대한안과학회지 2013년 제 54 권 제 6 호 J Korean Ophthalmol Soc 2013;54(6):987-993 pISSN: 0378-6471 eISSN: 2092-9374 http://dx.doi.org/10.3341/jkos.2013.54.6.987
= 증례보고 =
뇌실주위백질연화증 환자에서 동반된 시신경 위축과 시야 결손 1예
김호윤⋅최희영⋅이지웅 부산대학교 의학전문대학원 안과학교실
목적: 하부시야결손을 주소로 내원한 22세 여자환자에서 동반된 뇌실주위백질연화증 1예를 경험하였기에 이를 보고하고자 한다.
증례요약: 22세 여자 환자가 시력교정수술을 위해 방문한 개인안과에서 양안의 시신경 위축과 시야검사 후 양안 하부시야결손이 발견 되어 정상안압녹내장으로 진단받고 의뢰되었다. 최대교정시력은 양안 1.0 이었고 안압은 양안 16 mmHg이었다. 양안의 유두함몰비는 정상이었으나 이측 유두부에 시신경의 창백 소견이 관찰되었다. 흑백안저사진과 빛간섭단층촬영검사에서 상이측 망막신경섬유층 결 손이 관찰되었다. 시야검사에서는 양안 하부시야결손이 나타났다. 출생시 재태기간은 34주, 출생체중은 1600그램으로 미숙아 및 저체 중아 과거력이 있었고, 뇌자기공명영상검사에서 양측 뇌실주위백질연화증이 관찰되었다.
결론: 양안의 시신경 위축과 하부시야결손으로 정상안압녹내장으로 진단받았던 환자에서 뇌실주위백질연화증을 경험하였다. 저체중 출생 또는 미숙아 과거력을 가지고 특이적 녹내장성 변화를 보이지 않는 시야 결손을 보이는 경우, 원인으로 안질환 이외의 뇌병변을 고려해야 하고 뇌자기공명영상 검사가 진단에 도움이 될 수 있음을 알 수 있었다.
<대한안과학회지 2013;54(6):987-993>
■ Received: 2012. 10. 20. ■ Revised: 2012. 12. 30.
■ Accepted: 2013. 3. 23.
■ Address reprint requests to Ji Woong Lee, MD, PhD Department of Ophthalmology, Pusan National University Hospital, #179 Gudeok-ro, Seo-gu 602-739, Busan Tel: 82-51-240-7319, Fax: 82-51-240-7341 E-mail: [email protected]
극소저체중출생아의 생존율이 높아짐에 따라 뇌성마비 와 같은 강직성 운동장애 및 인지학습장애를 포함하는 심 각한 만성 신경학적 합병증이 문제되고 있다.1,2뇌실주위백 질연화증은 이러한 신경학적 합병증의 중요한 원인이고, 극 소저체중출생아의 2.6-29%에서 뇌실주위백질연화증이 발 생한다고보고되었다.3,4 뇌실주위백질연화증은 임신 제2삼 분기 후기나 제3삼분기 초기에 뇌 혈류의 감소로 인한 산소 결핍에 의해 발생한다.5,6 병변은 흔히 가쪽뇌실의 삼각부 (trigone) 근처에 호발하며, 드물게 뇌실간공 주변에 발생 한다.5,6뇌실간공 주변의 피질척수섬유가 영향을 받아 뇌성 마비와 같은 강직성 운동장애가 발생하고,6 가쪽뇌실의 삼 각부와 근접한 시각로부챗살의 손상으로 시각장애가 발생 한다.7
국외에서 재태기간 32주에 출생한 13세 남아에서 발견 된 뇌실주위백질연화증에 동반된 시야장애가 보고되었으 나,8국내에서는 뇌실주위백질연화증에 동반된 시야장애에 대한 보고가 없었다. 이에 저자들은 양안의 정상안압녹내장 으로 진단받은 22세 여자환자에서 시신경 위축과 시야 결
손을 동반한 뇌실주위백질연화증 1예를 경험하였기에 보고 하는 바이다.
증례보고
22세 여자가 레이저 시력교정수술을 시행 받기 위해 내 원한 개인 안과에서 양안의 하부 시야결손과 시신경위축이 발견되었으며, 정상 안압과 개방된 전방각 소견을 바탕으로 양안의 정상안압녹내장으로 진단받고 본원에 의뢰되었다.
