Preliminary Experience of Laparoscopic Hepatectomy for Hepatocellular Carcinoma
Purpose: Laparoscopic liver resection has gained much popularity in recent years, but relatively few centers have performed hepatectomies in hepatocellular carcinoma (HCC) patients due to the technical difficulties faced with underlying liver cirrhosis. We now present our early experience with laparoscopic liver resection in HCC performed in a single institution.
Methods: From October 2003 until March 2009, 39 laparoscopic liver resections were performed on HCC patients among whom 26 had underlying liver cirrhosis.
Results: The location of the tumor was in the left lateral section in 15, segment 5 or 6 in 20, segment 4 in 3 and caudate lobe in 1. Resection involving less than a monosegment was done in 26 and more than 2 segments in 13. Tumor size ranged from 0.8 cm to 6.6 cm (median 2.35) and the resection margin from 0.1 to 6 cm (median 1.5 cm). All patients were either stage I (29) or II (10). There was no difference between cirrhotic and non-cirrhotic patients in operation time (median 210 minutes, range 60∼637), change of hematocrit value (4.8%,
−1∼19.6%), or hospital stay (8 days, 3∼67 days). The median follow up duration was 15.1 months, and the 2-year recurrence free survival rate was 48.3%.
Conclusion: Laparoscopic liver resection in HCC with or without underlying cirrhosis seems to be feasible with minimal morbidity, especially in well selected cases with early stage HCC.
Gwan Chul Lee, M.D., Choon Hyuck David Kwon, M.D., Jae Won Joh, M.D., Jin Seok Heo, M.D., Gum O. Jung, M.D., Ju Ik Moon, M.D., Jong Man Kim, M.D., Mill Jae Shin, M.D., Moon Suk Choi, M.D.
1Departments of Surgery,
1Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine
Corresponding Author Choon Hyuck David Kwon Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50, Irwon-dong Gangnam-gu, Seoul 135-710, Korea
Tel: +82-2-3410-1281 Fax: +82-2-3410-0040 E-mail: [email protected]
*This paper has been presented at the 12th World Congress of Endoscopic Surgery, April 2010
*This paper was funded by Foundation for Corporate Collaboration,
Sungkyunkwan University
Key Words : Laparoscopy, Hepatectomy, Carcinoma, Hepatocellular
Received: 2010. 9. 27 Accepted: 2010. 12. 1
Introduction
Recently because of interest of minimally invasive surgery and development of operative procedures and devices,
laparoscopic surgery has been adopted in wider varieties of surgeries. However laparoscopic liver resection has been limited due to the technical difficulties and bleeding complications especially in patients with underlying liver cirrhosis.1,2 In particular, the risk of cancer cell dissemi-
nation when using laparoscopic liver resection in malignant tumors of the liver such as hepatocellular carcinoma (HCC) must be considered. Nevertheless, there have been several reports about the adequacy and safety of laparoscopic liver resection in HCC and some advocated routine laparoscopic procedure in lesions of left lateral section.3-7
We herein show the initial experience of laparoscopic liver resection for HCC in a single institution and evaluated the adequacy and safety of laparoscopic liver resection for HCC. We also evaluated the risk associated with laparosco- pic procedures in patients with underlying liver cirrhosis and assessed the recurrence and survival rate.
Methods
A retrospective analysis of 39 patients with laparoscopic liver resection for HCC from October 2003 to March 2009 at Samsung Medical Center, Seoul Korea was done. Among these, 26 patients had underlying liver cirrhosis.
1. Operative procedure
All liver resections were performed by totally laparosco- pic surgery method. For left side tumors (segment 2∼4) and caudate lobe tumors, the patient was placed in supine position, and the working ports were placed in described positions: 25 mm ports close to the subcostal margin at right anterior axillary line and left midclavicular line and a 12 mm main working between right midclavicular line and the umbilical port. In case an additional port was necessary, a 5 mm port was inserted just inferior of xyphoid process. For right side tumors (segment 5∼6), the patient was placed in left semi-lateral decubitus position and the ports were placed at right mid ∼ anterior axillary line close to the subcostal margin (5 mm), right anterior axillary line
∼ midclavicular line (main working port, 12 mm), and between left midclavicular line ∼ xyphoid process (5 mm).
