Corresponding author: Moo Il Kwon, Department of Anesthesiology and Pain Medicine, Kyung Hee University Hospital, #1 Hoegi- dong, Dongdaemun-gu, Seoul 131-702, Korea
Tel: +82-2-958-8589, E-mail: [email protected] Received November 24, 2010, Revised December 5, 2010 Accepted December 10, 2010
Association between ARPC2 Polymorphisms and Kawasaki Disease in Korean Children
Departments of *Anesthesiology and Pain Medicine,
†Pediatrics, School of Medicine, Kyung Hee University, Seoul, Korea
Su Sang Jung*, Sung Wook Park*, Kyung Lim Yoon
†, Moo Il Kwon*
Kawasaki disease (KD) is an acute, self-limited vasculitis of infants and young children that predominantly affects the coronary arteries. KD is the leading cause of acquired heart disease among children in developed countries. We hypothesized that the actin related protein 2/3 complex, subunit 2, 34 kDa (ARPC2) gene may be related to the development of KD. In this study, the associations between single nucleotide polymorphisms (SNPs) of ARPC2 and KD were investigated in 111 KD patients and 429 healthy controls. Two promoter (rs6720105, −099G/A and rs6720449, −839G/A) and 5 intronic SNPs (rs12992937, rs10932765, rs10169718, rs6436047, and rs13430006) were selected, and genotypes of each SNP were analyzed using Affymetrix targeted genotyping chip. The genetic data of 7 SNPs were evaluated by SNPStats, SNPAnalyzer, Haploview, and Helixtree programs. Two promoter SNPs (rs6720105 and rs6720449) were weakly associated with KD. The SNP rs6720105 showed a statistical difference between KD and controls in the codominant model (OR=1.45, 95% CI=1.00∼2.10, p=0.042). The SNP rs6720449 also showed differences between KD and controls in the codominant (OR=1.47, 95% CI=1.02∼2.14, p=0.036) and dominant models (OR=1.55, 95% CI=1.01∼2.40, p=0.045), respectively. In the analysis of haplotypes, a haplotype (AATTAAG) was weakly associated with KD (frequency=0.249, chi square=3.867, p=0.049). The results suggest that ARPC2 may be associated with the development of KD in Korean children. (Korean J Str Res 2010;18:389∼394)
Key Words: Kawasaki disease, ARPC2, Single nucleotide polymorphism, Haplotype
INTRODUCTION
Kawasaki disease (KD) is an acute febrile vasculitis of infants and children characterized by prolonged fever, skin rash, erythema of the oral mucosa, palms, and soles, bilateral conjunctival injec- tion, and cervical lymphadenopathy. Coronary artery aneurysms
develop in 15 to 25% of untreated KD (Kato et al., 1975;
Vijayan et al., 2009; Rowley et al., 2010). KD is the leading
cause of acquired heart disease among children, and death occurs
in a small but significant percentage of KD patients. Admini-
stration of intravenous immunoglobulin (IVIG) reduces the
aneurysm rate to less than 5% in affected subjects (Tremoulet et
al., 2008; Udi et al., 2008; Hata et al., 2009; Galeotti et al.,
2010; Manlhiot et al., 2010). Although an infectious agent is
strongly implicated according to clinical and epidemiologic fea-
tures, no pathogen had been isolated. Accumulated evidences
suggest that genetic factors are related to the susceptibility and
outcome of KD. The incidence of KD is higher in Asians than
in Caucasians. The risk of KD is 10 times higher in siblings of affected individuals than in general population (Pinna et al., 2008;
Onouchi, 2009; Wood et al., 2009; Yeung, 2010).
Actin polymerization plays an important role in the change of cell shape and locomotion. An approximately 220-kD multi- protein complex induced actin polymerization is found from human platelet. This complex contains actin-related proteins (Arp2 and Arp3) and therefore was named the Arp2/3 complex.
The human Arp2/3 complex consists of 7 subunits: ARP2 (ACTR2), ARP3 (ACTR3), ARC41 (ARPC1B), ARC34 (ARPC2), ARC21 (ARPC3), ARC20 (ARPC4), and ARC16 (ARPC5) (Welch et al., 1997). The actin related protein 2/3 complex, subunit 2, 34 kDa (ARPC2) is one of seven subunits of the human Arp2/3 complex, and located at chromosome 2q36.1. Quantitative real- time RT-PCR analysis of 32 primary gastric cancer samples and 8 gastric cancer cell lines revealed that expressions of all seven subunits were significantly decreased (Kaneda et al., 2004). Single nucleotide polymorphism (SNP) of ARPC2 is associated with ulcerative colitis in Dutch population (Festen et al., 2010).
