63
• 교신저자: 조용현, 가톨릭대학교 의과대학 비뇨기과학교실 서울시 영등포구 여의도동 62번지
우150-896 Tel: 02-3779-1024, Fax: 02-761-1626 E-mail: [email protected]
Received: February 28, 2010 / Accepted: March 29, 2010
전립선검진을 위해 내원한 성인 남성에서 배뇨 후 잔뇨량과 요로감염과의 상관관계
가톨릭대학교 의과대학 비뇨기과학교실
임승혁∙하유신∙손동완∙조용현 [Abstract]
The Correlation between Post-void Residual Urine Volume and Urinary Tract Infection in Asymptomatic Men Visited for Prostate Examination
Seung Hyuk Yim, U-Syn Ha, Dong Wan Sohn, Yong-Hyun Cho
From the Department of Urology, College of Medicine, The Catholic University of Korea, Seoul, Korea
Purpose: The large post-void residual urine (PVR) could be related to various complications, especially urinary
tract infections (UTIs). Although numerous cut-off value of PVR related to UTIs have been proposed there is still debate on that. We investigated the correlation between PVR and UTIs.
Materials and Methods: From January 2008 to December 2008, retrospective analysis was performed on 351
asymptomatic male patients who visited our clinic for prostate examination. The prostate specific antigen (PSA) level, peak urine flow rate, PVR, voided urine volume, International Prostatic Symptom Score (IPSS) and urine culture results were obtained. PVR was measured by portable bladder scanner. A positive result of urine culture was defined as growth of more than 100,000 bacteria per ml. We investigated the association between urine culture results and PVR, and estimated cut-off value of PVR predicting bacteriuria using ROC analysis.
Results: The mean age of patients was 63.3±10.4years and 8.83% of the total patients (31 patients) showed
positive in urine culture. Mean PVR volume was significantly higher in the group with positive urine culture compare to the group with negative urine culture (105.6mL vs 41.8mL, p<0.001), but we couldn't validate cut-off value of PVR for predicting UTIs.
Conclusions: Significant bacteriuria was found in 8.83% of the asymptomatic male patients. Although the
positive relationship between PVR and the risk of UTIs was found we couldn't validate cut-off value of PVR for predicting UTIs. (Korean J UTII 2010;5:63-67)
Key Words: Urination, Residual volume, Urinary tract infection
서 론
남성에서 배뇨 후 잔뇨는 주로 전립선비대증에 의한 방광출구폐색에 의해 발생하는 합병증이며, 전 립선암, 요로감염, 요로손상, 약물, 신경학적 이상에 따른 배뇨장애 및 수술 후 합병증으로 인하여 발생 할 수 있다.
1배뇨 후 잔뇨량이 많은 경우 요로감염, 방광결석, 방광충만에 기인한 상행감염 혹은 수신증 에 의한 신기능손상 등의 다양한 합병증이 나타날 수 있으며, 특히 요로감염의 발생 위험이 높은 것으 로 알려져 있다.
1최근 여러 연구에서 요로감염에 관련된 잔뇨량의 절단치 (cut-off value)를 제시하고 있으나, 아직 공인된 결과는 없는 실정이다. 1978년 에 Abrams 등
2이 제시한 300ml의 절단치가 정설로 받아들여졌으나, 2008년에 Truzzi 등
3은 ROC 회귀분 석을 이용하여 180ml의 잔뇨량이 87%의 민감도와 98.5%의 특이도를 나타내는 요로감염 발생의 예측 인자가 된다고 발표하였다. 2009년에 May 등
4은 요 로감염 환자에서 배뇨 후 잔뇨량이 의미 있게 높긴 하나 (113 vs 41ml, p<0.001) 요로감염에 대한 배뇨 후 잔뇨량의 절단치를 결정할 수는 없다고 하였다.
이에 저자들은 지난 1년 동안 본원 외래에서 전 립선 검진을 받은 무증상의 환자를 대상으로 배뇨 후 잔뇨량과 요로감염의 상관관계를 알아보고자 하 였다.
