투고일: 2012년 6월 15일, 심사일: 2012년 6월 30일, 게재확정일: 2012년 6월 30일 책임저자:류주석, 성남시 분당구 야탑동 351
(463-712) 차의과학대학교 분당차병원 재활의학과 Tel: 031) 780-6285, Fax: 031) 780-6206 E-mail: jseok337@cha.ac.kr
Copyrights ⓒ The Korean Dysphagia Society, 2012.
상부 식도 괄약근 수축의 생리
류주석
차의과학대학교 분당차병원 재활의학과
Physiology of Upper Esophageal Sphincter Contraction
Ju Seok Ryu, M.D., Ph.D.
Department of Rehabilitation Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea
Upper esophageal sphincter is defined as the intra-luminal high-pressure zone separating the pharynx from the esophagus. This region is consisted of inferior pharyngeal constrictor, cricopharyngeus muscle and cranial cervical esophagus. The primary function of upper esophageal sphincter is to transmit bolus from pharynx to esophagus.
Cricopharyngeus muscle is the most important muscle in upper esophageal sphincter. This muscle responds differ- ently in diverse circumferences. It is necessary to know normal anatomy and physiology of upper esophageal sphinc- ter to understand normal function of upper esophageal sphincter. In addition, to know normal function is pre- requisite to know abnormal findings of this region. So I will review the normal anatomy and physiology of upper esophageal sphincter. I think this topic is important for doctors and therapists who want to investigate and practice dysphagia. (JKDS 2012;2:35-42)
Keywords: Dysphagia, Upper esophageal sphincter, Anatomy, Physiology
서론
연하장애란 음식물을 섭취하여 구강기, 인두기 및 식도 기 전 과정에서 발생할 수 있는 모든 이상을 총칭한다.
연하장애는 음식을 먹을 때 식사 시간의 지연, 불편감, 기 침과 같은 가벼운 문제에서부터 영양장애, 탈수, 흡인성 폐렴과 같은 심각한 문제를 일으킬 수 있으며, 심지어 사 망에 이를 수도 있어서 매우 주의를 요한다1.
연하에는 구강, 인두, 식도가 관여하게 되며, 이 구조물 은 괄약근에 의해 세 개의 방으로 나뉘어 연속적으로 팽 창 및 수축하게 된다. 식괴의 이동은 식괴의 후방에 작용
하는 양압과 전방에서 형성된 음압에 의해 이루어진다1. 연하는 전통적으로 구강전기(oral preparatory phase), 구강기(oral phase), 인두기(pharyngeal phase), 식도기 (esophageal phase)의 네 단계로 이루어진다2. 이 일련 의 과정은 구강, 인두, 후두, 식도에 존재하는 25쌍의 근 육에 의해 연속적으로 조화된 수축과 이완을 통해 달성된 다. 특히 식괴의 앞 부분이 전구협궁(anterior faucial arch) 또는 코 가시(nasal spine)를 통과한 후 식괴의 후 방이 상부식도 괄약근을 통과할 때까지를 인두기로 부르 며, 연하에서 특히 중요한 단계이다. 본 종설은 인두기와 식도기를 구분하는 상부 식도 괄약근에 초점을 맞추어 정
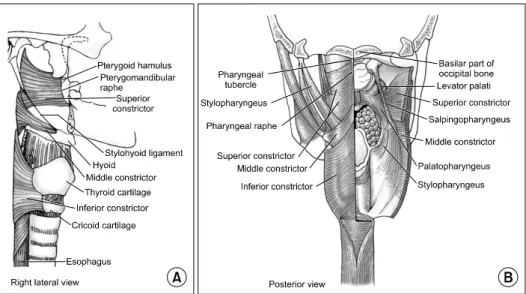
Fig. 1. These figures show normal anatomy of normal upper esoph- ageal sphincter.
상 해부 및 생리에 대해 알아보도록 하겠다.
본론
1. 상부식도 괄약근의 정의
상부 식도 괄약근은 인두-식도 부분(pharyngo-esoph- ageal segment)을 말하고, 인두와 식도를 구분하는 내강 내 고 압력 부위(intraluminal high-pressure zone)를 의미한다.
