림프군 75.5%, 제4림프군 59.2%, 제2림프군 51.0%, 제5림 프군 42.9%의 순서였고, 제1림프군에는 전이가 없었다(Fig.
3).
3) 장기 보존
내경정맥, 척추부신경 및 흉쇄유돌근에 육안적인 림프절 전이가 없을 경우 이러한 장기를 보존하였다. 세 가지 장기 모두 보존된 경우가 곽청군에서 16명(48.5%), 보존군에서 26명(53.1%)이었고, 내경정맥을 절제한 예는 곽청군에서 10 명(30.3%), 보존군에서 21명(42.9%)이었다. 척추부신경을 절제한 예는 곽청군에서 10명(30.3%), 보존군에서 4명(8.2%) 이었다. 흉쇄유돌근을 절제한 예는 양 군 모두 없었다(Table 2).
4) 술 후 합병증
수술 후 부갑상선이나 회귀 후두신경 손상과 연관된 합 병증은 없었다. 척추부신경을 절제한 14명 모두와 척추부 신경이 보존된 4명에서 어깨 부위의 통증을 호소하였다. 이 는 제1림프 곽청군의 42.2%와 보존군의 8.2%였다. 귓불(ear lobe) 주위의 저린 감각을 호소한 예는 제1림프 곽청군의 63.6%와 보존군의 28.6%였다. 어깨 부위의 통증과 귓불 주 위의 저린 감각은 제1림프 곽청군에서 유의하게 많았다(P<
0.01). 제1림프 곽청군 중 1예에서 안면신경의 악하분지 손 상이 있었으며, 제1림프 보존군 중 1예에서 흉관 손상이 있 었다(Table 3).
5) 술 후 결과
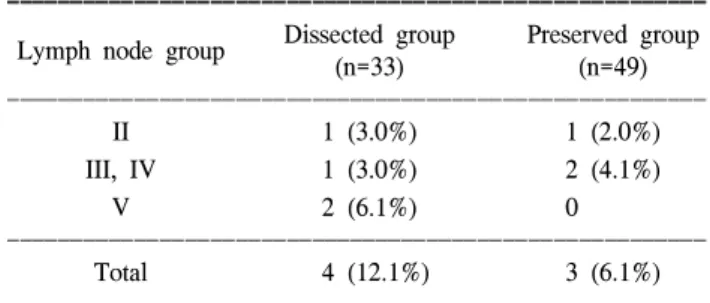
최소 10년에서 15년간의 추적 기간 중, 7명에서 임상적으 로 림프절 재발이 관찰되었다(Table 4). 이 중 4명(12.1%)은 제1림프 곽청군이었고 3명(6.1%)은 보존군으로 제1림프 보 존군에서 림프절 재발이 적었으나 통계적인 의미는 없었다 Table 1. Number of metastatic nodes in the level I dissected and
preserved groups.
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Dissected group Preserved group Involved nodes
(n=33) (n=49)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
0 3 0
1∼3 5 2
4∼5 5 7
6∼10 7 12
11∼15 6 13
16∼20 4 9
21∼30 2 4
30∼ 1 2
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Fig. 2. Location of metastatic nodes in the level I dissected group.
Fig. 3. Location of metastatic nodes in the level I preserved group.
*Level I dissection was not done.
Table 2. Structures preserved in the level I dissected and preserved groups
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Dissected group Preserved group Preserved structures
(n=33) (n=49)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ SCM SAN IJV 16 (48.5%) 26 (53.1%)
SCM SAN 7 (21.2%) 19 (38.8%)
SCM IJV 7 (21.2%) 2 (4.1%)
SCM 3 (9.1%) 2 (4.1%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ SCM = sternocleidomastoid muscle; SAN = spinal accessory nerve; IJV = internal jugular vein.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
(P=0.43). 재발된 7명은 림프절의 국소 절제를 시행하였다.
재발한 예를 포함한 82예 모두에서 사망은 없었다.
