It is very important to detect failing hemodialysis arte- riovenous fistula as early as possible because the early treatment of stenoses by percutaneous intervention has been shown to increase the longevity of the dialysis shunts (1, 2). In current clinical practice, detection and grading of the stenosis are usually performed using color doppler sonography and digital subtraction angiography (DSA) (3, 4). Color doppler sonography is obviously the first choice of diagnostic method and it can non-inva- sively demonstrate failing hemodialysis arteriovenous
Contrast-Enhanced MR Angiography of Failing Hemodialysis Arteriovenous Fistulas and Grafts: A Preliminary Experience1
Young-Sun Lee, M.D., Gong-Yong Jin, M.D., Young-Min Han, M.D., Sang-Yong Lee, M.D., Hak-Hun Park, M.D., Sung Kwang Park, M.D.2
Purpose:The purpose of this report is to evaluate the vascular stenosis for failing he- modialysis arteriovenous fistulas and grafts using contrast-enhanced MR imaging (CE- MRI) and to compare the results with digital subtraction angiography (DSA).
Materials and Methods:Nine patients (27 segmental vessels) with symptoms and signs of AVF stenosis or occlusion who presented to our medical department were recruited into this prospective comparative study. All of the patients with Brescia-Cimino arteri- ovenous fistula (AVF) or synthetic polytetrafluoroethylene (PTFE, GoretexⓇ) loop graft underwent MRA and DSA of the fistula. MRA was performed with a 1.5-T system us- ing VIBE sequence: TR/TE=3.5/1.5 msec, flip angle 20-25°, matrix 115×256, FOV 350×350, interpolated slice thickness 2.0 mm, fat suppression, scan time 13-18 sec and total time of 5 min. DSA was used as the reference standard for assessing the accu- racy of MRA, and MRA was analyzed for the presence of stenosis or occlusion, a grad- ing of stenosis, and the presence of collateral vessels. Two radiologists prospectively analyzed the MRAs by working in consensus.
Results:Regarding the stenotic grade, CE-MRA corresponded with the DSA in six pa- tients (66.7%) and it overestimated the stenoses in three patients (33.3%). For the stenotic site, MRA had a sensitivity of 86.4%, a specificity of 40%, a positive predictive value of 32.1%, and a negative predictive value of 66.7%.
Conclusion: Multiphase CE-MRA of the AVF noninvasively provided information comparable to that provided by DSA for the vascular stenosis regarding failing he- modialysis arteriovenous fistula.
Index words :Fistula, arteriovenous
Magnetic resonance (MR), three-dimensional Magnetic resonance (MR), vascular studies Digital subtraction angiography
1Department of Diagnostic Radiology, Chonbuk National University Medical School
2Department of Internal Medicine, Chonbuk National University Medical School
Received April 24, 2004 ; Accepted October 27, 2004
Address reprint requests to : Gong-Yong Jin, M.D., Department of Diagnostic Radiology, Chonbuk National University Hospital, 634-18 Keumam-dong, Chon-ju, Chonbuk 561-712, South Korea.
Tel. 82-63-250-2307 Fax. 82-63-272-0481 E-mail: [email protected]
fistulas, including stenosis, thrombosis, arterial steal and aneurysmal formation. However, color doppler also has some limitations: it is dependent upon the skill of the ex- aminer, and it is difficult to distinguish between the very slow moving blood flow due to a severe stenosis and that of the occlusion; it is also difficult to detect col- lateral vessels around the prestenotic area (5, 6).
Although DSA and color doppler sonography have been the preferred methods for observing failing he- modialysis arteriovenous fistula, magnetic resonance angiography (MRA) may also be an attractive non-inva- sive method for evaluating dysfunctional hemodialysis access. Varying results have been published concerning the ability of MRA to detect the stenoses in AVF by us- ing time-of-flight (TOF) (7), phase contrast (PC), and con- trast-enhanced MRA (CE-MRA) (8, 9) techniques. A ma- jor problem with the flow-based approaches to MRA, such as TOF and PC, has been the frequent occurrence of flow artifacts in regions with disturbed blood flow, and these artifacts can complicate interpretation of the MRA (7). Compared with TOF and PC, CE-MRA is less sensitive to these artifacts and has provided better re- sults (10, 11). However, there has been only limited in- formation reported on its use in the literature.