여기에는 하인두수축근(inferior pharyngeal constrictor), 윤 상인두근(cricopharyngeus), 두 개경부식도(cranial cervic- al esophagus) 등으로 이루어진다3.(Fig. 1)
이 중 윤상인두근이 특히 중요한 역할을 담당한다. 윤 상인두근은 1717년 Valsalva에 의해 처음으로 기술되었 으나4, 20세기에 들어서야 그 존재가 명확해지기 시작했 다. 문헌에 따라서는 하인두수축근을 윤상인두근에 포함 시키기도 한다. 그래서 하인두수축근을 윤상인두근의 상 부 기울어진 부위(pars oblique), 윤상인두근을 하부 수 평 부위(pars fundiformis)로 부르기도 하나, 대체로는 하인두수축근과 윤상인두근으로 나누는 것이 일반적이다.
고 압력 부위(high pressure zone)는 후두(laryngeal opening)에서 연결되며, 약 2-4 cm 사이에 위치하며, 윤 상인두근은 고 압력 부위의 아래쪽 1/3을 차지한다3. 각각의 근육의 역할은 생리적인 상태에 따라 다르게 나 타난다. 인두와 식도 사이의 울타리로 작용하여 연하 중 식도로부터의 역류를 막기도 하지만, 구역질이나 구토 중 에는 식도 내의 물질이 인두, 구강으로 통하도록 허용하 기도 한다.
2. 정상 상부 식도 괄약근의 해부
하인두수축근은 후정중솔기(posterior median raphe) 에서 기시하여 감상연골의 앞 부위에(anterior thyroid cartilage)에 부착한다. 윤상인두근은 하인두수축근의 하 방에서 연속적으로 기시하여 주행하며, 윤상연골(cricoid cartilage)의 후방 옆면에 부착한다. 특히 정중솔기에는 부착하지 않고, C 모양의 근육 띠를 형성한다. 그러므로 고 압력 부위는 단순히 근육으로 이루어진 띠라기보다는 근육, 연골, 건막(aponeurosis) 등으로 이루어진 복합체 를 말한다3,5.(Fig. 1)
윤상인두근은 직경이 25-35 μm로 매우 작은 가로무늬근 (striated muscle)으로 구성되고, 상하 길이는 0.7 cm, 너비 는 1-2 cm이다6. 섬유형은 주로 고산화(highly oxidative), 느린 연축(slow twitch), 제1형 섬유형(type I fiber)으로 이루어져 있으며, 제2형 섬유(빠른 연축근)는 상대적으로 적다6. 제1형 섬유가 상대적으로 많은 조직학적 특징으로 인해 기저 긴장성을 유지할 수 있다. 제2형 섬유는 삼킴 이나, 트림, 구토 시 빠른 수축에 관여하게 된다. 그 외에 교원 조직이 상당한 부분을 차지하여(약 40%) 탄력성에 기여하게 된다. 즉 식괴가 상부식도 괄약근을 통과할 때 능동적 이완 없이 확장되며, 식괴가 통과한 뒤 빠르게, 신 경의 자극 없이 원래 위치로 되돌아간다.
후두의 신경지배는 대부분 10번 뇌신경에 의하며, 위후 두신경(superior laryngeal nerve)에서 분지한 내후두신 경(internal laryngeal nerve)이 성대주름(vocal folds) 위 후두 점막의 감각을 담당하고, 되돌이후두신경(recurrent laryngeal nerve)이 윤상갑상근(cricothyroid muscle)을
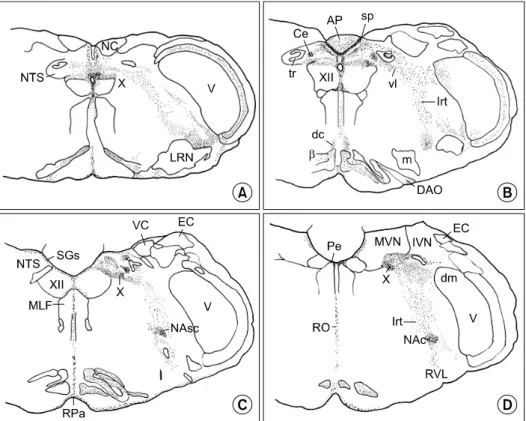
Fig. 2. These figures show medulla oblongata, caudal (A), (B) and rostral (C), (D). NTS: Nucleus tractus solitarii, β: subnucleus beta of medial accessory olive, Ce: nucleus centralis of NTS, DAO: dorsal accessory olive, dc: dorsal cap of Kooy, dm: dorsal medial protuberance of V, EC: ex- ternal cuneate nucleus, IVN: inferior vestibular nucleus, m: medial division of lateral reticular nucleus (LRN), MLF: medial longitudinal fasciculus, MVN: medial vestibular nucleus, NAc: nucleus ambiguus, compact division, NAsc: nucleus ambiguus, semicompact division, NC: nucleus cuneatus, RO: nucleus raphe obscurus, RPa: nucleus raphe pallidus, RVL: rostral ventrolateral reticular nucleus, SGs: stratum gliosum subependymale, sp:
subpostremal subnucleus of NTS, tr: tractus solitarius, VC: vestibular complex (caudal pole), vl: ventrolateral subnucleus, XII: hypoglossal nucleus.
