내피세포기능에
16
0
0
전체 글
(2) 예측은 향상되지 않았다.14). 관벽의 세포구성성분 안으로의 용매 운반을 조절,3) 혈. 다른 한편으로 관상동맥질환의 예측도는 LDL-cho15). 액내 강력한 유해 결과를 초래하는 물질과 세포로 부터. 16). 의 혈관 보호,4) 부분적 손상에 대한 혈액 응고, 염증, 그. 및 C-reactive protein 을 함. 리고 수선반응에 의한 혈관의 항상성을 유지하는, 대사. 께 측정하여 적용하였을 때 향상되었다. 치료전 및 치. 적으로 활발한 기관 체계이다. Nitric oxide는 혈관의. 료후의 LDL-cholesterol 농도와 심혈관계 end points. 건강을 유지시키고 혈관손상으로부터 보호하는 중심적. 의 상관관계를 몇몇 임상적 연구에서 평가하였다.2)4)8). 인 열쇠 역할을 한다. 그러나 고콜레스테롤혈증, 고혈압,. 아주 높은 위험도를 가진 그룹인 높은 LDL-choleste-. 흡연, 당뇨병, 울혈성 심부전, 폐고혈압, 에스트로젠 결. rol 수치를 가진 관상동맥질환 생존자를 대상으로 평가. 핍, hyperhomocysteinemia, 그리고 노화를 포함하는. 한 Scandinavian Simvastatin Survival Study에서도. 상태하에서는 endothelium이 손상되어 있는 것으로 알. 치료전 LDL-cholesterol 농도와는 관계없이 일정한. 려져 있다. 결과적으로 이들 상태들은 염증, 지단백의 산. 정도의 major coronary events가 감소됨을 관찰하였. 화, 평활근세포의 증식, 세포외 기질의 침착 혹은 분해,. lesterol 수치와 HDL-cholesterol, 17). plasma viscosity,. 2). fibrinogen, 18). West of Scotland Coronary Prevention Study. lipidrich 물질의 축적, 혈소판 활성, 그리고 혈전형성이. (WOSCOPS)에서는 심근경색증 발병은 없었지만, LDL-. 촉진될 것으로 추정된다. 내피세포기능 장애로 인한 이들. cholesterol 및 다른 요인으로 인하여 위험도가 높은. 결과들은 동맥경화의 진행 및 임상증세에 기여할 것이. 환자를 대상으로 치료동안 LDL-cholesterol 수치 혹. 다. 다시 말하면 endothelium의 기능장애가 관상동맥심. 은 총 콜레스테롤의 변화와 Framingham 관상동맥질. 장질환의 병인에 중요한 역할을 하는 것으로 여겨진다.. 환 위험도 모델을 이용한 관상동맥질환 위험도의 상관. 이런 점에서 급성관상동맥증후군 전,후에 시행된 연속. 다.. 4). Pravastatin 치료 환자군에서 관. 성 관상동맥조영술 연구결과를 보면 불안정형 협심증 및. 상동맥 위험도는 LDL-cholesterol 수치가 19%에서. 심근경색증의 원인인 경화반은 대부분의 경우 50% 미. 54% 범위에서 감소하였음에도 불구하고 LDL-cho-. 만의 협착을 보였다.24)25) 실제로 최근의 연구에서 심한. 관계를 평가하였다.. 4). leterol 수치변화 정도와는 상관관계가 없었다.. 협착을 보인 혈관의 수와 사망률간의 상관관계는 70%. Framingham 모델경우 위약군에서는 관상동맥질환. 이상의 협착을 가진 혈관수와 연관이 없고 다른 혈관에. 발생위험도를 정확히 예측하였으나, pravastatin 치료. 존재하는 minor plaque의 양과 밀접한 관계가 있는 것. 군에서는 관상동맥질환 위험도 감소는 35%까지 저평. 으로 보고되었다.26) 다혈관 관상동맥질환자가 한 개의. 