C-Type Natriuretic Peptide as a Surrogate Marker in Variant Angina Pectoris
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
Brain natriuretic peptide predicts right heart failure in patients with acute pulmonary embolism. Kucher N, Printzen
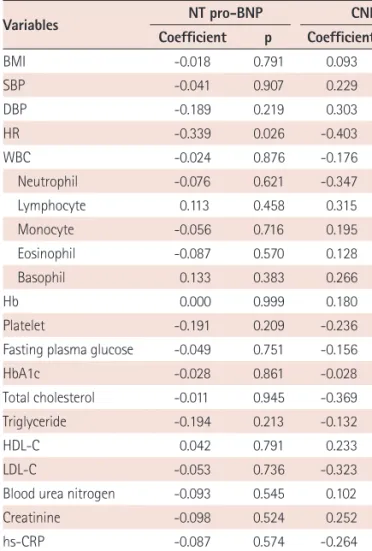
MACE, major adverse cardiac events; Tn-I, troponin-I; NT-proBNP, N- terminal proB-type natriuretic peptide; hs-CRP, high-sensitivity C-reactive protein; IHD, ischemic
The present study was designed to examine whether the bas- al C-peptide level correlates with cardiovascular risk in T2DM patients via comparison with IMT, the 10-year coronary heart
The multiple regression analysis also showed that basal C-peptide significantly correlated with IMT (P=0.043) but did not correlate with the ten-year coronary heart disease (CHD)