제외한 후두의 모든 내재근(intrinsic muscle)을 지배한 다. 인두는 주로 IX, X번 뇌신경과 위목신경얼기(superior cervical plexus)의 지배를 받는다. 인두신경얼기(pharyngeal plexus)의 미주신경 분지(vagal branch)는 모든 인두 근 육을 지배하나 예외적으로 경돌인두근(stylopharyngeus muscle)은 IX 뇌신경에 의해, 구개범장근(tensor veli pa- latini muscle)은 V2 신경의 지배를 받는다7.
윤상인두근의 신경지배를 조금 더 자세히 살펴보면, 윤 상인두근의 아래와 앞 부분은 되돌이후두신경에 의해, 위 와 뒤쪽 부분은 인두신경얼기의 지배를 받는다. 되돌이후 두신경을 자극하면 윤상인두근에서 빠르고, 큰 진폭의 운 동단위 활동전위를 얻을 수 있으며, 근위부 식도를 빨리 닫고, 인두를 빨리 거상시키게 된다. 반면 인두신경얼기 를 자극하면 느린 속도, 저 진폭의 운동단위 활동전위가 나타나게 된다. 윤상인두근의 감각은 혀인두신경(glosso- pharyngeal nerve)과 위후두신경(superior laryngeal nerve)이 담당하고, 동물 실험에서는 교감운동신경이 운
동조절에 관여한다는 보고가 있으나 사람에서는 관여하지 않는다는 문헌도 있어서 논쟁이 있다8,9.
3. 인두기의 신경 조절(neuronal control of pha- ryngeal phase of swallowing)
뇌간의 망상체(reticular formation) 내의 신경들을 통 합해서 central pattern generator (CPG)라고 부른다. 이 는 이 부위가 흥분 및 억제 신호를 담당하는 운동 신경을 자극하여, 일련의 복잡하지만 반복적인 운동을 유발하기 때 문이다. CPG는 구심성 신경 체계(afferent input system), 원심성 신경 체계(efferent system), 조절 체계(organi- zing system)의 세 부분으로 나눌 수 있다. 구심성 신경 체계는 말초 감각 신경을 수용하고, 원심성 신경 체계는 인두의 근육으로의 운동 출력(motor output)을 담당하 며, 조절 체계는 운동 양상을 계획하는 뇌간 내의 신경 내 네트워크를 조절하는 기능을 한다. 구체적으로 살펴보 면, 식괴가 인두로 넘어가면서 인두의 감각 수용체가 자
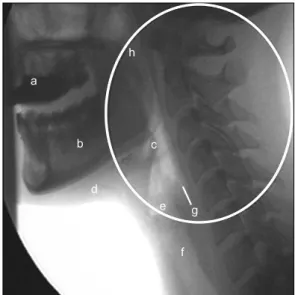
Fig. 3. This figure shows normal lateral image from a VFSS. The components of normal structure are as followings. a. barium in the oral cavity, b. Mandible, c. Epiglottis, d. Suprahyoid muscles, e. Vocal cords, f. Trachea, g. High-pressure zone of the UES.
Adapted from Singh S and Hamdy S. Neurogastroenterology &
Motility, 2005.