가하였다. 이들 분석 결과는 nonlipid 기전들19)20)이. 관상동맥질환자에 비해 높은 사망률을 보이는 이유는. WOSCOPS에서 심혈관계질환의 발생을 감소시키고,. 앞으로 관상동맥증후군을 일으키는 병변인 비협착성이. 다른 몇가지 연구에서도 초기의 임상적 이로운 효과에. 거나 경한 협착성 경화반을 많이 가지고 있기 때문이라. 4)5)8)21)22). 관여할 것으로 최근에 제안되고 있다.. 고 할 수 있다. 급성심근경색증의 진행은 이미 존재하는. Endothelial 세포들은 신체에서 가장 광범위한 조직. 관상동맥협착과 상관관계를 가지지 않는다는 최근의 관. 구조물이다. 1980년도에 Furchgott와 Zawadzki23)는. 찰 및 연구결과24)25)는 다른 기전에 대한 연구를 추진토. endothelium이 동맥분절을 확장시키는 물질을 분비하. 록 하였다. 이러한 점에서 최근 상당히 많은 연구들에서. 는 것을 처음으로 관찰하였다. 그 이후부터 많은 연구. 동맥경화증 및 관상동맥 심장질환의 발병과 악화에 중. 가 이루어져 혈관운동에 대한 endothelium의 조절기전. 요한 인자로 흥미를 집중시키고 있는 것이 endothe-. 이 밝혀졌다. 그러나, 혈관운동의 조절이외에 endothe-. lium이다.. lium은 혈관건강을 유지시키고, 염증반응과 혈액응고같. Endothelium의 역할이 동맥경화증과 관상동맥 심장. 은 혈관손상에 대한 반응을 결정하는 여러 가지 중요한. 질환의 병인에 중요한 것으로 대두되고 있기 때문에 저. 특성을 가지고 있다.. 자들은 동맥경화증과 관상동맥 심장질환을 예방하거나. Endothelium은 오직 혈관 벽으로 순환하는 혈액의 유 1). 지연시킬 것으로 추정되는 endothelium에 대한 statin. 출을 방지하는 해부학적 장벽이라기 보다는 혈관운동. 의 효과 즉 혈관운동기능, 염증반응, 섬유소용해능력을. 조절,2) 부분적 세포성장, 세포외 기질 침착, 그리고 혈. 초점화하여 재조명하고자 한다. 1017.
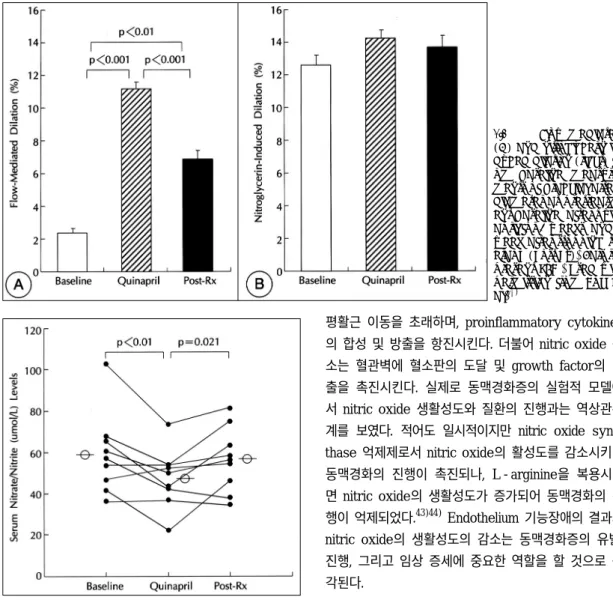
(3) 내피세포기능 장애의 기전과 결과들(Mechanisms and. 본. 문. consequences of endothelial dysfunction) 동맥경화증 고콜레스테롤혈증 동물모델에서 endo-. 산화질소와 고콜레스테롤혈증(Nitric oxide and hyper-. thelial 세포들은 superoxide anion 같은 높은 반응성. cholesterolemia). 을 가지는 분자들의 생산을 증가시키는 것으로 추정된 G. 고콜레스테롤혈증 환자에서 N -monomethyl-L-. 다.35) 기능장애가 있는 endothelium에서 nitric oxide. arginine(L-NMMA)는 정상인과 비교했을 때 기초 전. 의 합성이 실제로 증가 혹은 감소되어 있는지는 명확. 완(forearm) 혈류는 비슷한 효과를 가진다. 그러나, ace-. 하지 않다. Nitric oxide 생성증가의 가능성을 제시하는. tylcholine에 대한 전완 혈류의 L-NMMA 반응이 정. 실험으로 동맥경화성 토끼 대동맥에서 대조군의 조직. 상 콜레스테롤 농도를 가진 사람과 비교하였을 때 감소. 에 비해 nitrogen oxide의 분비가 증가되었다.36) 그리. 되는 현상은 기초상태에서 nitric oxide 방출은 보전되. 고 배양된 endothelium 세포에 LDL을 첨가시키면 ni-. 