최대교정시력은 양안 1.0 이었고 구면렌즈대응치는 우안 -6.25 디옵터, 좌안 -6.75 디옵터였다. 안압은 양안 16 mmHg이었고 중심각막두께는 우안 557 μm, 좌안 561 μm, 안축장의 길이는 우안 26.24 mm, 좌안 26.19 mm로 측정 되었다. 아침 9시부터 오후 5시까지 2시간 간격으로 5회 안 압을 측정하였고 이 평균 안압은 우안 16.3 mmHg, 좌안 15.7 mmHg이었고, 모든 측정값은 21 mmHg 이하였다.
안저검사에서 양안 이측 유두부에 시신경의 창백소견을 보였고 상이측의 망막신경섬유층 위축이 관찰되었으나, 유 두함몰비는 우안 0.36, 좌안 0.34로 정상이었고, 신경망막 테의 패임이나 시신경출혈 등의 전형적인 녹내장성 시신경 손상은 보이지 않았다(Fig. 1).
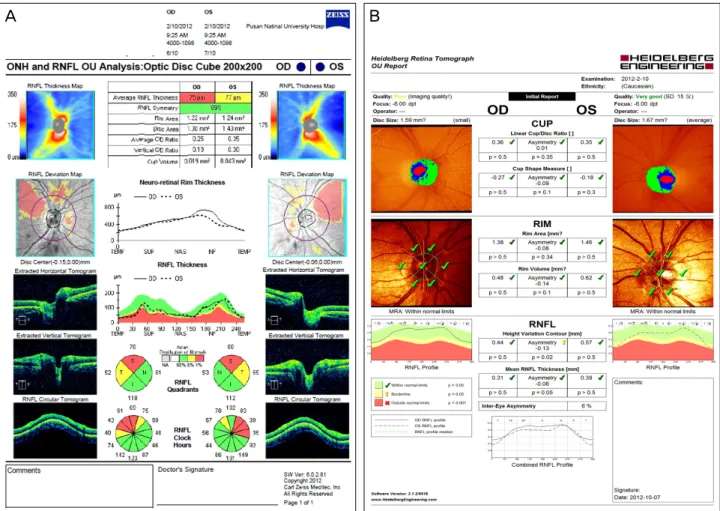
스펙트럼도메인 빛간섭단층촬영기(Optical Coherence Tomography, Cirrus HD-OCT, Carl Zeiss, Meditec Inc., Dublin, USA) 검사에서 양안에서 상이측 망막신경섬유층
A B
C D
Figure 1. Retinal nerve fiber layer (RNFL) and color fundus photographs of the patient at initial visit. Cup-disc ratio is 0.36 in the
right eye (A) and 0.34 in the left eye (B). Optic discs have temporal pallor in both eyes. Superotemporal RNFL defects with intact neuroretinal rim in the both eyes (C, D).의 두께가 감소되어 있었다. 레이저 시신경유두 분석기 (Heidelberg Retina Tomography, HRT Ⅲ, Heidelberg Engineering GmbH. Heidelberg. Germany) 검사에서 양안 망막신경섬유층 결손이 있음에도 불구하고 시신경의 6개 구역에서 Moorfield Regression Analysis (MRA)의 이상 이 발견되지 않아 신경망막테가 정상범위에 있음을 시사하 였다(Fig. 2). 레이저 시신경유두 분석기 에서 시신경유두 면적은 우안은 1.59 mm2, 좌안은 1.67 mm2였다. 자동 시 야검사에서 양안의 하측 시야결손이 관찰되었다(Fig. 3).
한식 색각검사에서 양안 정상 소견을 보였고 상대구심성동 공운동장애는 관찰되지 않았다. 시유발전위검사에서 우안 에 비해 좌안의 P100 파의 진폭 감소 및 잠복시간의 지연 이 관찰되었다.
환자의 과거력에서 쌍생아 중 첫째로 재태기간은 34주, 출생체중은 1600그램이었다. 출생 후 18개월에 보행장애 를 보였다.