극되면 위후두신경으로 신호가 전달되어, CPG의 조절을 받아 비수의적인 삼킴 반사가 나타나게 된다10,11. 구심성 신경 체계는 삼차신경(V), 혀인두신경(IX), 미 주신경(X)에서 담당하여 말초의 감각 피드백을 CPG에 제공한다. 특히 인두신경얼기를 통한 혀인두신경과 미주 신경에서 나온 위후두신경이 가장 민감한 부위이다. 감각 신경은 뇌간의 고립로핵(nucleus tractus solitaries)에 도 달하며, 이 부위가 인두, 식도의 주요 감각 핵(nucleus)이 다11,12.
원심성 운동 출력에 관여하는 뇌간의 주요 핵으로는 혀밑 신경 운동 핵(hypoglossal motor nucleus), 의핵(nucleus ambiguous)이 담당하며, 식도 운동신경은 rostal com- pact formation of the nucleus가, 인두와 연구개의 운동 신경은 intermediate semicompact formation이, 후두 운동신경은 caudal loose formation of the nucleus 등 이 관여한다12.
뇌간의 사이신경(brainstem interneuron)은 주로 협동 (coordination)에 관여하며, 등쪽 연하군(dorsal swallow- ing group)과 배쪽 연하군(ventral swallowing group)으 로 나뉜다. 등쪽 연하군은 주로 연하를 시작하는 데 관여하 고, 배쪽 연하군은 조절, 협응에 관여한다13.(Fig. 2) 식괴 없이도 삼키면 연하반사가 일어나는 것으로 보아 대뇌 피질에서의 자극이 연하를 유발할 수 있음을 시사한다. 뇌의 일차운동피질(primary motor cortex), 전운동피질(premotor cortex), 피질하 부위(피질원심통로(corticofugal pathway), 속섬유막(internal capsule), 시상밑부(subthalamus), 편도핵 (amygdale), 시상하부(hypothalamus), 흑색질(substantia nigra), mesencephalic reticular formation, 모노아민 뇌관 통로(monoaminergic brain stem pathway), 아래뇌섬엽 (inferior insula), 담장(claustrum), 소뇌(cerebellum) 등 이 관여하는 것으로 알려져 있으나 정확한 해부생리학적 기존은 모르는 상태이다.
경두개자기자극을 이용한 연구에서는 하부 중심앞이랑 과 후아래전두이랑(lower precentral, posterior inferior frontal gyri)의 자극으로 구강기 근육의 수축을 유도하였 고, 앞아래전두이랑(anterior inferior, middle frontal gyri)의 자극으로 인두 및 식도 가로무늬근의 자극을 유 도하였다. 또한 피질 자극(cortical stimulation)과 후두하 의 미주신경을 자극함으로써 윤상인두근의 수축도 유도할 수 있다14.
4. 정상 상부식도 괄약근의 생리
비디오 투시조영 검사를 통해 연하에 관여하는 중요한
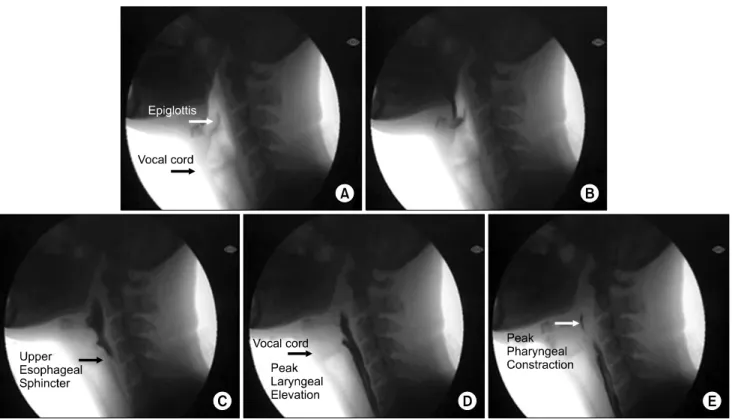
해부학적 위치를 아는 것이 필요하다.(Fig. 3) 운동형상학 적 분석을 통하여 인두기의 주요 연하 과정은 1/30 초 단 위로 분석이 가능하며, 이를 통해 후두개(epiglottis), 성대 주름의 거상, 인두의 수축, 상부 식도 괄약근의 이완 등과 같은 요소들의 정확한 시간 순서를 알 수 있고, 상부 식 도 괄약근이 다른 연하 관련 요소의 움직임과의 시간적 관련성을 이해할 수 있다15,16.(Fig. 4)
후두개는 선 자세에서 후두가 열리면서 수평 자세로, 이어서 아래로 굽은 자세가 된다. 이 동작은 설골, 후두의 거상, 갑상설골근(thyrohyoid muscle)과 성대주름(vocal folds)에 인접한 후두의 내재근의 수축에 의해 유도된다.