The purpose of this study was to evaluate the feasibili- ty of using CE-MRA for failing hemodialysis arteriove-
nous fistulas and grafts.
Materials and Methods
Patients
Nine patients who presented to our medical depart- ment with symptoms and signs of AVF stenosis or oc- clusion were recruited for this prospective comparative study. If the absolute AVF flow at any time was <600 ml/minute or if a patient exhibited a flow decline of
>25% between two consecutive measurements in com- bination with an absolute flow of <1000 ml/minute, then the fistula was considered at risk for thrombosis (11). All of the patients (4 men and 5 women, aged 32- 72 years; mean age: 53.1 years) had a Brescia-Cimino ar- teriovenous fistula (AVF) (n=5) (Fig. 1) or synthetic polytetrafluoroethylene (PTFE, Goretex(r)) loop graft (n=4) (Fig. 2), and they all underwent MRA of the fistu- la, and within four days, digital subtraction angiography (DSA).
Digital subtraction angiography (DSA)
All the DSA examinations were performed by one ex- perienced angiographer (YMH) with the use of an an- giostar (Simens, Muchen, German). Vascular access was examined by using high-frequency (7.0-MHz) color ul-
A B
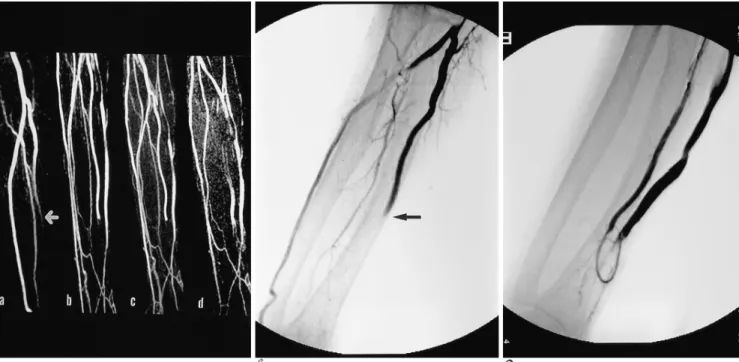
Fig. 1. MIP of a multiphase CE-MRA and DSA of a radiocephalic AVF ob- tained from the left arm of a 33-year- old male patient.
A. On the CE-MRA, multiple severe stenoses are viable in the cephalic vein.
B. CE-MRA of the severe venous steno- sis is shown with the corresponding DSA. The patient did not undergo per- cutaneous angioplasty due to the multi- ple, long stenoses.
trasonography (US) (ATL, WA, U.S.A.) and the puncture site was chosen to be as far away as possible from the anastomosis. To access the collapsed fistula, a sterile la- tex tourniquet was placed tightly on the upper arm or shoulder region. The fistula was punctured with an 18- gauge cannula sheath, and this was generally done un- der US guidance. A 0.035-inch hydrophilic guide wire and a 7F vascular sheath (Cook, Bloomington, IN, U.S.A.) were introduced in a retrograde fashion.
Angiography was performed by means of a hand injec- tion of 5-10 ml of dilute iohexol (Visipaque 320, Nycomed Amersham, Cork, IRELAND) through the vascular sheath. Based on the CE-MRA and DSA, seven patients underwent percutaneous angioplasty (PTA) and two patients underwent surgical treatment.
