795
Correlation between the Carotid Intima-Media Thickness and the Plaque Burden of the Left Main Coronary Artery Using Ultrasonography
Dae Woo Hyun, MD1, Kee Sik Kim, MD2 and Seung Ho Hur, MD2
1Division of Cardiology, Cardiovascular Center, College of Medicine Konyang University, Daejeon,
2Department of Cardiology, Keimyung University Dongsan Medical Center, Daegu, Korea
ABSTRACT
Background and Objectives:It has been reported that the common carotid artery (CCA) intima-media thickness (IMT) correlates to angiographically determined coronary artery stenosis. The aim of this study was to evaluate the correlation between the carotid IMT and left main (LM) plaque using ultrasonography. Subjects and Methods:In fifty patients (mean age 59.6±9.9, males 35 (70%)) with coronary artery disease (CAD), the risk factors of atherosclerosis were evaluated and coronary angiographs obtained. The carotid IMT was measured in the far wall of both CCAs, with a 10 MHz linear probe, and the value of the IMT was automatically calculated using programmed software (M’ATH, METRIS Co., Argenteuil, France). The LM plaque was measured by intravascular ultrasound. The maximal thickness, ratio of the maximal thickness, cross-sectional area (CSA) and burden of the plaque were measured at 2 mm intervals, and the average values calculated. Results:In the right common carotid artery, the maximal IMT significantly correlated with the mean plaque CSA and plaque burden of the LM (r=0.375. p=0.007, r=0.408. p=0.003, respectively). The mean IMT significantly correlated with the plaque burden of the LM, but not with the mean plaque CSA of the LM (r=0.357. p=0.011, r=0.264. p=0.063, respectively). In the left common carotid artery, the maximal IMT was not significantly correlated with the mean plaque CSA and plaque burden of the LM (p=0.251, p=0.218, respectively). The mean IMT was not correlated with the mean plaque CSA and plaque burden of the LM (p=0.249, p=0.078, respectively). Conclusion:There was a significant correlation between the right CCA IMT and plaque burden of the LM in patients with CAD.
(Korean Circulation J 2005;35:795-800)
KEY WORDS:Ultrasound;Coronary disease;Carotid arteries.
Introduction
The ultrasonographic assessment of peripheral arte- ries has evolved as a promising technique for non-in- vasive evaluation of atherosclerosis.1)2) Assessment of the carotid artery intima-media thickness(IMT), using B- mode ultrasound, is a useful clinical and research tool for the measurement of atherosclerosis.3) An increased IMT is considered as a sign of early atherosclerosis of the carotid artery, and is associated with future car- diovascular events, asymptomatic myocardial ischemia, coronary risk factors and a change in the coronary risk factors after therapeutic intervention. The effect of the
IMT of the carotid artery has been used as the primary variable in the evaluation of the progression/regression of atherosclerosis during lipid-lowering or antihyper- tensive treatment.4)5) The atherosclerotic process can be studied at an earlier phase through measurement of the carotid IMT. Determination of the carotid IMT allows for a direct, non-invasive, repeatable measure- ment. It has been reported that the common carotid IMT is correlated to the angiographically determined coronary artery stenosis in coronary angiography,6-9) this correlation is only weak.10) In contrast to coronary angiography, which investigates the vascular contour and lumen, intravascular ultrasound(IVUS) imaging depicts the structural morphology of the arterial wall itself. Despite being angiographically silent, left main (LM) disease, as detected by IVUS, is an independent predictor of future cardiac events and may serve as a marker for such events.11) The aim of this study was to evaluate the correlation between the carotid IMT and the plaque burden of the left main coronary artery(LM),
Received:April 25, 2005 Revision Received:June 23, 2005 Accepted:July 28, 2005
Correspondence:Kee Sik Kim, MD,Department of Cardiology, Keimyung University Dongsan Medical Center, #194 Dongsan-dong, Jung-gu, Daegu 700-721, Korea
Tel: 82-53-250-7379, Fax: 82-53-250-7434 E-mail: [email protected]
using B-mode ultrasound and IVUS, respectively.