대상 및 방법
2008년 1월부터 12월까지 1년간 전립선 검진을 위해 본원 외래에 내원한 351명의 요로감염증상이 없는 환자를 대상으로 하였으며, 전립선특이항원, 최대요속, 배뇨 후 잔뇨량, 요배양검사, 국제전립선 증상점수 등을 의무기록을 토대로 후향적으로 분석 하였다. 급성요폐, 도뇨관삽관 중인 환자, 간헐적 도 뇨 중인 환자, 신경인성방광, 급성요로감염, 항생제 복용 중인 환자는 본 연구 대상에서 제외하였다. 균 배양채뇨는 요침사검사에서 5개 이상의 백혈구를 보인 환자에서 중간뇨를 채뇨하여 시행하였으며, 배 뇨 후 잔뇨량은 이동식 초음파 스캐너 (portable bladder
scanner)를 사용하여 측정하였다. 요배양검사에서 10
5개 이상의 균주가 동정된 경우를 요로감염이 있는 것 으로 정의하였고, 배양 결과와 측정된 배뇨 후 잔뇨 량과의 상관관계 및 세균뇨에 대한 배뇨 후 잔뇨량 의 절단치를 정할 수 있는지에 대해 조사하였다.
요배양검사 결과에 대한 나이, 잔뇨량, 최대요속, 전립선특이항원, 국제전립선증상점수의 차이를 알 아보기 위해 각각의 변수에 대하여 Student t-test를 이용하여 통계분석을 하였다. 그리고 배양 결과와 배뇨 후 잔뇨량의 상관관계 및 세균뇨에 대한 배뇨 후 잔뇨량의 절단치에 대한 통계학적 분석을 위해 다중로지스틱회귀분석 및 ROC 분석을 이용하였으 며, p 값이 0.05 미만이면 통계적으로 의미 있는 것 으로 간주하였다. 통계 프로그램은 SPSS 12.0 한글 버전을 사용하였다.
결 과
대상 환자들의 평균 나이는 63.3±10.4세였으며, 전 체 351명의 환자 중 31명 (8.83%)에서 요배양검사에 서 양성 소견을 보였다. 요배양검사 결과에 대한 각 변수의 차이를 알아보기 위한 Student t-test에서 연령, 배뇨 후 잔뇨량 및 국제전립선증상점수가 요배양검사 결과에 따른 유의한 차이를 보였다 (p<0.05)(Table 1).
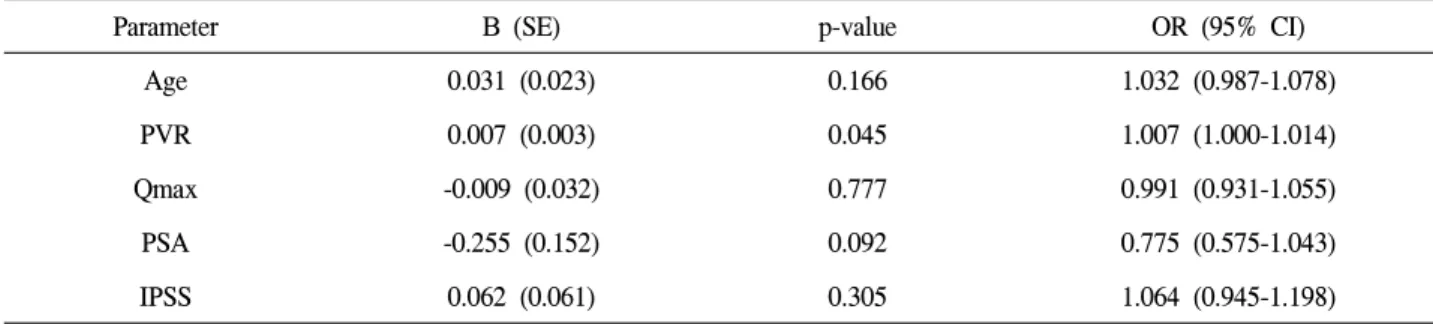
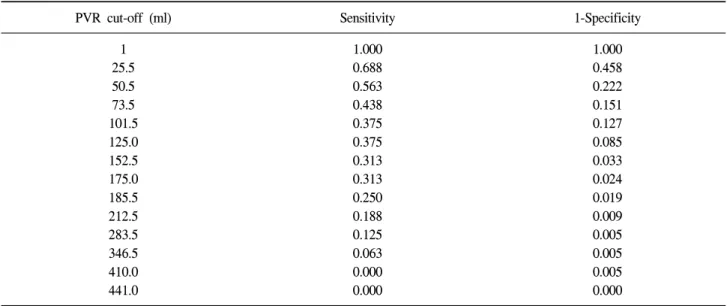
요로감염에 대한 예측인자를 알아보기 위한 다중로 지스틱회귀분석에서 연령과 국제전립선증상점수는 유의한 상관성이 없었고, 배뇨 후 잔뇨량만 유의한 상관성을 보였다 (p<0.05)(Table 2). 배뇨 후 잔뇨량 의 절단치를 알아보기 위한 ROC 분석에서 배뇨 후 잔뇨량 절단치가 175ml인 경우 민감도 31.3%, 특이 도 97.6%, 185ml인 경우 민감도 25%, 특이도 98.1%, 283.5ml인 경우 민감도 12.5%, 특이도 99.5%, 346.5ml 인 경우 민감도 6.3%, 특이도 99.5%로 나타났으며 (Table 3), ROC curve에서 유의한 절단치를 정할 수 는 없었다 (Fig. 1).