However, the exact genetic role of ARPC2 is largely unknown.
To investigate the possible relationship between ARPC2 and KD, two promoter and 5 intronic SNPs were evaluated in 111 KD patients and 429 contro1 subjects.
MATERIALS AND METHODS
1. Subjects
This study was approved by the Ethics Committee of the Medical Research Institute, School of Medicine, Kyung Hee University, Seoul, Korea. Blood samples were obtained with informed written consent from unrelated Korean subjects. One hundred and eleven KD patients were recruited at Kyung Hee University Hospital and East-west Neo Medical Center, Seoul, Korea. KD was diagnosed by well-trained physician. Four hundred and twenty nine healthy individuals were enrolled. In the control group, patients with diabetes, stroke, hypertension, and cardiac diseases were excluded. Blood samples for DNA extraction were collected in ethylenediamine tetraacetic acid (EDTA) tube.
Genomic DNA was extracted using DNA isolation kit (Nu- cleoSpin
Ⓡ) for mammalian blood (MACHEREY-NAGEL GmbH
& Co., Düren, Germany) and stored at −20
oC before use.
2. SNP Selection and Genotyping
We searched all SNPs of ARPC2 by the following criteria: (1) known heterozygosity; (2) minor allele frequency>0.05; (3) tagging SNPs (http://www.hapmap.org/ and http://www.ncbi.nlm.
nih.gov/SNP/). All coding SNPs of ARPC2 were unknown hetero- zygosity. Finally, two promoter (rs6720105, −1099G/A and rs6720449, −839G/A) and five intronic SNPs (rs12992937, rs10932765, rs10169718, rs6436047, and rs13430006) were selected. Genotyping was performed using Affymetrix targeted genotyping chip (Affymetrix, CA, USA) according to the manu- facturer protocol. In brief, PCR products by specific primers were purified. The purified products were end-labeled by terminal deoxynucleotidyl transferase. Labeled DNAs were hybridized and scanned. The scanned images were analyzed by GCOS software (Affymetrix).
3. Statistics
Statistical analyses were performed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA). Hardy-Weinberg equilibrium (HWE) for each SNP was assessed using SNPStats (http://bioinfo.iconcologia.net/
index.php). For the analysis of genetic data, SNPStats, HelixTree (Golden Helix Inc., Bozeman, MT, USA), and SNPAnalyzer (ISTECH Inc., Goyang, Korea) were used. Logistic regression models (codominant, dominant, and recessive) were used for odds ratios (ORs), 95% confidence intervals (CIs), and corresponding p values, controlling gender as a covariable. The linkage disequili- brium (LD) block was made by Haploview 4.2. For all statistical tests, the significance level was set at 0.05.
RESULTS
The mean age in KD patients was 2.8±2.1 (mean±SD) years.
Coronary artery lesions were present in 35 patients but absent in
76 patients. The standard treatment of 2 g/kg IVIG was admini-
stered to 90 patients. Of these 90 patients, 11 subjects needed
at least one extra dose of IVIG (data not shown). A total of 429
normal controls (mean age 36.8 years) were used as the control
group due to difficulty in obtaining a healthy infant control
group. Although it is ideal to use the control group of matched
age, however, it is not a major problem because it was reported