이 시기에 성대주름의 외전근과 후윤상피열근(posterior cricoarytenoid muscle)은 억제된다.
후두는 해부학적으로 아래에서 위 방향으로 닫힌다. 즉 성대주름이 가장 먼저 닫히고, 전정주름(vestibular folds), 하부 안뜰(lower vestibule), 상부 안뜰(upper vestibule) 의 순서로 닫히며, 열릴 때는 위에서 아래 방향으로 열리 게 된다7.
근전도를 이용한 연구를 보면, 악설골근(mylohyoid muscle)에서 먼저 수축이 일어나고, 이와 동시에 또는 아 주 조금 뒤 전이복근(anterior digastric muscle, V), 악 돌근(pterygoid muscle, V)의 수축이 일어난다. 이후 이 설골근(geniohyoid, XII), 경상설골근(stylohyoid, VII),
Fig. 4. Swallowing processes of a normal person. (A) Initiation of pharyngeal phase. (B) Latency of epiglottis contact. (C) Latency of UES opening. (D) Latency of peak laryngeal elevation. (E) Latency of peak pharyngeal constriction. Adapted from Choi KH, et al. Dysphagia, 2011.
Table 1. Changes in upper esophageal sphincter pressure either observed or experimentally characterized. Adapted from Singh S and Hamdy S. Neurogastroenterology & Motility, 2005.
UES pressure Dncreased
Increased
Swallowing Belching Vomiting Expiration Sleep Infancy Elderly Inspiration Stress
Esophageal distension Intra-esophageal acid
Secondary peristalsis originating in the esophagus Pharyngeal stimulation with air or water 경상설근(styloglossus, XII), 후방 혀(posterior tongue),
상인두수축근(superior constrictors, X), 구개설근(palato- glossus, X), 구개인두근(palatopharyngeus muscle, X) 등 이 수축한다. 이러한 근육군을 선도 복합체(leading com- plex)라 부른다. 이후 중, 하인두수축근(middle, inferior constrictor, X)가 순차적으로 겹치면서 수축하고, 상부 식도 괄약근에 근수축의 물결이 도달하면 일련의 과정이 끝나게 된다17.
상부 식도 괄약근은 휴식 시 윤상인두근의 긴장수축 (tonic contraction)에 의해 닫혀있고, 열릴 때는 긴장수 축이 억제된다. 이 시기는 인두기가 시작할 때 같이 시작 하여 식괴가 식도를 통과한 뒤 윤상인두근이 다시 수축할 때까지 지속된다. 정상적인 상부 식도 괄약근의 이완에는 후두의 거상과 윤상인두근의 이완이 가장 중요한 요소이다.
상부 식도 괄약근의 성공적인 통과를 위해서는 식괴의 뒤에 작용하는 강력한 혀의 압력과 인두-식도 부위에서 발생한 음압과 인두수축근의 연동운동(가장 덜 중요함)이 필요하다18,19.
고 압력 부위에 식괴가 통과하면 이 부위의 압력이 급 격히 올라간 뒤 천천히 내려오는 비대칭적인 양상을 보인
다. 측면에 비해 전후면에서 3배의 압력이 가해지며, 휴 식기 압력은 35-200 mmHg이다. 수면 시에는 압력이 완 전히 소실되고, 영아나 노인에서는 상대적으로 압력이 낮 다. 삼킬 때는 식괴가 통과한 뒤 인두 수축근의 연동운동
Fig. 7. Two stages of the CP-EMG pause (absolute and rela- tive) are shown with conventional and integrated/averaged CP-EMG traces. There was almost complete bioelectrical si- lence during the first part of the pause (absolute period), but in the later part of the pause (relative period), small motor unit potentials are seen. Adapted from Ertekin C and Aydogdu I. Muscle and Nerve, 2002.