고 찰
요역동학적 관점에서 볼 때 잔뇨의 원인은 폐쇄
성 방광기능부전, 방광근비활성 및 두 가지 원인의
Table 1. Patient characteristics
Urine culture
Variable Overall Negative Positive p-value
No. patients Mean age Mean PVR Mean Qmax Mean PSA Mean IPSS
351 63.32±10.41 47.45±61.36 13.90±6.80
2.11±5.05 8.60±5.30
320 62.81±10.17 41.83±53.34 14.08±6.66
2.18±5.25 8.23±5.23
31 68.55±11.60 105.55±99.22
12.02±7.94 1.36±2.02 12.48±4.43
0.003 0.001 0.107 0.388
<0.001 PVR: post-void residual urine, Qmax: maximal uroflow rate,
PSA: prostate specific antigen, IPSS: international prostate symptome score
Table 2. Multiple logistic regression analysis of urinary tract infection predictors on the urine culture
Parameter B (SE) p-value OR (95% CI)
Age 0.031 (0.023) 0.166 1.032 (0.987-1.078)
PVR 0.007 (0.003) 0.045 1.007 (1.000-1.014)
Qmax -0.009 (0.032) 0.777 0.991 (0.931-1.055)
PSA -0.255 (0.152) 0.092 0.775 (0.575-1.043)
IPSS 0.062 (0.061) 0.305 1.064 (0.945-1.198)
PVR: post-void residual urine, Qmax: maximal uroflow rate,
PSA: prostate specific antigen, IPSS: international prostate symptome score, SE: standard error, OR: odd ratio, CI: confidence interval
상호작용에 기인한다. 이외에도 수분보충상태, 약물 투여, 배뇨행태 및 알콜 섭취 등의 원인으로 인해 방광 내 요배출이 방해되어 잔뇨가 남을 수 있다.
요로감염의 방어기전 중 가장 중요한 것 중의 하 나가 잔뇨 없이 배뇨하는 것이며, 이는 당뇨 및 신 경인성 환자의 경우에서 주로 적용되는 개념이다.