전형적인 녹내장성 시신경 변화와는 다르게 시신경은 창백하였으나 시신경유두함몰비는 정상이었고, 신경망 막테의 패임, 시신경출혈은 동반하지 않았다. 또한 미숙 아, 저체중 출생, 보행장애의 과거력이 있어, 비녹내장성 시신경병증과의 감별진단을 위하여 뇌자기공명영상 검 사를 시행하였다. 뇌자기공명영상 검사에서 시각로부챗 살 과 앞쪽 피질척수섬유 부위의 백질에 조영이 증가된 양상을 보였고, 뇌실은 뇌실 주위 백질의 위축으로 커져 있는 양상이 관찰되었다(Fig. 4). 환자는 미숙아에서 발 생한 뇌실주위 백질연화증에 동반된 시신경위축과 시야 결손으로 진단을 내리고 안압하강제 치료 없이 경과 관 찰하기로 하였다.
고 찰
본 증례에서처럼 시신경위축과 시야검사에서 시야결손
- 김호윤 외 : 뇌실주위백질연화증과 시야 결손 -
Figure 2. Optical coherence tomography (OCT) (A) and Heidelberg retinal tomography (HRT) (B). Superotemporal retinal nerve fi-
ber layer (RNFL) defects were detected in the RNFL thickness deviation map on OCT with normal Moorfield Regression Analysis (MRA) on HRT in both eyes.이 관찰되고 개방된 전방각, 21 mmHg 이하의 안압을 나타 낼 때 정상안압녹내장이 그 원인으로 고려될 수가 있다. 하 지만 정상안압녹내장으로 진단받기 위해서는 시야결손의 원인이 될만한 안질환이나 전신질환이 없는 상태가 전제가 되어야 함에도 불구하고, 안질환 이외의 평가는 그에 상응 하는 증상이 나타나지 않는 한 간과되고 녹내장으로 진단 된 후 치료 중 시행되어지기도 한다.
녹내장에 의한 시신경 함몰은 하측 시신경 함몰이 뚜렷 한데 반해 비녹내장성 시신경함몰은 신경망막테 감소가 전 반적으로 뚜렷하며 본 증례에서처럼 함몰보다는 창백소견 이 더 명백한 특징이 있다.9
정상안압녹내장과 비녹내장성 시신경위축을 나타낼 수 있는 질환을 감별해야 하는 경우는 다음과 같다. 50세 이하 에서 녹내장 진단을 받았거나 두통이 동반되거나 국소적인 신경학적 증상이 동반된 경우, 색각검사 이상, 신경망막테 의 창백, 비대칭적 함몰, 시신경유두함몰과 시야검사결과의 불일치 등의 소견이 있는 경우 감별 진단을 위하여 신경학 적 영상검사를 시행하여야 한다.9
본 증례에서 환자의 나이는 22세로 젊은 나이였고 양안 에서 전반적인 망막신경섬유층 결손이 관찰되었으나, 시신 경유두함몰비는 정상이었고 시신경 이측부위가 창백하였 다. 또한 신경망막테의 패임, 시신경 출혈과 같은 전형적인 녹내장성 손상을 동반하지 않았다는 점이 녹내장성 시신경 손상과 다른 점이라 할 수 있다. 이상의 소견은 OCT와 HRT검사에서도 확인되었다. 양안 모두 OCT에서 망막신경 섬유층의 결손이 관찰되었으나, HRT의 MRA 상 정상으로 신경망막테가 정상범위안에 있음을 시사하였다.
뇌실주위백질연화증은 재태기 24주에서 34주 사이에 성 숙하지 못한 뇌에 일어나는 허혈성 뇌실주위백질 손상으로 발생한다.5,6국외 보고에 따르면 미숙아의 32%에서 뇌실주 위백질연화증을 관찰되었다.5다른 보고에 따르면 뇌실주위 백질연화증 환자 중 20%에서 시야장애를 호소하며,10대칭 적 하부 시야 결손을 보인다.11 시야결손에도 불구하고 정 상시력을 보일 수 있다.12
뇌실주위백질연화증 환자에서 가쪽뇌실의 삼각부와 근 접한 시각로부챗살의 손상으로 시야장애가 발생한다.7 본
A B
Figure 3. Automated visual field examinations showed bilateral inferior visual field defect in the left eye (A) and right eye (B).
Figure 4. The patient’s brain MRI. Magnetic resonance imag-
ing (fluid-attenuated inversion recovery sequence) shows high signal intensity in the optic radiations (black arrows) and the corticospinal pathways (white arrow). Posterior ventricles were enlarged.증례에서도 가쪽뇌실의 삼각부와 근접한 시각로부챗살의 손상이 뇌자기공명영상검사에서 확인되었다.