The main working port was always inserted parallel to the line of liver resection margin. A 30 degree laparoscope was universally inserted through 10 mm port placed at
subumbilical area and pneumoperitoneum was established with carbon dioxide insufflation to a maximum pressure of 13 mmHg. To gain adequate resection margin, the laparoscopic USG (7.5 MHz; Aloka, Wallingford, CT) was used universally for segment V and VI lesions and whenever necessary for left side lesions.
Parenchymal resection was performed using Harmonic scalpel (Ethicon) or LigaSure (Tyco) until 2 cm depth from the capsule was reached, but for deeper parenchymal resection, combination of Cavitron Ultrasonic Surgical Aspirator (CUSA) with monopolar electrocautery nose cone and bipolar forceps was used. Small vessels were clipped with Endoclip (Autosuture), and for major vessel branches or small Glisson branches (<5 mm), Hem-o-lok (Weck Closure Systems) was used. For transaction of larger Glisson branches and major hepatic veins, EndoGIA 2.5 mm (Autosuture) or EchelonTM60 Endopath Stapler 2.5 mm was applied.
Routine use of Pringle maneuver was not done but we prepared for Pringle maneuver by applying looped sling using an umbilical tape when substantial amount of bleeding could be anticipated such as in patients with severe liver cirrhosis, resection of more than 2 segments or when the tumor was located close to a major vessel. Pringle maneuver was only applied when considerable bleeding was evident during parenchymal resection using a 5mm intestinal clamp through the left side 5 mm port by 15 minutes of occlusion and 5 minutes reperfusion.
CVP could not be monitored since central line is not routinely inserted at our institution during liver resection, but intraoperative fluid infusion was limited to about 500 ml/hr. Intraperitoneal pressure was maintain between 10∼
13 mmHg, which was tailored according to amount of bleeding and visibility of the operation field. Transeso- phageal ultrasonography was not used for monitoring of air embolism during operation.
2. Statistical analysis
Analysis software used by PASW 17.0 by SPSS, Inc.,
Table 1. Patients characteristics
Age (years), median (range) 54 (19∼75) Gender ratio (male : female) 32 : 7 Child Classification (A : B) 38 : 1 ICG15 (%), median (range) 9.95 (0.2∼69.3) Preoperative Laboratory result,
median (range)
Bilirubin (mg/dl) 0.8 (0.4∼3.1)
Albumin (g/dl) 4.1 (2.7∼5.1)
Prothrombin time (%) 87 (56∼99) Underlying liver cirrhosis
Cirrhosis 26 (67%)
Normal liver 13 (33%)
Fig. 1. Causes of hepatocellular carcinoma.
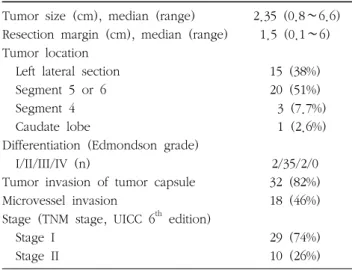
Table 2. Tumor characteristics
Tumor size (cm), median (range) 2.35 (0.8∼6.6) Resection margin (cm), median (range) 1.5 (0.1∼6) Tumor location
Left lateral section 15 (38%)
Segment 5 or 6 20 (51%)
Segment 4 3 (7.7%)
Caudate lobe 1 (2.6%)
Differentiation (Edmondson grade)
I/II/III/IV (n) 2/35/2/0
Tumor invasion of tumor capsule 32 (82%)
Microvessel invasion 18 (46%)
Stage (TNM stage, UICC 6
thedition)
Stage I 29 (74%)
Stage II 10 (26%)
Chicago, USA. Continuous variables were compared using the Mann-Whitney U test, survival rate was calculated by Kaplan-Meier method.
p
-value less than 0.05 was consi- dered statistically significant.Results
The median age was 54 year (19∼75) with 32 male and 7 female patients. All patients were Child-Pugh A, except for one B and the median value of 15 minutes indocyanin green test was 9.95% (0.2∼69.3%) (Table 1). Thirty-five patients had hepatitis B, 1 hepatitis C, 2 alcoholic liver disease and in 1 patient the etiology was unknown (Fig.
1). Underlying liver cirrhosis was present in 26 patients (66.6%).
The location of the tumor was in left lateral section in
15, segment V or VI in 20, segment IV in 3, and caudate lobe in 1. Resection involving less than monosegment was done in 26 and more than 2 segments in 13. Tumor size ranged from 0.8 cm to 6.6 cm (median 2.35) and resection margin from 0.1 to 6 cm (median 1.5 cm). Other tumor characteristics are well described in Table 2. Overall, 29 patients had stage I HCC according to the TNM stage (UICC 6th edition) and 10 had stage I.