고 찰
본 연구에서 경부 곽청술은 림프절 전이가 의심되는 경 우에서만 시행하였고 예방적 곽청술은 시행하지 않았다.
이전 보고에 의하면 예방적 경부 곽청술 시의 림프절 전이 빈도는 90%인 반면,(5) 임상적으로 관찰되는 재발률은 10%
이하이다.(6) 이러한 차이는 미세한 현미경적 전이와 임상 적으로 만져지는 림프절 전이에 차이가 있기 때문인데 이 는 대부분의 미세 전이가 진행하지 않기 때문이다. 이러한 유두상 갑상선암의 느린 성장은 갑상선암의 치료에 있어 좀 더 보존적인 경향을 나타내어 림프절이 임상적으로 만 져지지 않는다면 예방적인 경부 곽청은 권장되지 않는다.
이러한 보존적 치료 방침의 이유로는 첫째, 림프절 전이가 생존율에 영향을 주지 않는다고 알려져 있으며, 둘째, 확대 수술이 생존율의 향상에 도움이 되지 않고, 셋째, 이러한 확 대 수술로 인하여 수술 후 부작용의 가능성이 증가하기 때 문이다.
제1림프군은 갑상선암에서 주된 림프절 전이 경로가 아 니며 전이 빈도는 0.6에서 11%로 낮다. Frazell과 Foote(4)는 치료적 경부 곽청술의 10%에서 제1림프군 전이가 발견되 었다고 하였으며, 예방적 경부 곽청술에서는 1.5%에서만이 발견되었다고 하였다. Marchetta 등(7)은 임상적으로 만져지 는 경부 림프절 곽청술의 11%에서 전이가 발견되었다고 하 였다. Attie(8)는 158예의 경부 곽청술에서 1예에서만 제1림 프군 전이를 발견하였으며, Lin 등(9)은 167예의 경부 곽청 술 중 3예에서 전이를 발견하였다고 하였다. 본 연구에서는 1예에서만이 제1림프군 전이가 있었으며, 이와 같이 제1림 프군 전이가 드물기 때문에 연구의 후반기에는 제1림프군 곽청술을 생략하게 되었다.
경부 곽청술의 부작용으로 1예에서 안면신경의 악하분 지 손상이 있었다. Lahey(10)는 악하분지 손상이 우려될 경 우 수술 전 환자에게 이에 대한 설명이 필요하다고 하였으 며, 수술 중 신경 자극기를 이용하여 신경의 위치를 파악하
면 신경 손상을 막는 데 도움이 된다고 하였다. 또한 안면신 경의 악하분지는 안면동맥과 정맥을 가로질러 주행하므로 이러한 혈관을 이용하여 악하분지를 둘러싸는 고리를 만들 경우 물리적 손상이나 전기 소작기로 인한 열손상을 방지 할 수 있다.(11)
Attie(8)는 두 개의 절개선을 이용하다가 하나의 절개선으 로 바꾸었는데, 하나의 횡절개로도 두힘살근(digastic muscle) 까지의 경부 림프절 곽청술이 가능하였다. 절개선을 여러 개 이용할 경우 혈액 순환의 문제로 인하여 상처의 괴사 등 부작용이 발생할 수 있다. 따라서 하나의 절개선은 이러 한 부작용을 방지할 수 있고 대부분의 환자에서 기능성 및 미용상 만족할 만한 결과를 가져왔다. 본 연구의 전반기에 는 전형적인 McFee 절개를 이용하였는데 미용상 및 기능상 의 이유로 인하여 후반기에는 경부 절개로 바꾸어 시행하 였다.