뇌실주위백질연화증에서는 시야장애 이외의 군집현상, 시지각장애 등이 동반될 수 있다.13 뇌실주위백질연화증 환자는 대부분 시야결손을 보였고,14약시가 12-67%에서 관찰되었다.13,15그 외 이들은 시각 지각인식 결핍 및 시각 발달지연이 보이고 사시, 특히 내사시가 관찰되며,16 대부 분 안진을 동반된다.17 색각인지는 정상에 가까운 소견을 보인다.18
본 증례에서는 시야장애 이외의 약시, 사시 및 색각이상 은 관찰되지 않았다. 그러나 대다수의 뇌질주위백질연화증 환자에서 상기 증상이 동반되는 경우가 많으므로 이에 대 한 평가가 필요하다.
시신경위축, 시신경 형성부전을 동반한 뇌실주위백질연 화증과 정상안압녹내장을 감별하는 것은 중요하다. 뇌실주 위백질연화증 환자에서는 두가지 다른 형태의 시신경 양상 이 관찰될 수 있다.19Jacobson et al20에 의하면 뇌실주위백 질연화증에서 양안의 시신경유두의 크기는 정상이면서, 신 경망막테가 감소하여 유두함몰비가 비정상적으로 큰 시신 경형성부전의 양상이 관찰된다. 이러한 시신경의 양상은 공
A B
- 김호윤 외 : 뇌실주위백질연화증과 시야 결손 -
막 터널이 정상 직경으로 발달된 후 시각로부챗살에 손상 이 발생하여 일어난 역행 연접횡단 변성의 결과로 설명된 다.20만약 뇌실주위백질연화증을 보이는 환자의 시신경에 서 상기의 이유로 유두함몰비가 증가되어 있다면, 정상안 압녹내장과의 감별이 어렵다. 이런 경우 미숙아의 과거력, 정상 안압, 특징적인 대칭적 하부 시야 결손으로 녹내장성 시신경 위축과 뇌실주위연증을 구별하는데 도움이 될 수 있다.
이와는 다르게 뇌실주위백질연화증에서 공막터널이 정 상적인 크기로 발생하기 전 시각로 부챗살에 손상이 일어 난다면 본 증례처럼 유두함몰비의 증가 없이 전반적인 시 신경형성부전 또한 발생할 수 있다.21
본 증례의 경우 레이저시신경유두 분석기에서 시신경유 두면적은 우안은 1.59 mm2, 좌안은 1.67 mm2였고, 이전의 20대 정상 한국인 남녀의 시신경유두 분석에 대한 연구의 결과와 비교하였을 때, 정상보다 작은 시신경유두 면적을 가진 것으로 판단되었다.22
안증상 이외에 뇌성마비, 정신지체를 포함한 발달지체, 그 외 행동문제가 발생할 수 있다. 뇌질주위백질연화증이 확인된 환자중 70%에서 뇌성마비가 발생했다는 보고가 있으며,23대부분의 경우 하지의 신경 분포가 되어 있는 내 측피질척수로가 영향을 받고 그 결과 강직성 하지마비가 나타난다.24본 증례에서도 환자는 양측 하지 근력 운동 저 하를 동반한 보행장애를 가지고 있었고, 뇌자기공명영상 검사에서 뇌실간공 주변의 앞쪽 피질척수섬유의 손상이 확인되었다.
뇌실주위백질연화증의 영상학적 진단은 초음파검사, 전 산화단층촬영, 자기공명영상을 주로 이용하고 있다. 신생아 시기의 초기 진단을 위해서는 뇌초음파 검사가 널리 유용 하게 사용되고 있으나,25뇌자기공명영상 검사가 백질 손상 범위를 가장 예민하게 판단할 수 있다.10뇌 자기공명영상 검사는 출산전 및 출산중의 허혈성 손상의 종류, 부위, 범위 를 결정하는데 가장 민감한 검사이다.10 이전의 여러 연구 에서 심각한 뇌실주위백질연화증의 경우, 시야장애와 자기 공명영상상의 해부학적 이상의 결과가 상호 관계를 보인다 고 보고하였다.26 그러나 시각피질이나 시각로부챗살의 병 변이 없는 시야 장애의 경우 망상체-슬상체-선조피질 통 로와 다른 뇌 부위의 손상이나 동안신경 장애와 같은 다른 신경학적 장애로 설명될 수 있다.