5,6다수의 비뇨기과 의사들은 배뇨 후 잔뇨를 전립선 비대증 수술에 대한 절대적 적응증으로 고려하고 있으나,
7배뇨 후 잔뇨를 보이는 상당수의 환자가 배뇨증상을 호소하지 않는 경우가 있고, 몇몇 연구 에서는 배뇨 후 잔뇨와 요로감염에 대한 상관관계 가 전혀 없다는 결과를 보고하기도 하였다.
8배뇨 후 잔뇨량은 연령, 전립선 용적, PSA, 배뇨증상점 수, 최대요속 및 요로감염에 영향을 받는다는 연구 결과가 있다.
9Kolman 등
10에 따르면, 성인 남성의 평균 잔뇨량은 141ml (평균 연령 54세)이었고, 전립
선의 크기와 상관관계가 있다고 하였으며, Barry 등
11은 하부요로증상이 있는 남성에서 배뇨증상, 연령, 최대요속이 배뇨 후 잔뇨량에 대해 상관관계를 보 인다고 하였다. Truzzi 등
3은 배뇨증상점수, 배뇨 후 잔뇨량이 요로감염에 대한 예측인자가 된다고 하였 으나, May 등
4은 요배양검사 결과에 따른 분석에서 배뇨 후 잔뇨량만이 요로감염에 대한 예측인자가 된다고 하였다. 본 연구에서는 연령과 배뇨 후 잔뇨 량이 요로감염에 대한 예측인자가 되는 것으로 나 타났다.
Truzzi 등
3과 May 등
4의 연구에서는 요배양검사에
서 양성을 보인 환자의 비율이 각각 27% 및 31%으
로 나타났는데, 이는 본 연구에서의 요배양검사 양
성률 8.83% 보다 높은 수치이다. 요배양검사 양성
률의 차이를 보이는 이유는 본 연구에서는 요침사
검사에서 백혈구 수치가 정상인 경우 추가적으로
Table 3. Sensitivity and specificity of PVR cut-off value by urinary tract infection results on the urine culture
PVR cut-off (ml) Sensitivity 1-Specificity
1 25.5 50.5 73.5 101.5 125.0 152.5 175.0 185.5 212.5 283.5 346.5 410.0 441.0
1.000 0.688 0.563 0.438 0.375 0.375 0.313 0.313 0.250 0.188 0.125 0.063 0.000 0.000
1.000 0.458 0.222 0.151 0.127 0.085 0.033 0.024 0.019 0.009 0.005 0.005 0.005 0.000 PVR: post-void residual urine
Fig. 1. post-void residual urine (PVR) as continuous variable correlated with positive urine culture.
A straight diagnoal line represents reference.
1-Specificity
1.0
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
요배양검사를 시행하지 않았기 때문에 요배양검사 에서 양성을 보인 경우가 낮게 나타났을 것으로 생 각한다. Truzzi 등
3이 보고한 180ml의 절단치는 본 연구에서는 적용되지 않았으며 May 등
4의 연구와 같은 결과를 보였다. Truzzi 등
3의 연구에서는 도뇨
관을 통하여 잔뇨량을 측정하였으나, May 등
4의 연
구 및 본 연구에서는 초음파 스캐너를 사용하여 측
정하였다. 김 등
12의 연구에서 초음파를 이용한 잔
뇨량 측정 시 민감도와 특이도가 높게 나타나 도뇨
법을 대체할 수 있는 방법이라고 하였고, 초음파를
이용한 잔뇨량 측정법은 유럽비뇨기과학회 가이드 라인에서 권장하고 있는 방법이기도 하다.
13본 연 구를 포함한 여러 연구에서 요로감염에 대한 잔뇨 량의 상관관계는 통계학적으로 의미가 있었으나 잔 뇨량의 절단치에 대한 결과가 다르게 나오는 것은 동일 환자에서 잔뇨량을 여러 번 측정하였을 때 각 각의 결과가 다를 수 있고, 도뇨법으로 측정된 잔뇨 량과 초음파 스캔으로 측정된 잔뇨량이 차이가 있 을 수 있으며, 균배양채뇨 방법에 따라 소변의 오염 도 차이가 생길 수 있는 등의 문제가 발생하기 때 문으로 생각한다.