Subjects and Methods Study population
Fifty consecutive patients with ischemic heart disease, undergoing percutaneous coronary intervention on the left anterior descending or left circumflex artery, were enrolled. All had angiographically normal or mild LM disease by visual assessment(<20% diameter ste- nosis). The diagnosis of stable angina was defined as a clinically constant pattern of severity for more than two months. Unstable angina was diagnosed if the patient’s chest pain, which was accompanied by electrocardio- graphic ST-T changes, was either new or worse in fre- quency, severity or duration, superimposed on a pre- existing pattern of anginal pain. Patients were diagnos- ed as having myocardial infarction according to the presence of chest pain lasting more than 30 minutes, accompanied by ST-T segment elevation in two or more related electrocardiographic leads, pathologic Q waves, or elevation of serum levels of creatine kinase- MB fraction(CK-MB)(more than twice the upper normal limit) or cardiac troponin-I. Hypertension was defined as a blood pressure ≥140/90 mmHg or the use of anti- hypertensive medications. Diabetes was defined as being present when previously diagnosed by a physician. Smo- king was estimated from the patient’s history. Hyper- cholesterolemia was defined as a total-cholesterol level of ≥200 mg/dL. Obesity was defined as a body mass index(BMI)(weight in kilograms divided by the square of the height in meters) of ≥25.
Measurement of the carotid IMT
B-mode ultrasound measurements were performed with a 10-MHz linear- array transducer, connected to a
Vivid 7 echocardiograph(General Electronics Corp., Horten, Norway). The patients were examined in the supine position. The operator directed the sound beam perpendicularly to the arterial surface of the far wall of the common carotid artery(CCA) to obtain two pa- rallel echogenic lines, corresponding to the blood-in- tima and media-adventitia interfaces. The right and left CCA IMT were measured at least 10 mm proximal to the bifurcation. The values of the maximal and mean IMT were automatically calculated by the programmed software(M’ATH, METRIS Co., Argenteuil, France) (Fig. 1). The presence of a plaque was evaluated in the carotid artery. The plaque was defined as a distinct area, with an IMT exceeding twice that of the neighbo- ring sites, so an IMT > 1.3 mm was consequently not included in the calculation of the carotid IMT.
Measurement of the LM plaque and coronary an- giography
Coronary angiography was performed using the stan- dard Judkins technique, and significant coronary artery stenosis was diagnosed when the coronary angiogram showed a ≥50% reduction in the lumen diameter. The LM plaque was measured using IVUS(CLEARVIEW.
Boston Scientific Corp., San Jose, California, USA), with a 30 MHz probe, at 2 mm intervals. In each cross section, the maximal thickness, ratio of thickness, cross- sectional area(CSA) and burden of the LM plaque were measured. These variables were calculated by the following formulae: ratio of the thickness=(maximal plaque thickness/vessel diameter)×100, plaque CSA
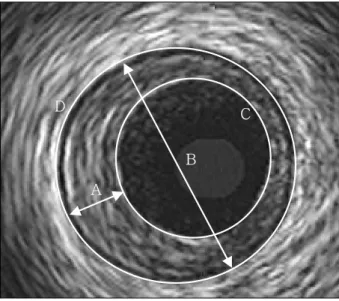
=vessel CSA-lumen CSA, plaque burden=(plaque CSA/vessel CSA)×100(Fig. 2). For each variable the
Fig. 1. Measurement of the carotid intima-media thickness (IMT). The values of the maximal (Max) and mean (Mean) intima-media thickness is automatically calculated using programmed software (M’ATH, ME- TRIS Co., Argenteuil, France). Q.I.: qualitative index, Std D: stan- dard deviation.
Fig. 2. Measurement of the plaque of the left main coronary artery.
The plaque of the left main coronary artery was measured at 2 mm intervals, and the average value calculated. Maximal thickness (A), Ratio of thickness (%)=Maximal plaque thickness (A)/Vesseldiame- ter (B) ×100, Plaque CSA=Vessel CSA (D)-Lumen CSA (C), Burden (%)=Plaque CSA/Vessel CSA (D) ×100. CSA: cross sectional area.