Contrast-enhanced MR angiography using a volumetric interpolated breath-hold examination (VIBE)
MRA was performed with a 1.5-T system (Symphony;
Siemens, Enlargen, Germany) by using a torso phase ar- ray coil or surface coil. The coil was placed over the pa- tients so as to extend from the shoulder to the hand. We used a coronal contrast enhanced three-dimensional (3D) VIBE sequence: TR/TE=3.5/1.5 msec, flip angle 20-25°, matrix 115×256, FOV 350×350, interpolated slice thickness 2.0 mm, fat suppression, scan time 13- 18 sec and total time of 5 min. An intravenous catheter was placed in the contralateral antecubital or forearm vein prior to the start of the study, and it was attached to an MR-compatible power injector (SpectrisⓇ; Medrad, Pittsburgh, U.S.A.). At the exact same time that the CE- MRA commenced, the injection of contrast medium (MagnevistⓇ, Schering, Korea) was started. The injection rate for the contrast medium without saline injection was set at 3.0 mL/second at a dose of 0.1 mmol/kg. Since
a multiphase technique was used, the image acquisition was started together with the injection of contrast medi- um so that no additional timing of the contrast medium’
s arrival in the AVF was need. This allowed the estima- tion of patient circulation time to ensure the optimal timing of the arterial phase imaging using MR fluo- roscopy. The VIBE images were obtained before admin- istration of contrast material and also during the arterial, venous, and equilibrium phases of contrast enhance- ment.
Image processing and data analysis
Post-processing of the fat-saturated 3D VIBE images was performed on a commercially available MR work- station. One investigator (YSL) evaluated the overall im- ages and performed reformations of the data sets before and after contrast administration. To increase the vessel- to-background contrast, the first (non-enhanced) 3D vol- ume was later subtracted on a partition basis from the subsequent identical scans that were obtained during the presence of contrast material. The subtraction was performed using commercially available software (Windows NTR, Siemens, Enlargen, Germany).
Compressing the subtracted images of each phase by means of maximum intensity projection post-processing created a dynamic subtraction contrast-enhanced MR angiogram.
The vessels of the upper extremity and the AVF were subdivided into three segments for analysis: the arterial segment, the anastomosis site and the venous segment.
Two radiologists (GYJ, YMH) prospectively analyzed the MRA by working in consensus. The DSA was used as the reference standard for assessing the accuracy of the MRA, and the MRA was analyzed for the presence of stenosis or occlusion, and a grading of stenosis and
Table 1. Summary of the Stenoses Identified with Digital Subtraction Angiography and Magnetic Resonance Angiography
N Age/Sex Type of Hemodialysis access Location of stenosis Grade of stenosis Collateral vessel
MRA DSA MRA DSA
1 32/F BC AS, vein III III (+) (+)
2 33/M BC AS, vein III III (+) (+)
3 68/M GRAFT AS I I (+) (+)
4 72/F GRAFT Intragraft Occlusion Occlusion ( - ) ( - )
5 39/F GRAFT Intragraft Occlusion III ( - ) ( - )
6 46/F BC AS, artery, vein III III ( - ) ( - )
7 60/F BC AS, vein III II (+) (+)
8 75/M GRAFT Intragraft Occlusion Occlusion ( - ) ( - )
9 53/M BC AS, artery, vein Occlusion III ( - ) ( - )
*AS=anastomosis site, BC=Brescia-Cimino arteriovenous fistula, GRAFT=synthetic polytetrafluoroethylene loop graft, MRA= magnet- ic resonance angiography, DSA= digital subtraction angiography
the presence of collateral vessels. A stenosis was diag- nosed if there was a focal narrowing: grade I was less than 25%, grade II was from 25% to 75%, and grade III was greater than 75% luminal reduction. If multiple stenoses existed, the most severe stenosis was assessed.
Occlusion was diagnosed if there was complete luminal signal loss within a patent vessel.
Statistical Analysis
The sensitivity and specificity of MRA for the detec- tion of AVF stenosis were calculated using DSA as the reference standard.
Results
There were 27 vessel segments available in 9 patients for the analysis with CE-MRA, and CE-MRA was suc- cessfully completed in all nine of these patients.
Regarding the stenotic grade, the CE-MRA correspond- ed with the DSA in six patients (66.7%) and it overesti- mated the stenoses in three patients (33.3%) (Table 1).