뇌실주위백질연화증이 주로 가쪽뇌실의 삼각부와 근접 한 시각로부챗살과 뇌실간공 주변의 피질척수섬유에서 발 생하고, 뇌자기공명영상 검사에서 T2 flair 강조영상상 뇌 실주위 고음영을 보이며 뇌실주위 백질 위축으로 뇌실확장 소견이 관찰된다.
뇌실주위연화증이 신생아기에 진단되었을 경우 신경학 적 손상 정도를 파악하는 것은 어렵다. 그리고 광범위한 뇌 병변을 보이는 미숙아라 할지라도 특징적인 근력저하를 보 이는 경우가 드물다. 이 경우 시간유발전위검사, 청각뇌간 반응검사 및 뇌파검사 등이 이용된다.27
본 증례를 통하여 양안의 정상안압녹내장으로 진단된 환 자에서 시신경위축과 시야결손이 뇌실주위백질연화증과 동 반하여 발생할 수 있음을 알 수 있었다. 양안의 시신경위축 과 시야결손을 보이는 환자에서 50세 이전의 발병, 저체중 출생이나 미숙아의 과거력, 보행장애, 시신경 유두 창백 등 의 비특이적인 임상양상을 보이는 경우 동반된 뇌병변을 고려하여 뇌에 대한 영상학적 검사를 시행하는 것이 진단 및 치료에 도움을 줄 수 있을 것으로 생각한다.
REFERENCES
1) Miller SP, Ferriero DM, Leonard C, et al. Early brain injury in pre- mature newborns detected with magnetic resonance imaging is as- sociated with adverse early neurodevelopmental outcome. J Pediatr 2005;147:609-16.
2) Litt J, Taylor HG, Klein N, Hack M. Learning disabilities in chil- dren with very low birthweight: prevalence, neuropsychological correlates, and educational interventions. J Learn Disabil 2005;
38:130-41.
3) Hernández-Cabrera MA, Flores-Santos R, García-Quintanilla JF, et al. Periventricular leukomalacia prevalence in premature newborn.
Rev Med Inst Mex Seguro Soc 2009;47:147-50.
4) Liu J, Li J, Qin GL, et al. Periventricular leukomalacia in pre- mature infants in mainland China. Am J Perinatol 2008;25:535-40.
5) Olsén P, Pääkkö E, Vainionpää L, et al. Magnetic resonance imag- ing of periventricular leukomalacia and its clinical correlation in children. Ann Neurol 1997;41:754-61.
6) Jacobson L, Hård A-L, Svensson E, et al. Optic disc morphology may reveal timing of insult in children with periventricular leuco- malacia and/or periventricular haemorrhage. Br J Ophthalmol 2003;87:1345-9.
7) Fazzi E, Bova SM, Uggetti C, et al. Visual-perceptual impairment in children with periventricular leukomalacia. Brain Dev 2004;26:
506-12.
8) Brodsky MC. Periventricular leukomalacia: an intracranial cause of pseudoglaucomatous cupping. Arch Ophthalmol 2001;119:626-7.
9) Allingham RR, Damji KF, Freedman S, et al. The clinical form of glaucoma. Shields’ textbook of glaucoma. 6th ed. Philadelphia:
Lippincott Williams & Wilkins, 2011; chap. 11.
10) Cioni G, Fazzi B, Coluccini M, et al. Cerebral visual impairment in preterm infants with periventricular leukomalacia. Pediatr Neurol 1997;17:331-8.
11) Brodsky MC. Congenital optic disc anomalies. In: Pediatric Neuro- Ophthalmology, 18th ed. Springer, 2010; v. 18. chap. 2.
12) Fazzi E, Bova S, Giovenzana A, et al. Cognitive visual dysfunc- tions in preterm children with periventricular leukomalacia. Dev Med Child Neurol 2009;51:974-81.
13) Park SJ, Chang BL. Strabismus, amblyopia and refractory errors in
patients with cerebral palsy. J Korean Ophthalmol Soc 1999;40:
2898-903.
14) Keith CG, Kitchen WH. The significance of ocular morbidity in very-low-birthweight infants to the Australian health service. Aust J Ophthalmol 1983;11:29-31.
15) Khetpal V, Donahue SP. Cortical visual impairment: etiology, asso- ciated findings, and prognosis in a tertiary care setting. J AAPOS 2007;11:235-9.