Fig. 6. Time line showing the relationship of events during a normal swallow. The exact timing are influenced by factors such as age and bolus size. Adapted from Singh S and Hamdy S. Neurogastroenterology & Motility, 2005.
Table 2. Incidence of CP-EMG properties encountered in 39 nomral subjects during swallowing. Adapted from Ertekin C and Aydogdu I. Muscle and Nerve, 2002.
Properties No. of cases (%)
CP-EMG pause Rebound burst Foreburst
Two stages of CP-EMG pause Forepause
39 (100) 39 (100) 27 (69) 14 (36) 7 (18) CP-EMG: cricopharyngeal muscle electromyography.
Fig. 5. This figure shows EMG activities of the suprahyoid muscle (SM-EMG) and cricopharyngeal muscle (CP-EMG) while 3 cc water are swallowed. During rest, there was con- tinuously high-frequency tonic EMG activity in the CP muscle (third trace). During swallowing, SM-EMG activity began first and the tonic EMG activity of CP muscle was switched off (pause) (first and second traces). Adapted from Ertekin C and Aydogdu I. Muscle and Nerve, 2002.
이 지속되며, 이 기전으로 인해 내강 내 물질의 역류를 막는데 도움이 된다. 트림을 하면 윤상인두근의 압력이 매우 감소하고, 삼킬 때에 비해 상부 식도 괄약근의 이완 기간은 4배 가량 더 길어진다. 구역질, 구토 시에 하인두 수축근과 윤상인두근이 함께 압력이 감소하고, 기침이나 재채기에서는 함께 압력이 증가한다3.(Table 1)
삼킴 동안에 상부 식도 괄약근 압력 감소는 영상에서 보이는 것보다 선행한다. 이 이유는 윤상인두근과 하인두
수축근 수축의 억제와 설골상근(suprahyoid muscle)의 수축 등이 관여하기 때문이다.
5. 상부 식도 괄약근의 전기생리학적 특징
윤상인두근와 설골상근에 침 전극을 붙인 뒤 삼킴 반사 를 유도해보면, 설골상근이 먼저 수축한 뒤 윤상인두근 수축이 억제되는 것을 볼 수 있다5.(Fig. 5) 또 윤상인 두근과 상부 식도 괄약근의 압력, 후두의 거상 및 하강, 후두 안뜰의 닫힘, 식괴의 이동을 같은 그림에 시간의 순서대로 나열하면 Fig. 6의 일련의 과정을 확인할 수 있다3.(Fig. 6)
삼킴 동안 윤상인두근의 이완(CP-EMG pause)을 살펴 보면 CP-EMG pause에서 절대적과 상대적 이완(absolute, relative pause)이 있음을 확인할 수 있다. 절대 이완은 전기적으로 완전히 조용한 상태이며, 초기 100-200 ms 이며, CP-EMG pause의 약 40%에 해당하며, 상대 이완 은 작은 운동단위 전위가 보이고, CP-EMG pause의 약 50% 이상을 차지한다5.(Fig. 7)
CP-EMG pause가 나타나기 전에 전돌발파(foreburst activity)가 관찰되고, CP-EMG pause 후 반동돌발파 (rebound burst activity)가 나타난다. 전돌발파는 정상인 의 약 69%에서 발견되고, 삼킴에는 반드시 필요하지 않 는 일종의 보호적 반사(protective reflex)로 여겨진다5. 반면 반동돌발파는 정상인의 100%에서 나타나고, central pattern generator의 연속적 근육 수축에 명확히 구분되 는 전기적 현상(electrical event)이다3,5.(Table 2) 결론
삼킴 중 상부 식도 괄약근을 통과할 때는 먼저 긴장성 운동신경의 억제가 일어나고, 둘째, 윤상인두근의 이완이 나타나게 되며, 셋째, 반동돌발파 동안에는 위상성이며, 더 큰 운동신경이 자극되어서 식괴가 통과한 뒤 가능한 빨리 괄약근을 닫게 된다. 이후 넷째로 긴장성 운동신경 이 다시 흥분되며 삼킴의 과정이 끝나게 된다.