A
D C
B
average value was calculated.
Statistical analysis
All results were expressed as the mean±standard error of the mean. SPSS 11.0 was used for all statistical calculations. Statistical comparisons were performed using Student’s t-tests. Correlations between the varia- bles of the carotid IMT and plaque of the LM were evaluated using the Pearson correlation coefficient. A probability value of <0.05 was taken as statistically sig- nificant. Multiple linear regression analysis was used to test for an association between the plaque burden of the LM and male, hypertension, diabetes, smoking, hy- percholesterolemia, obesity and the mean right CCA IMT.
Results Baseline characteristics
The mean age of the patients in this study was 59.6
±9.9 years; 70% were male. The diagnoses of the pa- tients were 16(32%) with stable angina, 10(20%) with unstable angina and 24(48%) with myocardial infarc-
tion. Hypertension was present in 20(40%), diabetes mellitus in 9(18%), smoking in 27(54%), hypercho- lesterolemia in 15(30%) and obesity in 16(32%) of the patients.
Twenty-seven patients(54%) had a one-vessel disease, 17(34%) a two-vessel disease and 6(12%) a three- vessel disease(Table 1).
Effect of the risk factors for carotid IMT and LM plaque
With regard to a difference between the genders, the plaque CSA and burden of the LM were 10.9±4.2 mm2, 40.9±12.0% in males and 8.2±1.7 mm2, 32.9
±6.9% in females, respectively. The plaque CSA and burden were significantly larger in the males compared to those in the females(p=0.023, p=0.019). In the hy- pertensive and normotensive patients, the right maximal and mean carotid IMTs were 1.04±0.17 and 0.82±
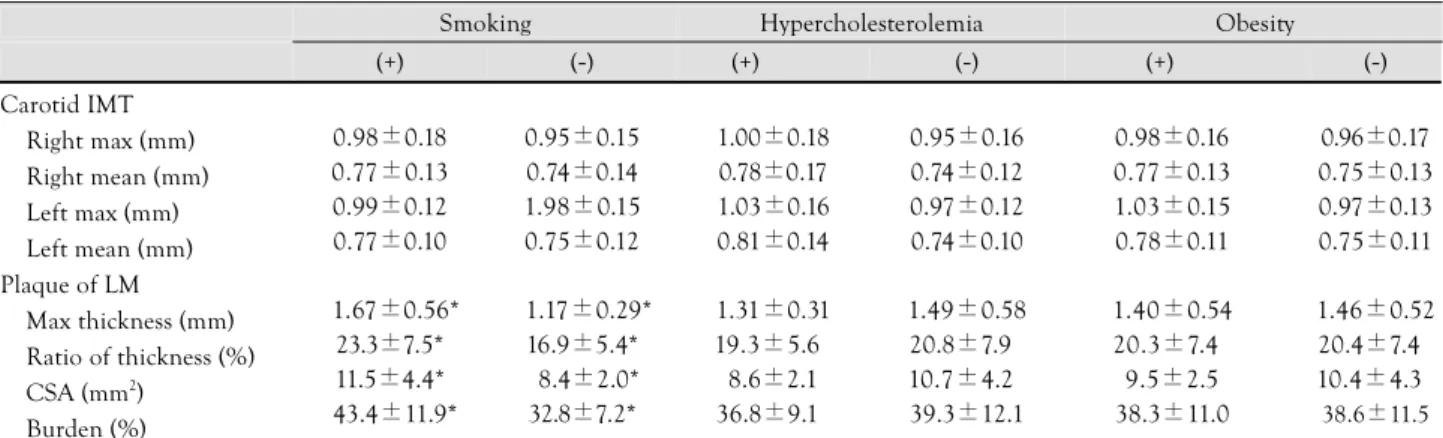
0.14 mm, and 0.91±0.14 and 0.71±0.11 mm, respec- tively. The right maximal and mean carotid IMT were larger in the hypertensive than normotensive patients (p=0.005, p=0.006). For diabetes mellitus, there was no significant difference between the patients with and those without in the carotid IMT and plaque of the LM(Table. 2A). For smoking, the maximal thickness, ratio of the thickness, CSA and burden of the LM pla- que were 1.67±0.56 mm, 23.3±7.5%, 11.5±4.4 mm2 and 43.4±11.9%, respectively, in the smokers and 1.17±0.29 mm, 16.9±5.4%, 8.4±2.0 mm2 and 32.8
±7.2%, respectively, in the non-smokers. The maxi- mal thickness, ratio of the thickness, CSA and burden of the plaque were larger in the smokers than in the nonsmokers(p=0.000, p=0.002, p=0.003 and p=
0.000, respectively)(Table. 2B). In a multiple linear regression analysis, the plaque burden of the LM was significantly associated with smoking and the right mean CCA IMT(p=0.042, p=0.029, respectively)(Table 3).