For the stenotic site, MRA had a sensitivity of 86.4%, a specificity of 40%, a positive predictive value of 32.1%
and a negative predictive value of 66.7%. Collateral or engorged vessels were demonstrated in four patients
having either a Brescia-Cimino arteriovenous fistula (n=3) or loop graft (n=1). CE-MRA showed findings similar to DSA in all four of these patients. Collateral or engorged vessels usually emerged from a prestenotic area in a vein.
Seven patients underwent successful percutaneous angioplasty and thrombolysis, and two patients had to be taken to surgery. One patient had severe engorge- ment or collateral vessels at the prestenotic venous site.
Although we performed percutaneous angioplasty on the stenotic area, the thrill didn’t completely disappear.
After carefully reviewing the MRA and DSA, we per- formed ligation of a side branch among the prestenotic vessels, and this caused a marked improvement of the thrill.
Disccusion
In this preliminary study, multiphase CE-MRA of the AVF provided non-invasive information comparable to the information provided by conventional angiography.
It was also a quick and easy examination that produced high-quality images. We can suggest that multiphase CE-MRA is a reliable and reproducible tool for the de- tection of flow-limiting stenoses that occur in hemodial-
A B C
Fig. 2. MIPs of a four phase CE-MRA (13 second intervals) and the DSA of a U-loop PTFE graft AVF obtained from the left arm of a 75-year-old male patient.
A. On oblique coronal view of a multiphase CE-MRA, occlusion of graft is shown (arrow).
B. CE-MRA of the occlusion site is shown with the corresponding DSA.
C. After we performed percutaneous angioplasty and thrombolysis on the stenotic area, the graft was patent on DSA.
ysis AVF (11).
In general, multiphase CE-MRA has some advantages;
1) it is not dependent upon a skillful examiner, 2) the pa- tient is not exposed to ionizing radiation, 3) it is not con- traindicated for patients with impaired renal function, 4) it takes a short time (15-20 min), and 5) the blood flow rate can be measured. However, multiphase CE-MRA still has some disadvantages. The field of view is limited due to the use of a surface coil. Also, CE-MRA detected a relatively large number of false positive lesions and the overestimation of stenosis can still not be avoided (10, 11).
In this study, we performed CE-MRA using VIBE.
VIBE is a 3D gradient-echo MRI technique tailored to- wards minimizing partial volume artifacts and maximiz- ing the image contrast. The VIBE sequence is achieved by asymmetric k-space sampling in the readout direc- tion and zero-filling in the section-select direction. The asymmetric echo in the read direction produces sharper images with fewer ringing artifacts and this permits the use of a narrower bandwidth. As a result, this sequence improves the SNR and the inplane spatial resolution.
With VIBE, it’s possible to use thinner sections than for the other sequences used for body MR, and this enables the use of fat saturation with a minimum of added imag- ing time. Therefore, very small caliber evaluations are feasible, and fat saturation improves the enhancement of vascular structures on gadolinium-enhanced MR an- giography. With those advantages of VIBE, we success- fully obtained good MR angiography results similar to those of DSA (13-18).
We suggest that this method is useful for evaluating venous stenosis or obstruction for the failing hemodialy- sis arteriovenous fistula before the interventional proce- dure. Although the optimal venous anatomy for AVF development is a single cephalic vein, in many cases the cephalic vein may have one or several accessory veins.
In all our cases, the patients who underwent Brescia- Cimino arteriovenous fistula had a stenotic vein and anastomosis site. Venous stenotic sites that occurred af- ter repeated needle punctures could have caused de- creased thrill and decreased blood flow. As a result, this can cause anastomotic occlusion. According to Liang et al. (1), retrograde catheterization is usually not feasible for thrombosed AVFs that have coexisting venous steno- sis and accessory veins. According to Hunter et al. (19), nine of 28 occlusions could not be crossed despite ag- gressive attempts from multiple directions. In our cases, PTA was not performed in two patients because they
had multiple stenoses and multiple collateral veins.