어 있지마는 endothelium의 자극동안에 nitric oxide. trogen oxide의 분비가 촉진되었다(특히 peroxynit-. 27). 그러나, 고혈압. rite).37) 산화된 LDL은 nitric oxide synthase의 tran-. 환자는 bradykinin에 대한 혈관 확장 반응이 손상되어. scription과 합성을 촉진하는 것으로 알려져 있다.38). 있는 반면에,28) 고콜레스테롤혈증 환자에서 bradykinin. 또한 사람의 동맥경화반에서 nitric oxide의 constitutive. 에 대한 혈관확장반응이 정상인 점은 고콜레스테롤혈증. form 보다 많은 양의 nitric oxide을 합성할 수 있는 in-. 에서 G-protein-dependent pertussis toxin-sen-. ducible form의 표현이 증가 됨이 관찰되었다.39) 그래. sitive signal transduction pathway에 부분적인 손상. 서, 고콜레스테롤혈증과 동맥경화증에서 혈관세포들이. 활성도는 감소되어 있음을 암시한다.. 29). 이 있음을 제시하는 것이라 하겠다.. 정상보다 많은 nitric oxide를 합성할 것으로 추정되지 만, 이들 nitric oxide는 과잉 생산된 superoxide anion. 산화 질소와 동맥경화증(Nitric oxide and atheroscl-. 및 free radical 분자들의 축적으로 신속한 산화과정을. erosis). 거쳐 불활성화 되거나 독성 nitrogen oxide로 전환된. 각기 다른 여러 연구들에서 관상동맥질환을 가진 환. 다. 최근에 Koh 등40)은 관상동맥질환을 가진 9명을 대. 자의 심외막 관상동맥들이 관상동맥조영술상 폐쇄성 동. 상으로 혈관 평활근세포에 작용하는 endothelial nitric. 맥경화증이 있는 부위와 경화반이 있는 부위에서 ace-. oxide의 bioassay로서 전완에 허혈에 따른 증가된. 30-32). tylcholine 반응에 수축을 보였다.. 반면에 동일한 용. shear stress로 인한 상완동맥의 확장반응을 고주파 초. 량의 acetylcholine은 관상동맥 질환의 증거가 없는 환. 음파로 측정하여 angiotensin 전환효소억제제인 quin-. 자에서 관상동맥혈관을 확장시켰다. 이들 2개의 군에서. april의 효과를 연구하였다. nitrate 제한식이를 3일간 실. acetylcholine에 대한 대조적인 반응과는 달리 nitro-. 시한 후에 endothelial nitric oxide 방출의 지표인 혈. glycerin(nitric oxide donor)에 대한 반응은 동일한데. 청 nitrogen oxide를 측정하였다. 환자는 하루에 quina-. 이는 적어도 경증의 동맥경화 혈관에서는 nitric oxide. pril 20~40 mg을 8주 동안 복용하였다. 치료전과 비. 에 대해 정상적인 평활근반응을 가지고 있음을 의미한. 교하여 quinapril 치료후에 flow-mediated dilation은. 다. 동맥경화증에 대한 위험인자들인 고콜레스테롤혈증,. 유의하게 증가되었다(Fig. 1). 그러나, quinapril 치료후. 남성, 노년, 흡연, 당뇨, 관상동맥질환을 가진 가족병력. 혈청 nitrogen oxide 수치는 치료 전과 비교할 때 19%. 등이 있으면서 정상소견의 관상동맥 조영상을 가진 환. 유의하게 감소되었다(Fig. 2). 이같은 결과는 quinapril. 자들에서도 acetylcholine에 의한 관상동맥혈관이 수축. 이 혈관벽내의 angiotensin Ⅱ-induced oxidant str-. 