Plaque of the LM related to the presence or absence of carotid plaque
A carotid plaque was present in 14(28%) patients;
Table 2A. The effects of risk factors in the carotid intima-media thickness and plaque of the left main coronary artery
Sex Hypertension Diabetes
Male Female (+) (-) (+) (-)
Carotid IMT Right max (mm) Right mean (mm) Left max (mm) Left mean (mm) Plaque of LM
Max thickness (mm) Ratio of thickness (%) CSA (mm2)
Burden (%)
0.96±0.18 0.75±0.13 0.97±0.12 0.76±0.11
1.53±0.56 21.6±7.40 10.9±4.2*
*40.9±12.0*
0.98±0.14 0.76±0.14 1.02±0.17 0.76±0.13
01.21±0.30 17.5±6.30 08.2±1.7*
32.9±6.9*
1.04±0.17*
0.82±0.14*
1.00±0.14*
0.78±0.13*
1.54±0.50*
20.9±7.10*
10.5±3.8**
38.6±11.3*
0.91±0.14*
0.71±0.11*
0.98±0.13*
0.75±0.10*
1.37±0.53*
20.0±7.5**
9.8±3.8*
38.5±11.5*
1.07±0.17 0.84±0.15 1.06±0.10 0.82±0.09
1.58±0.48 22.0±5.8*
10.7±3.4*
40.7±7.0*
0.94±0.16 0.74±0.12 0.97±0.14 0.75±0.12
1.41±0.53 20.0±7.60 9.9±3.9 38.1±12.0 IMT: intima-media thickness, LM: left main coronary artery, Max: maximal, CSA: cross-sectional area. *: p<0.05
Table 1. Baseline characteristics Age (years)
Male BMI (kg/m2) Risk factors
Hypertension Diabetes mellitus Smoking
Hypercholesterolemia Obesity
Diagnosis Stable angina Unstable angina
Acute myocardial infarction Number of stenotic coronary artery
1 2 3
59.6±9.9 35 (70%) 23.9±2.3
20 (40%) 09 (18%) 27 (54%) 15 (30%) 16 (32%)
16 (32%) 10 (20%) 24 (48%)
27 (54%) 17 (34%) 06 (12%) BMI: body mass index
a right carotid plaque in 8(16%), a left plaque in 11 (22%), and both left and right plaques in 5(10%).
For the thickness and ratio of the thickness of the LM plaque, there was no significant difference between the patients with carotid plaque and those without. The plaque CSA and burden were 12.2±4.3 mm2 and 43.5±10.7%, respectively in the patient with carotid plaque and 9.3±3.3 mm2 and 36.6±11.0%, respecti- vely, in those patient without. The plaque CSA and burden of the LM were larger in patients with than without carotid plaques(p=0.014, p=0.048)(Fig. 3).