Hence, although it is very important to detect failing vascular access as early as possible for successful PTA, it is necessary to accurately evaluate the venous stenotic sites and any prestenotic vessels by using CE- MRA.
There were a few limitations with this study; first, we only had a small number of study patients. Therefore, the sensitivity and specificity of this MRI technique could have been affected by the small size of the patient group. Second, it’s expensive to performed MRA.
Third, 3D-contrast MRA still overestimated severe stenosis. In conclusion, CE-MRA of the AVF provided non-invasive information comparable to that provided by DSA for the vascular stenosis regarding the failing hemodialysis arteriovenous fistula. In the future, the use of CE-MRA will make to possible to provide more infor- mation regarding the failing hemodialysis arteriovenous fistula and it will help the physician classify those pa- tients who are candidates for PTA.
References
1. Liang HL, Pan HB, Chung HM, Ger LP, Fang HC, Wu TH, et al.
Restoration of thrombosed Brescia-Cimino dialysis fistulas by us- ing percutaneous transluminal angioplasty. Radiology 2002;223:
339-344
2. Sofocleous CT, Cooper SG, Schur I, Patel RI, Iqbal A, Walker S.
Retrospective comparison of the Amplatz thrombectomy device with modified pulse-spray pharmacomechanical thrombolysis in the treatment of thrombosed hemodialysis access grafts. Radiology 1999;213:561-567
3. Wasser MN. Magnetic resonance angiography of peripheral vascu- lar disease. J Comput Assist Tomogr 1999;23S:129-S133
4. Ruehm SG, Hany TF, Pfammatter T, Schneider E, Ladd M, Debatin JF. Pelvic and lower extremity arterial imaging: diagnostic performance of three-dimensional contrast-enhanced MR angiog- raphy. AJR Am J Roentgenol 2000;174:1127-1135
5. Finlay DE, Longley DG, Foshager MC, Letourneau JG. Duplex and color Doppler sonography of hemodialysis arteriovenous fistu- las and grafts. Radiographics 1993;13:983-999
6. Middleton WD, Picus DD, Marx MV, Melson GL. Color doppler sonography of hemodialysis vascular access: comparison with an- giography. AJR Am J Roentgenol 1989;152:633-639
7. Bos C, Smits JH, Zijlstra JJ, van Der Mark WA, Blankestijn PJ, Bakker CJ, et al. MRA of hemodialysis access grafts and fistulae using selective contrast injection and flow interruption. Magn Reson Med 2001;45:557-561
8. Cavagna E, D’Andrea P, Schiavon F, Tarroni G. Failing hemodial- ysis arteriovenous fistula and percutanous treatment: imaging with CT, MRI and digital subtraction angiography. Cardiovasc Intervent Radiol 2000;23:262-265
9. Waldman GJ, Pattynama PM, Chang PC, Verburgh C, Reiber JH, de Roos AD. Magnetic resonance angiography of dialysis access shunts: initial results. Magn Reson Imaging 1996;14:197-200 10. Smits JM, Bos C, Elgersma OE, van der Mark MA, Blankestijn PJ,
Bakker CJ, et al. Hemodialysis access imaging: comparison of
flow-interrpted contrast-enhanced MR angiography and digital subtraction angiography. Radiology 2002;225:829-834
11. Planken RN, Tordoir JM, Dammers R, de Haan MW, Oei TK, van der Sande FM, et al. Stenosis detection in forearm hemodialysis ar- teriovenous fistulae by multiphase contrast-enhanced magnetic resonance angiography: preliminary experience. J Magn Reson Imaging 2003;17:54-64
12. NKF-DOQI clinical practice guidelines for vascular access.
National kidney foundation-dialysis outcomes quality initiative.