SNP Genotype Kawasaki Control Codominant
p Dominant
p
Recessive
p
Locus n (%) n (%) OR (95% CI) OR (95% CI) OR (95% CI)
rs6720105 G/G 71 (64.0) 231 (53.9) 1.45 (1.00∼2.10) 0.042
a1.52 (0.99∼2.34) 0.054 1.80 (0.62∼5.25) 0.250
−1099 A/G 36 (32.4) 171 (39.9) A/A 4 (3.6) 27 (6.3)
rs6720449 G/G 71 (64.5) 231 (54.0) 1.47 (1.02∼2.14) 0.036
a1.55 (1.01∼2.40) 0.045
a1.78 (0.61∼5.21) 0.260
−839 A/G 35 (31.8) 170 (39.7)
A/A 4 (3.6) 27 (6.3)
rs12992937 A/A 34 (30.6) 124 (28.9) 1.04 (0.77∼1.40) 0.820 1.09 (0.69∼1.71) 0.720 1.00 (0.59∼1.69) 1.000 Intron 1 T/A 55 (49.5) 220 (51.3)
T/T 22 (19.8) 85 (19.8)
rs10932765 C/C 33 (29.7) 123 (28.7) 1.03 (0.76∼1.39) 0.840 1.05 (0.67∼1.66) 0.830 1.03 (0.61∼1.74) 0.910 Intron 2 T/C 56 (50.5) 219 (51.0)
T/T 22 (19.8) 87 (20.3)
rs10169718 G/G 33 (29.7) 123 (28.7) 1.03 (0.76∼1.39) 0.840 1.05 (0.66∼1.66) 0.840 1.03 (0.61∼1.74) 0.910 Intron 3 A/G 56 (50.5) 218 (50.9)
A/A 22 (19.8) 87 (20.3)
rs6436047 C/C 34 (30.6) 124 (29.1) 1.03 (0.77∼1.40) 0.820 1.08 (0.68∼1.69) 0.750 1.01 (0.60∼1.70) 0.980 Intron 3 A/C 55 (49.5) 217 (50.9)
A/A 22 (19.8) 85 (19.9)
rs13430006 T/T 33 (29.7) 123 (28.7) 1.03 (0.76∼1.39) 0.840 1.05 (0.67∼1.66) 0.830 1.03 (0.61∼1.74) 0.910 Intron 4 T/G 56 (50.5) 219 (51.0)
G/G 22 (19.8) 87 (20.3)
a
p<.05, Genotype distributions are shown as number (%). p values were from logistic regression analyses with the codominant, dominant, and recessive models. OR: odds ratio, CI: confidence interval, n: number of subjects, APRC2: actin related protein 2/3 complex, subunit 2, 34 kDa, SNP: single nucleotide polymorphism.
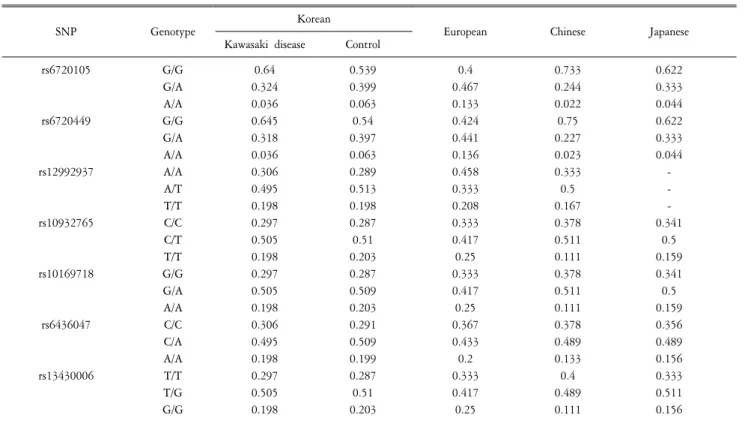
Table 1. Genotype frequencies of APRC2 SNPs in patients with Kawasaki disease and control subjects.
Fig. 1. Linkage disequilibrium (LD) block among ARPC2 SNPs. The block consists of rs6720105, rs6720449, rs12992937, rs10932765, rs10169718, rs6436047, and rs13430006. APRC2: actin related protein 2/3 complex, subunit 2, 34 kDa, SNP: single nucleotide polymorphism.
that the likelihood of the allele frequency changing according to age is quite low (Segal et al., 2003). The observed genotype distributions of all SNPs were in HWE (p>0.05, data not shown).
Multiple logistic regression analysis with adjustment for gender was performed. The genotype distributions of all SNPs are shown in Table 1. The promoter SNPs rs6720105 and rs6720449 were statistically associated with KD. The frequencies of GG, GA, and AA genotypes for the rs6720105 were 64.0%, 32.4%, and 3.6%
in the KD group, while they were 53.9%, 39.9%, and 6.3% in the control group, respectively. The SNP rs6720105 was asso- ciated with KD in the codominant (OR=1.45, 95% CI=1.00∼
2.10, p=0.042). The frequencies of GG, GA, and AA genotypes
for the rs6720449 were 64.5%, 31.8%, and 3.6% in the KD
group, while they were 54.0%, 39.7%, and 6.3% in the control
subjects. The SNP rs6720449 was associated with KD in the
codominant (OR=1.47, 95% CI=1.02∼2.14, p=0.036) and
dominant models (OR=1.55, 95% CI=1.01∼2.40, p=0.045),
Haplotype Frequency Kawasaki disease Control
Chi square p
+ − + −
GGACGCT 0.544 122 100 465 393 0.041 0.839
AATTAAG 0.249 44 178 225 633 3.867 0.049
aGGTTAAG 0.204 55 167 165 693 3.342 0.067
a