Median operative time was 210 minutes (60∼460). Two patients underwent open conversion; one due to uniden- tifiable mass after resection and one due to intraoperative bleeding who was the only patient that required transfusion (Table 3). Although intraoperative air embolism could not be evaluated exactly, no patients showed signs or symp- toms of air embolism such as dypnea or drop of blood pressure.
Pringle maneuver was applied on 10 patients. The procedure was applied selectively on patients whom excessive bleeding could be anticipated such as severe liver cirrhosis on laparoscopic examination, tumors in difficult locations or major hepatic resections. There was no difference in change of hematocrit between patients that underwent Pringle maneuver and patients that did not (Table 4).
The median hospital stay was 8 days (range 3∼67 days).
Postoperative complication was present in 4 patients; 1
Table 4. Comparison of operative results between cirrhotic and non-cirrhotic patients
Cirrhosis (n=26) Non-cirrhosis (n=13) p-value Operation time (minutes), median (range)
Applicationof inflow occlusion
Mean duration of inflow occlusion (minutes) Median change of hematocrit before and 7 days after operation (range)
215 (120∼637) 19.2% (5/26)
29 5.0 (1.2∼19.6)
190 (60∼330) 38.5% (5/13)
57 4.7 (−1∼10.2)
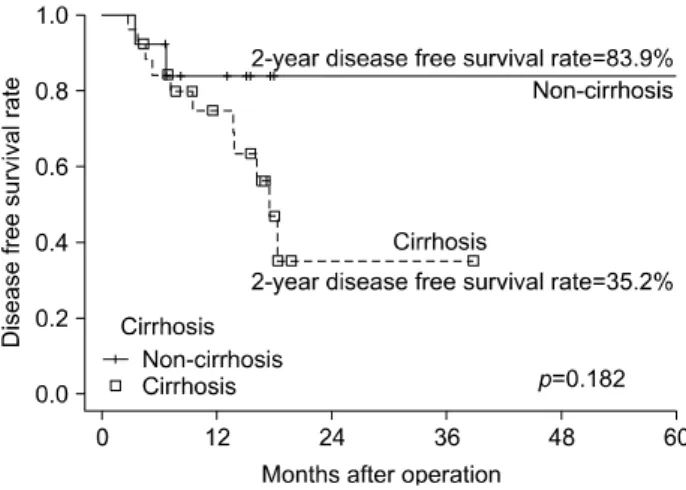
0.239 0.253 0.173 0.348 Fig. 2. Overall recurrence free survival rate.
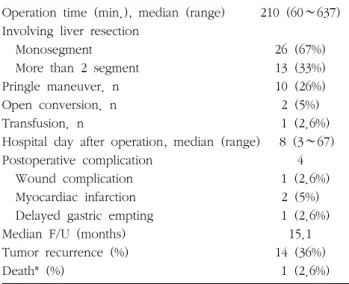
Table 3. Intraoperative and postoperative results
Operation time (min.), median (range) 210 (60∼637) Involving liver resection
Monosegment 26 (67%)
More than 2 segment 13 (33%)
Pringle maneuver. n 10 (26%)
Open conversion. n 2 (5%)
Transfusion. n 1 (2.6%)
Hospital day after operation, median (range) 8 (3∼67)
Postoperative complication 4
Wound complication 1 (2.6%)
Myocardiac infarction 2 (5%)
Delayed gastric empting 1 (2.6%) Median F/U (months) 15.1
Tumor recurrence (%) 14 (36%)
Death* (%) 1 (2.6%)
*1 case of death occurred at postoperative 58 months
wound complication, 2 postoperative myocardial infarctions (MI), and 1 delayed gastric empting. One patient with MI was 73 years old with a past history of hypertension, diabetes and coronary arterial disease treated with stent insertion 2 years prior to surgery. He developed MI soon after operation but recovered without complication after balloonplasty performed on 8th postoperative day. The other patient with MI had no previous history of coronary arterial disease and recovered without sequelae after conservative management and was discharged on postoperative day 8. One patient with delayed gastric emptying had history of diabetes for more than 20 years, and was diagnosed with delayed gastric emptying before operation. His hospital stay was prolonged up to 67 days due to poor oral intake after operation but eventually recovered and is well at the present time.The median follow up period was 15.1 months. One and 3 years recurrence free survival rate was 81.3% and 48.3%
respectively (Fig. 2). There was no difference in recurrence free survival rate between stage I patients and stage II (
p
-value=0.745) (Fig. 3). Recurrence free survival rate of non-cirrhotic patients was superior to cirrhotic patients (83.9% versus 35.3% at 3 years) but it did not have statistical significance (p
-value=0.182) (Fig. 4). Among the cohort, only one patient died due to progression of hepatocellular carcinoma 58 months after initial resection, so the overall patient survival could not be evaluated fully.The recurrence site of all 12 patients was the liver except for 2 patients who had intraperitoneal drop metastasis (Table 3). One patient with drop metastasis recurred 69 months after liver resection and metastectomy was successfully performed laparoscopically. The other patient recurred 7 months after resection, and laparotomy was performed to remove the drop metastasis. Both patients are currently well without recurrence. All patients with
Fig. 3. Recurrence free survival rate according to tumor stage. Fig. 4. Recurrence free survival rate of patients according to underlying liver cirrhosis.