본 연구의 한계점으로는 후향적 분석을 통한 연 구이기 때문에 연구하고자 했던 변수를 모두 적용 할 수는 없었다는 점, 잔뇨량 측정을 한 차례만 시 행한 점, 잔뇨량 측정시 도뇨법과 초음파 스캔의 차 이를 검토할 수 없었던 점, 단기간의 의무기록 검토 를 통한 단면적인 연구이기 때문에 추적관찰 결과를 알아볼 수 없는 점 등이며, 이는 향후 전향적 연구 를 시행하고자 할 때 참고해야 할 것으로 생각한다.
결 론
본 연구에서는 무증상의 성인 남성에서 의미 있 는 요로감염 발생율이 8.83%로 나타났고, 배뇨 후 잔뇨량만이 요로감염에 대한 의미있는 상관관계를 보였으나, 요로감염 예측을 위한 배뇨 후 잔뇨량의 절단치를 정할 수는 없었다. 따라서 기존의 300ml 혹은 180ml의 절단치를 임상적으로 적용하기에는 무리이고, 무증상 요로감염에 대한 진단 및 치료 적 응증은 배뇨 후 잔뇨량만으로 정할 수는 없으며, 여 러 가지 인자를 종합하여 적용하여야 할 것으로 생 각한다.
REFERENCES
1. Kaplan SA, Wein AJ, Staskin DR, Roehrborn CG, Steers WD. Urinary retention and post-void residual urine in men: separating truth from tradition. J Urol
2008;180:47-54
2. Abrams PH, Dunn M, George N. Urodynamic findings in chronic retention of urine and their relevance to re- sults of surgery. Br Med J 1978;2:1258-60
3. Truzzi JC, Almeida FM, Nunes EC, Sadi MV. Residual urinary volume and urinary tract infection-when are they linked? J Urol 2008;180:182-5
4. May M, Brookman-Amissah S, Hoschke B, Gilfrich C, Braun KP, Kendel F. Post-void residual urine as a predictor of urinary tract infection-is there a cutoff value in asymptomatic men? J Urol 2009;181:2540-4 5. Twaij M. Urinary tract infection in children: a review
of its pathogenesis and risk factors. J R Soc Health 2000;120:220-6
6. Kitami K. Vesicourethral dysfunction of diabetic patients. J Urol 1991;82:1074-83
7. Hansen MV, Wold T. A survey concerning the atti- tudes of urologists toward prostatism patients. Scand J Urol Nephrol 1994;28:257-64
8. Hampson SJ, Noble JG, Rickards D, Milrov EJ. Does residual urine predispose to urinary tract infection? Br J Urol 1992;70:506-8
9. Thomas AW, Cannon A, Bartlett E, Ellis-Jones J, Abrams P. The natural history of lower urinary tract dysfunction in men: minimum 10-year urodynamic fol- low-up of untreated bladder outlet obstruction. BJU Int 2005;96:1301-6
10. Kolman C, Girman CJ, Jocobsen SJ and Lieber MM.
Distribution of post-void residual urine volume in ran- domly selected men. J Urol 1999;161:122-7
11. Barry MJ, Cockett ATK, Holtgrewe HL, McConnell JD, Sihelnik SA, Winfield HN. Relationship of symp- toms of prostatism to commonly used physiological and anatomical measures of the severity of benign pro- static hyperplasia. J Urol 1993;150:351-8
12. Kim JH, Kim JH, Choi YD. The accuracy of portable ultrasound scanning in the measurement of residual urine volume. Korean J Urol 2002;43:933-7
13. Madersbacher S, Alivizatos G, Nordling J, Sanz CR, Emberton M, de la Rosette JJ. EAU 2004 guidelines on assessment, therapy and follow-up of men with lower urinary tract symptoms suggestive of benign prostatic obstruction (BPH guidelines). Eur Urol 2004;46:547-54