처음에는 제1림프군을 포함한 변형 근치적 경부 곽청술 을 시행하였다. 하지만 1예의 악하분지 손상을 경험하고 나 서 임상 진찰이나 초음파로 제1림프군의 전이가 의심되지 않는 경우에는 제1림프군 곽청술을 시행하지 않았다. 위에 서 언급하였듯이 이러한 치료 방침의 전환은 제1림프군 전 이 빈도가 적고 제1림프군 곽청술로 인하여 좀 더 많은 합 병증이 발생할 수 있기 때문이다. 또한 제1림프군을 보존함 으로 인하여 수술 시간을 단축할 수 있고 미용상에 도움을 주기 때문이다. 제1림프 곽청군과 보존군을 비교하였을 때 재발이나 사망에서 차이가 없었다. 이상에서 제1림프군 전 이가 의심되지 않는 경우에 제1림프군 곽청술은 생략이 가 능하며, 만약에 임상 진찰에서 제1림프군 전이가 의심되는 경우는 초음파 검사가 도움이 될 것이라 생각되었다.
결 론
갑상선 유두암 중 경부 림프절 전이 환자를 대상으로 시 행한 변형 근치적 경부 곽청술에서 제1림프 곽청군과 제1 림프 보존군 사이에 재발 및 사망률의 차이가 없었다. 이는 갑상선 유두암의 림프절 전이 경로가 다른 두경부 종양과 Table 3. Postoperative complications in the level I dissected and
preserved groups
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Dissected group Preserved group Complications
(n=33) (n=49)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Ear lobe numbness 21 (63.6%) 14 (28.6%) Aching shoulder pain 14 (42.4%) 4 (8.2%) Mandibular branch injury 1 (3.0%) 0 Thoracic duct injury 0 1 (2.0%) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Table 4. Regional lymph node recurrences in the level I dissected and preserved groups
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Dissected group Preserved group Lymph node group
(n=33) (n=49)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
II 1 (3.0%) 1 (2.0%)
III, IV 1 (3.0%) 2 (4.1%)
V 2 (6.1%) 0
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total 4 (12.1%) 3 (6.1%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 다르며, 유두상 갑상선암의 느린 성장으로 제1림프군 전이
가 드물기 때문으로 생각된다. 또한 제1림프군 절제를 생략 함으로써 수술시간을 단축하고 부작용이 적으며 미용상 우 수한 절개선으로 수술이 가능할 것이다. 따라서 전이성 갑 상선 유두암의 변형 근치적 경부 곽청술에서 제1림프군의 전이가 의심되지 않는 경우 제1림프군 절제는 생략 가능하 리라 생각된다.
REFERENCES
1) Schlumberger MJ, Filetti S, Hay ID. Nontoxic goiter and thyroid neoplasia. In: Larsen PR, editor. Williams Textbook of Endocrinology. 10th ed. Philadelphia: W.B. Saunders; 2002.
p.469-73.
2) Shaha AR. Management of the neck in thyroid cancer. Oto- laryngol Clin North Am 1998;31:823-31.
3) Robbins KT. Classification of neck dissection: current concepts and future considerations. Otolaryngol Clin North Am 1998; 31:639-55.
4) Frazell EL, Foote FW. Papillary thyroid carcinoma: pathol
ogical findings in cases with and without clinical evidence of cervical node involvement. Cancer 1955;8:1164-6.
5) Attie JN, Khafif RA, Steckler RM. Elective neck dissection in papillary carcinoma of the thyroid. Am J Surg 1971;122:
464-71.
6) Mazzaferri EL, Young RL. Papillary thyroid carcinoma: a 10 year follow-up report of the impact of therapy in 576 patients.
Am J Med 1981;70:511-8.
7) Marchetta FC, Sako K, Matuura H. Modified neck dissection for carcinoma of the thyroid gland. Am J Surg 1970;120:452-5.
8) Attie JN. Modified neck dissection in treatment of thyroid cancer: a safe procedure. Eur J Cancer Clin Oncol 1988;24:
315-24.
9) Lin JD, Liou MJ, Chao TC, Weng HF, Ho YS. Prognostic variables of papillary and follicular thyroid carcinoma patients with lymph node metastases and without distant metastases.
Endocr Relat Cancer 1999;6:109-15.
10) Lahey F. Radical dissection of the neck. Surg Clin North Am 1949;29:631.
11) Palkar VM. Protection of marginal mandibular nerve during neck dissection. J Surg Oncol 1997;66:54.