Correlation between the carotid IMT and plaque of the LM
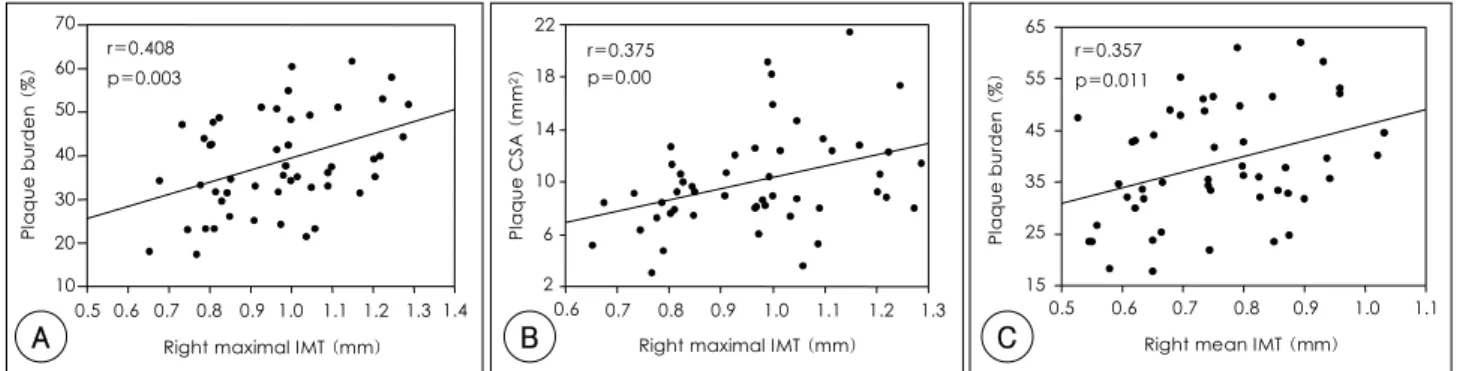
In the right common carotid artery(CCA), the ma- ximal IMT was significantly correlated to the plaque CSA and burden of the LM(r=0.375. p=0.007, r=
0.408. p=0.003, respectively)(Fig. 4A, B). The mean IMT was significantly correlated to the plaque burden (Fig. 4C), but not with the plaque CSA of the LM (r=0.357. p=0.011, r=0.264. p=0.063, respectively).
In the left CCA, the maximal IMT was not signifi- cantly correlated to the plaque CSA and burden of the LM(p=0.251, p=0.218, respectively). The mean IMT was not correlated with the plaque CSA and burden of the LM(p=0.249, p=0.078, respectively).
Discussion
Carotid artery disease and coronary artery disease (CAD) are primary manifestations of generalized athe- rosclerosis. An association between carotid atheroscle- rosis and coronary atherosclerosis has been demons- trated in several epidemiologic and clinical studies.1)3)12-14) An increased IMT and plaque development in the extracranial carotid arteries were correlated with the prevalence of coronary artery disease.6-9) Our study in- vestigated the correlations between coronary atheroscle- rosis, as and carotid atherosclerosis, as detected by IVUS and ultrasonography, respectively.
The IMT was defined as the maximum measurement determined at the far wall between the leading edges of the lumen-intima and the media-adventitia inter- faces. There are many different methods for measuring the carotid IMT. In previous studies, measurement of the IMT was subjective as the operator and the points of measurement were poor(less than 10 points).5)6)15) In our study, the value of the IMT was automatically calculated using programmed software(M’ATH, ME- TRIS Co., Argenteuil, France)(Fig. 1); thus, the mea- surement of the IMT was objective and the points of
Table 2B. The effects of risk factors in the carotid intima-media thickness and plaque of the left main coronary artery
Smoking Hypercholesterolemia Obesity
(+) (-) (+) (-) (+) (-)
Carotid IMT Right max (mm) Right mean (mm) Left max (mm) Left mean (mm) Plaque of LM
Max thickness (mm) Ratio of thickness (%) CSA (mm2)
Burden (%)
0.98±0.18 0.77±0.13 0.99±0.12 0.77±0.10
01.67±0.56*
23.3±7.5*
11.5±4.4*
*43.4±11.9*
0.95±0.15 0.74±0.14 1.98±0.15 0.75±0.12
01.17±0.29*
16.9±5.4*
08.4±2.0*
32.8±7.2*
1.00±0.18 0.78±0.17 1.03±0.16 0.81±0.14
1.31±0.31 19.3±5.60 8.6±2.1 36.8±9.10
0.95±0.16 0.74±0.12 0.97±0.12 0.74±0.10
1.49±0.58 20.8±7.90 10.7±4.20 39.3±12.1
0.98±0.16 0.77±0.13 1.03±0.15 0.78±0.11
1.40±0.54 20.3±7.40 9.5±2.5 38.3±11.0
0.96±0.17 0.75±0.13 0.97±0.13 0.75±0.11
1.46±0.52 20.4±7.40 10.4±4.30
38.6±11.5 IMT: intima-media thickness, LM: left main coronary artery, Max: maximal, CSA: cross sectional area. *: p<0.05
Table 3. Stepwise multiple linear regression analysis for the plaque burden of the left main coronary artery as a dependent variable
B SE (B) p
Male Hypertension Diabetes Smoking
Hypercholesterolemia Obesity
Mean IMT, right CCA
2.814 -0.546 0.247 8.088 -0.319 -1.036 28.535
04.038 03.298 03.923 03.849 03.276 03.062 12.625