intrahepatic metastasis underwent transarterial chemoembo- lization and one patient received a liver transplant.
Discussion
Laparoscopic approach has gained much popularity during recent years and many centers are now reporting about the safety and feasibility of laparoscopic liver resections. In the past, due to the restricted surgical field and the complexity of surgical procedures during laparo- scopic approach, laparoscopic liver resection required a much longer operation time.8,9 However much progress has been made during the last decade and many surgeons now report no difference in operation time between open and laparoscopic approach.10,11 Although our study did not compare the operation time with open approach, the median operation time was only 210 minutes which is similar with previous reports. The hospital stay was also relatively short with a median of 7 days and we can conclude that laparoscopic liver resection is feasible in selected cases.
Although laparoscopic liver resection has been histori- cally applied to non-malignant conditions,12-14 many studies have recently been published on malignant diseases.
Cancer dissemination has been of primary concern in these situations. According to Kaneko and collegues,15 laparo- scopic liver resections has been successfully performed in
HCC patients, and they reported no difference in operation time, bleeding amount as well as overall survival and recurrence free survival between open and laparoscopic method. Chen and collegues16 reported a 5 year survival rate of 59.4% in patients undergoing laparoscopic liver resection of less than 2 segments, and 61.7% in resection of more than 2 segments Furthermore, Lai and colleagues showed 5 year recurrence free survival of 50% and 5 year overall survival of 36%.17 The safety and feasibility of laparoscopic liver resection for HCC has also been reported in Western countries.3 Comparing our results to the historical data, recurrence free survival was comparable with a 3 years recurrence free survival of 48.3%. Intere- stingly, there were 2 intraperitoneal drop metastasis, a form of recurrence pattern not frequently observed in open liver resection, which may have occurred due to the laparo- scopic resection technique, and warrants our attention.
Fortunately, both patients received metastectomy and both are currently without recurrence. Although there are limitations due to the short median follow up duration of only 15.1 months, the overall patient survival seems superior, with only one patient death at 58 months after initial resection, resulting in survival rate of 97.4%. A longer duration of follow up is necessary to draw a firm conclusion.
According to the French group, laparoscopic liver
resection has the advantage of less ascites and less loss of liver function compared to open method.18 Although we did not compare these factors in our study, patients with underlying cirrhosis did not differ in operation time, frequency of inflow occlusion used, duration on inflow occlusion, or median change of hematocrit compared to non-cirrhotic patients supporting the feasibility of laparo- scopic approach in cirrhotic patients. However, an interest- ing observation was the difference of recurrence free survival rate between the 2 groups, 83.9% at 2 years for non-cirrhotic compared to 35.2% in cirrhotic patients, even though there was no statistical difference in this study.
Cirrhosis is a well known risk factor of recurrence, but this difference in recurrence free survival rate warrants our attention and further study with a larger patient population and a longer follow is definitely needed to draw a conclusion.
Conclusion
Although our study is limited with a short follow up and small number of patients, we can carefully conclude from our initial results that laparoscopic liver resection in HCC with or without underlying cirrhosis seems to be feasible with minimal morbidity in well selected cases with early stage HCC. Since laparoscopic liver resection is a highly technically demanding operation with a long learning curve, with accumulation of experience, we hope that in the near future we will be able to achieve even better results. Nonetheless, a well designed study with a larger patient population and longer follow up will be needed to draw a final conclusion.