Am J Kidney Dis 1997;30:150-191
13. Lee VS, Lavelle MT, Rofsky NM, Laub G, Thomasson DM, Krinsky GA, et al. Hepatic MR imaging with a dynamic contrast- enhanced isotropic volumetric interpolated breath-hold examina- tion: feasibility, reproducibility, and technical quality. Radiology 2000;215:365-372
14. Maki JH, Prince MR, Chenevert TL. Optimizing three-dimensional gadolinium-enhanced magnetic resonance angiography. Original investigation. Invest Radiol 1998;33:528-537
15. Lee HM, Wang Y, Sostman HD, Schwartz LH, Khilnani NM, Trost DW, et al. Distal lower extremity arteries: evaluation with two-di- mensional MR digital subtraction angiography. Radiology 1998;
207:505-512
16. Bader TR, Semelka RC, Pedro MS, Armao DM, Brown MA, Molina PL. Magnetic resonance imaging of pulmonary parenchy- mal disease using a modified breath-hold 3D gradient-echo tech- nique: initial observations. J Magn Reson Imaging 2002;15:31-38 17. Wetzel SG, Johnson G, Tan AG, Cha S, Knopp EA, Lee YS, et al.
Three-dimensional, T1-weighted gradient-echo imaging of the brain with a volumetric interpolated examination. AJNR Am J Neuroradiol 2002;23:995-1002
18. Rofsky NM, Lee VS, Laub G, Pollack MA, Krinsky GA, Thomasson D, et al. Abdominal MR imaging with a volumetric in- terpolated breath-hold examination. Radiology 1999; 212:876-884 19. Hunter DW, Castaneda-Zuniga WR, Coleman CC, Young AT,
Salomonowitz E, et al. Failing arterivenous dialysis fistulars: evalu- ation and treatment. Radiology 1984;152:631-635
대한영상의학회지 2004;51:609-614
기능부전 혈액투석동정맥루의 조영 증강 자기공명 혈관조영술: 예비 연구1
1전북대학교 의과대학 진단방사선과학교실
2전북대학교 의과대학 내과학교실
이영선・진공용・한영민・이상용・박학훈・박성광2
목적:기능부전 혈액투석동정맥루의 협착을 평가하는 데 있어 디지털 감산 혈관조영술과 비교시 조영 증강 자기공명 혈 관조영술의 유용성을 알아 보고자 하였다.
대상과 방법:기능부전 혈액투석동정맥루가 의심되는 환자 9명, 27개의 혈관을 대상으로 조영 증강 자기공명 혈관조영
술과 디지털 감산 혈관조영술을 시행하였다. 자가동정맥루는 5예였으며, 인조혈관동정맥루는 4예였고, 연령은 32-72 세(평균 53세)였다. 자기공명 혈관조영술 영상은 1.5 T의 자기공명영상장치에 위상배열 코일을 이용하였으며, VIBE 기법(TR/TE=3.5/1.5 msec, flip anlge 20-25°, matrix 115×256, FOV 350×350)으로 조영 전과 후의 영상을 영상 을 얻었다. DSA를 영상 분석에 있어서 기준으로 간주하였으며, 조영 증강 자기공명 혈관조영술상 혈관의 협착이나 폐 쇄의 유무, 협착의 위치(동맥, 동정맥루, 정맥), 정도(경도, 중등도, 고도)를 DSA에서의 소견을 기준으로 비교 평가하 였다.
결과:기능부전 혈액투석동정맥루의 협착정도는 6명의 환자(66.7%)에서 조영 증강 자기공명 혈관조영술이 디지털 감 산 혈관조영술과 일치하였으며, 3명의 환자(33.3%)에서는 과대평가 되었다. 협착에 대한 조영 증강 자기공명 혈관조 영술의 민감도는 86.4%, 특이도는 40%, 양성 예측도는 32.1%, 음성예측도는 66.7%였다.
결론:기능부전 혈액투석동정맥루의 협착된 혈관의 평가에 있어서 조영 증강 자기공명 혈관조영술은 비침습적으로 디 지털 감산 혈관조영술에 상응하는 정보를 제공할 수 있다.