0.490 0.869 0.950 0.042 0.923 0.737 0.029 IMT: intima-media thickness, CCA: cross-sectional area, B: regres- sion coefficient, SE (B): standard error of regression coefficient
Fig. 3. The plaque of the left main coronary artery (LM) related to the presence or absence of a carotid plaque. CCA: common carotid artery, CSA: cross sectional area, NS: not significant.
Maximal thickeness (mm)
(-) CCA plaque (+)
1.38 1.58
p=NS
(-) CCA plaque (+) p=NS
p<0.05 p<0.05
(-) CCA plaque (+) (-) CCA plaque (+) Ratio of thickeness (%)
Plaque CSA (mm2) Plaque burden (%)
9.3 12.2 36.6 43.5
19.6 22.3
measurement were larger(more than 100 points) than in previous studies.
Carotid plaques are related to the risk of cardiovas- cular death or myocardial infarction.15) Kato et al.5) reported that the prevalence of soft and hard plaques was higher in the patients with multiple coronary pla- ques than in those with single plaques. In ACS, they demonstrated that multiple coronary plaques are asso- ciated with positive carotid remodeling. Honda et al.16) reported that echolucent carotid plaques, with low in- tegrated backscatter values, predicted the coronary pla- que complexity and development of future coronary complications in patients with stable CAD. These fin- dings5)15-17) may suggest that carotid plaques may reflect vulnerable coronary lesions. Giral et al.18) reported that echographic evaluation of the carotid plaque signifi- cantly improved the diagnostic specificity of the exercise electrocardiography. There are usefulness in predicting CAD by ultrasonic evaluation of the carotid plaque.17)18) In our study, carotid plaques were found in 28% of patients. The plaque burden of the LM was larger in the patient with carotid plaques than in those without(Fig.
4). This finding suggests that the evaluation of the carotid plaque appears to provide information on the diagnosis of CAD.
An increased carotid IMT is regarded as an early sign of atherosclerosis. The IMT increases if the vas- cular walls are exposed to cardiovascular risk factors, such as age, hypercholesterolemia, hypertension and smoking.19-22) The reduction of the cardiovascular risk factors inhibits the progression of increases in the IMT.4) Because B-mode ultrasound imaging of arterial walls is a noninvasive and “patient-friendly” technique, it allows for repeated measurements over time in large groups of patients. Therefore, the method has become a powerful tool in studies of atherosclerosis.
Coronary angiography can only indirectly measure the degree of atherosclerosis by assessing the lumen size. Therefore, coronary angiography can only quan- tify the atherosclerosis at a relatively later stage of in- trusive lesion formation. Unlike angiography, which in-
vestigates the vascular contours and lumen, ultrasound imaging depicts the structural morphology of the arte- rial wall itself. Despite being angiographically silent, the LM disease detected by IVUS is an independent predictor of future cardiac events, which may serve as a marker for such events.11) The LM was selected from among the coronary arteries, because the evaluation of whole segments is possible in the left main coronary artery using IVUS.