상부 식도 괄약근의 기능을 이해하기 위해서는 정상 해 부 및 생리를 이해하는 것이 필요하다. 최근 근전도 및 경두개자기자극술 등의 방법으로 상부 식도 괄약근의 기 능에 대한 이해가 깊어졌다. 정상 상부 식도 괄약근을 이 해하는 것은 이상을 판단하는 기초가 되므로, 연하장애를 연구하고, 임상에 적용하는 하는 의사 및 치료사에게 매 우 중요할 것으로 생각한다.
REFERENCES
1. Leonard R, Kendall K. Dysphagia assessment and treat- ment planning: a team approach. 2nd ed. San Diego:
Plural Publishing, 2008.
2. Dodds WJ, Stewart ET, Logemann JA. Physiology and ra- diology of the normal oral and pharyngeal phases of swallowing. AJR Am J Roentgenol. 1990;154:953-63.
3. Singh S, Hamdy S. The upper oesophageal sphincter.
Neurogastroenterol Motil. 2005;17 Suppl 1:3-12.
4. Calcaterra T, Kadell BM, Ward PH. Dysphagia secondary to cricopharyngeal muscle dysfunction, Surgical Management.
Arch Otolaryngol. 1975;101:726-9.
5. Ertekin C, Aydogdu I. Electromyography of human cri- copharyngeal muscle of the upper esophageal sphincter.
Muscle Nerve. 2002;26:729-39.
6. Bonington A, Mahon M, Whitmore I. A histological and histochemical study of the cricopharyngeus muscle in man. J Anat. 1988;156:27-37.
7. Leonard R, Kendall K. Dysphagia assessment and treat- ment planning. 2nd ed. San Diego: Plural Publishing, Inc., 2008.
8. Brok HA, Copper MP, Stroeve RJ, Ongerboer de Visser BW, Venker-van Haagen AJ, Schouwenburg PF. Evidence for re- current laryngeal nerve contribution in motor innervation of the human cricopharyngeal muscle. Laryngoscope. 1999;
109:705-8.
9. Medda BK, Lang IM, Layman R, Hogan WJ, Dodds WJ, Shaker R. Characterization and quantification of a phar- yngo-UES contractile reflex in cats. Am J Physiol. 1994;
267:G972-83.
10. Jean A. Brain stem control of swallowing: neuronal net- work and cellular mechanisms. Physiol Rev. 2001;81:
929-69.
11. Altschuler SM. Laryngeal and respiratory protective reflexes. Am J Med. 2001;111 Suppl 8A:90S-4S.
12. Broussard DL, Altschuler SM. Central integration of swal- low and airway-protective reflexes. Am J Med. 2000;108 Suppl 4a:62S-7S.
13. Amirali A, Tsai G, Schrader N, Weisz D, Sanders I.
Mapping of brain stem neuronal circuitry active during swallowing. Ann Otol Rhinol Laryngol. 2001;110:502-13.
14. Ertekin C, Turman B, Tarlaci S, Celik M, Aydogdu I, Secil Y, et al. Cricopharyngeal sphincter muscle responses to transcranial magnetic stimulation in normal subjects and in patients with dysphagia. Clin Neurophysiol. 2001;
112:86-94.
15. Choi KH, Ryu JS, Kim MY, Kang JY, Yoo SD. Kinematic analysis of dysphagia: significant parameters of aspiration related to bolus viscosity. Dysphagia. 2011;26:392-8.
16. Kang JY, Choi KH, Yun GJ, Kim MY, Ryu JS. Does Removal of Tracheostomy Affect Dysphagia? A Kinematic Analysis. Dysphagia. 2012 Feb 12 [Epub].
17. Moore K, Dalley A. Clinically oriented anatomy. 5th ed.
Baltimore: Illiams and Wilkins, 2006.
18. McConnel FM. Analysis of pressure generation and bolus transit during pharyngeal swallowing. Laryngoscope. 1988;
98:71-8.
19. McConnel FM, Cerenko D, Jackson RT, Guffin TN Jr.
Timing of major events of pharyngeal swallowing. Arch Otolaryngol Head Neck Surg. 1988;114:1413-18.