16) Jacobson L, Ygge J, Flodmark O, Ek U. Visual and perceptual characteristics, ocular motility and strabismus in children with per- iventricular leukomalacia. Strabismus 2002;10:179-83.
17) Jacobson L, Ygge J, Flodmark O. Nystagmus in periventricular leucomalacia. Br J Ophthalmol 1998;82:1026-32.
18) Jacobson LK, Dutton GN. Periventricular leukomalacia: an im- portant cause of visual and ocular motility dysfunction in children.
Surv Ophthalmol 2000;45:1-13.
19) Brodsky MC. Semiology of periventricular leucomalacia and its optic disc morphology. Br J Ophthalmol 2003;87:1309-10.
20) Jacobson L, Hellström A, Flodmark O. Large cups in normal-sized optic discs: a variant of optic nerve hypoplasia in children with per- iventricular leukomalacia. Arch Ophthalmol 1997;115:1263-9.
21) Brodsky MC, Glasier CM. Optic nerve hypoplasia. Clinical sig-
nificance of associated central nervous system abnormalities on magnetic resonance imaging. Arch Ophthalmol 1993;111:66-74.
22) Lee DW, Ahn HB, Roh SH. Topographic measurement of the optic nerve head with confocal scanning laser tomography in normal third decade of Korean. J Korean Ophthalmol Soc 1999;40:489- 95.
23) Minagawa K, Tsuji Y, Ueda H, et al. Possible correlation between high levels of IL-18 in the cord blood of pre-term infants and neo- natal development of periventricular leukomalacia and cerebral palsy. Cytokine 2002;17:164-70.
24) Mewasingh LD, Demil A, Christiaens FJ, et al. Motor strategies in standing up in leukomalacic spastic diplegia. Brain Dev 2002;
24:291-5.
25) Flodmark O, Roland EH, Hill A, Whitfield MF. Periventricular leukomalacia : radiologic diagnosis. Radiology 1987;162(1 Pt 1):
119-24.
26) Lee YS, Yoo DS. Cystic periventricular leukomalacia in the neo- nate: analysis of sequential sonographic findings and neurologic outcomes. J Korean Radiol Soc 2003;49:57-62.
27) Park HK. Hypoxic-ischemic encephalopathy in premature infants:
update on periventricular leukomalacia. Korean J Perinatol 2009;
20:106-13.
=ABSTRACT=
A Case of Optic Atrophy and Visual Field Defect in Periventricular Leukomalacia
Ho Yun Kim, MD, Hee Young Choi, MD, PhD, Ji Woong Lee, MD, PhD
Department of Ophthalmology, Pusan National University School of Medicine, Busan, Korea
Purpose: To report a case of visual field defect and optic atrophy in a patient with periventricular leukomalacia.
Case summary: A 22-year-old woman was referred to our hospital for further glaucoma evaluation. She was diagnosed with normal tension glaucoma by her local ophthalmologist. Best corrected visual acuity and intraocular pressure were 1.0 and 16 mm Hg in both eyes, respectively. Fundus examination showed a cup disc ratio of 0.36 in the right eye and 0.34 in the left eye. However, the optic disc had temporal pallor. Red-free photograph and optical coherence tomography showed supratemporal retinal nerve fiber layer atrophy. Visual field examinations revealed inferior visual field defect in both eyes.
The patient was born at 34 weeks of gestation with a birth weight of 1600 g. Brain magnetic resonance imaging (MRI) showed periventricular leukomalacia.
Conclusions: The author presents a case of periventricular leukomalacia with inferior visual field defect and optic atrophy in a patient who was previously diagnosed with glaucoma. If non-specific clinical features that differ from typical glaucoma- tous clinical features are observed in a patient with a history of prematurity, a brain MRI can aid the diagnosis.
J Korean Ophthalmol Soc 2013;54(6):987-993
Key Words: Optic atrophy, Periventricular leukomalasia, Visual field defect
Address reprint requests to Ji Woong Lee, MD, PhD
Department of Ophthalmology, Pusan National University Hospital
#179 Gudeok-ro, Seo-gu 602-739, Busan
Tel: 82-51-240-7319, Fax: 82-51-240-7341, E-mail: [email protected]
- 김호윤 외 : 뇌실주위백질연화증과 시야 결손 -