There are many studies about the relationship bet- ween coronary atherosclerosis detected angiographi- cally and carotid atherosclerosis.6-9) Carotid IMT mea- surements can give a comprehensive picture of the da- mage caused on the arterial wall by several coronary heart disease risk factors over time23) and are an indicator of generalized atherosclerosis.3) Adams et al.10) reported that although the carotid IMT is significantly correlated with the extent and severity of coronary artery disease, the relationship is only weak. Usually, both CCAs were used to evaluate the carotid IMT.3)4)12)13)18)23)24) Some reports25)26) have described that one of the CCAs IMT was correlated with CAD, and was used to evaluate the carotid IMT. Ogata et al.27) reported that the average of the maximum CCA IMT was significantly correlated with the LM atherosclerosis evaluated by IVUS. In this study, the right carotid IMT was more correlated with the LM plaque than the left carotid IMT. It may seem that the right CCA is a shorter distance from the LM than the left CCA.
This study had some limitations; the sample size was small and the patients were a consecutive group under- going cardiac catheterization. This selection bias means that the correlations between the carotid IMT and CAD may not be applicable to the general population.
Conclusion
There was a significant correlation between the right carotid IMT and plaque burden of the LM in the pa- tient with CAD. The presence of plaques in the CCAs provides information for diagnosing CAD. These fin- dings suggest that the evaluation of the CCA by ultra- A Right maximal IMT (mm)
10 20 30 40 50 60 70
0.5 0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3 1.4 r=0.408
p=0.003
Plaque burden (%) r=0.375
p=0.00
2 6 10 14 18 22
Plaque CSA (mm2)
Right maximal IMT (mm)
0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3
r=0.357 p=0.011
15 25 35 45 55 65
0.5 0.6 0.7 0.8 0.9 1.0 1.1
Plaque burden (%)
Right mean IMT (mm)
B C
Fig. 4. A: correlation between the right carotid intima-media thickness (IMT) and the plaque burden of the left main coronary artery. B: correlation between the right maximal value of the carotid IMT and plaque cross-sectional area (CSA) of the left main coronary artery. C: correlation between the right mean value of the carotid IMT and the plaque burden of the left main coronary artery.
sound can be useful in the diagnosis of LM disease or coronary atherosclerosis.
REFERENCES
1) Chambless LE, Folsom AR, Sharrett AR, et al. Coronary heart disease risk prediction in the Atherosclerosis Risk in Commu- nities(ARIC) study. J Clin Epidemiol 2003;56:880-90.
2) Kieltyka L, Urbina EM, Tang R, Bond MG, Srinivasan SR, Berenson GS. Framinghan risk score is related to carotid artery intima-media thickness in both white and black young adults.
Atherosclerosis 2003;170:125-30.
3) Bots ML, Hofman A, de Jong PT, Grobbee DE. Common carotid intima-media thickness as an indicator of ahterosclerosis at other sites of the carotid artery. Ann Epidemiol 1996;6:147-53.
4) de Groot E, Jukema JW, Montauban van Swijndregt AD, et al.
B-mode ultrasound assessment of pravastatin treatment effect on carotid and femoral artery walls and its correlations with coro- nary arteriographic findings. J Am Coll Cardiol 1998;31:1561-7.
5) Kato M, Dote K, Habara S, Takemoto H, Goto K, Nakaoka K.
Clinical implications of carotid artery remodeling in acute coro- nary syndrome: ultrasonographic assessment of positive remo- deling. J Am Coll Cardiol 2003;42:1026-32.
6) Sonoda M, Yonekura K, Yokoyama I, Takenaka K, Nagai R, Aoyagi T. Common carotid intima-media thickness is correlated with myocardial flow reserve in patients with coronary artery disease: a useful non-invasive indicator of coronary atheros- clerosis. Int J Cardiol 2004;93:131-6.
7) Takashi W, Tsutomu F, Kentaro F. Ultrasonic correlates of com- mon carotid atherosclerosis in patients with coronary artery di- sease. Angiology 2002;53:177-83.
8) Sakaguchi M, Kitagawa K, Nagai Y, et al. Equivalence of plaque score and intima-media thickness of carotid ultrasonography for predicting severe coronary artery lesion. Ultrasound Med Biol 2003;29:367-71.
9) Mack WJ, LaBree L, Liu C, Selzer RH, Hodis HN. Correlations between measures of atherosclerosis change using carotid ultra- sonography and coronary angiography. Atherosclerosis 2000;
150:371-9.
10) Adams MR, Nakagomi A, Keech A, et al. Carotid intima-media thickness is only weakly correlated with the extent and severity of coronary artery disease. Circulation 1995;92:2127-34.
11) Ricciardi MJ, Meyers S, Choi K, Pang JL, Goodreau L, David- son CJ. Angiographically silent left main disease detected by intravascular ultrasound: a marker for future adverse cardiac events. Am Heart J 2003;146:507-12.
12) Kitamura A, Iso H, Imano H, et al. Prevalence and correlates of carotid atherosclerosis among elderly Japanese men. Atheroscle- rosis 2004;172:353-9.
13) Lekakis JP, Papamichael CM, Cimponeriu AT, et al. Atheroscle-
rotic changes of extracoronary arteries are associated with the extent of coronary atherosclerosis. Am J Cardiol 2000;85:949-52.
14) Spence JD. Ultrasound measurement of carotid plaque as a sur- rogate outcome for coronary artery disease. Am J Cardiol 2002;
89(Suppl):10B-16B.
15) Held C, Hjemdahl P, Eriksson SV, Bjorkander I, Forslund L, Rehnqvist N. Prognostic implications of intima-media thickness and plaques in the carotid and femoral arteries in patients with stable angina pectoris. Eur Heart J 2001;22:62-72.
16) Honda O, Sugiyama S, Kugiyama K, et al. Echolucent carotid plaques predict future coronary events in patients with coronary artery disease. J Am Coll Cardiol 2004;43:1177-84.
17) Liapis CD, Kakisis JD, Dimitroulis DA, Kostakis AG. The im- pact of the carotid plaque type on restenosis and future cardio- vascular events: a 12-year prospective study. Eur J Vasc Endo- vasc Surg 2002;24:239-44.
18) Giral P, Bruckert E, Dairou F, et al. Usefulness in predicting coronary artery disease by ultrasonic evaluation of the carotid arteries in asymptomatic hypercholesterolemic patients with po- sitive exercise stress tests. Am J Cardiol 1999;84:14-7.
19) Salonen R, Salonen JT. Progression of carotid atherosclerosis and its determinants: a population based ultrasonography study.
Atherosclerosis 1990;81:33-40.
20) Wendelhag I, Wiklund O, Wikstrand J. Atherosclerotic changes in the femoral and carotid arteries in familial hypercholeste- rolemia: ultrasonographic assessment of intima-media thickness and plaque occurrence. Arterioscler Thromb 1993;13:1404-11.
21) Tell GS, Howard G, McKinney WM, Toole JF. Cigarette smo- king cessation and extracranial carotid atherosclerosis. JAMA 1989;261:1178-80.
22) Gnasso A, Pujia A, Irace C, Mattioli PL. Increased carotid arte- rial wall thickness in common hyperlipidemia. Coron Artery Dis 1995;6:57-63.
23) Park NG, Choi KW, Kim HY, et al. Association of coronary artery disease with B-mode ultrasonographic intima-media thickness of the cartotid artery. Korean Circ J 1996;26:1012-9.
24) Joo SB, Choi YH, Choo JA, et al. The correlation between coronary artery disease and carotid atherosclerosis. Korean Circ J 1998;28:62-8.
25) Gnasso A, Irace C, Mattioli PL, Pujia A. Carotid intima-media thickness and coronary heart disease risk factors. Atherosclerosis 1996;119:7-15.
26) Park KR, Kim KY, Yoon SM, Bae JH, Seong IW. Correlation between intima-media thickness in carotid artery and extent of coronary atherosclerosis. Korean Circ J 2003;33:401-8.
27) Ogata T, Yasaka M, Yamagishi M, Seguchi O, Nagatsuka K, Minematsu K. Atherosclerosis found on carotid ultrasonography is associated with atherosclerosis on coronary intravascular ultrasonography. J Ultrasound Med 2005;24:469-74.