33)34). 이러한 관찰소견은 심외막 관상동. ess를 감소시켜 산화에 의한 nitric oxide 비활성화를. 맥혈관의 endothelium 기능장애가, 혈관촬영상 명백하. 방지함으로써 혈관항상성 유지를 위해 혈관운동조절에. 게 나타나거나 심근허혈 및 협심증을 일으키기에 충분. 요구되는 endothelium의 nitric oxide 합성을 감소시. 한 폐색이 발생되기 전에 먼저 관상동맥에서 일어나고. 켰기 때문으로 추정된다.. 반응을 보였다.. 있음을 보여주는 중요한 연구 결과이다. 1018. 고콜레스테롤혈증을 가진 환자와 관상동맥 경화증을 Korean Circulation J 1999;29(9):1016-1031.
(4) Fig. 1. Flow-mediated (A) and nitroglycerin-induced dilation (right) from baseline measurements of brachial artery diameter at pretreatment baseline, after quinapril for 8 weeks, and 1 week after stopping therapy (Post-Rx). Bars represent SEM. Used with permission from Koh et al.40). 평활근 이동을 초래하며, proinflammatory cytokines 의 합성 및 방출을 항진시킨다. 더불어 nitric oxide 감 소는 혈관벽에 혈소판의 도달 및 growth factor의 방 출을 촉진시킨다. 실제로 동맥경화증의 실험적 모델에 서 nitric oxide 생활성도와 질환의 진행과는 역상관관 계를 보였다. 적어도 일시적이지만 nitric oxide synthase 억제제로서 nitric oxide의 활성도를 감소시키면 동맥경화의 진행이 촉진되나, L-arginine을 복용시키 면 nitric oxide의 생활성도가 증가되어 동맥경화의 진 행이 억제되었다.43)44) Endothelium 기능장애의 결과와 nitric oxide의 생활성도의 감소는 동맥경화증의 유발, 진행, 그리고 임상 증세에 중요한 역할을 할 것으로 생 각된다. Fig. 2. Serum levels of nitrate/nitrite at respective pretreatment baseline, after quinapril for 8 weeks, and 1 week after stopping therapy (Post-Rx). Open circles represent mean values. Used with permission from Koh et al.40). 감염, 염증과 내피세포기능 장애(Infection, inflammation and endothelial dysfunction) 만성 감염과 죽상종 발생의 느린 진행과정과의 연관. 가진 환자에서 운동 혹은 정신적 stress 을 경험하. 성에 대해 많은 관심이 모아지고 있다.45)46) 실제로 인. 면, nitric oxide 합성의 감소 혹은 과도한 분해로 인해. 플루엔자 발생동안과 후에 심혈관질환의 사망률이 증가. 내장 평활근에 대한 nitric oxide 방출 감소와 nore-. 했다고 보고되었다.47) 이 현상은 허약한 노인층 뿐만아. pinephrine 같은 수축성자극에 혈관 감수성이 증가함42). 니라 과거에 건강한 중년층에서도 발생하는 것으로 나. 으로서 관상동맥 endothelium에 의한 혈관조절기능 손. 타났다. 박테리아 감염도 역시 심혈관계 위험도의 증가. 실로 인해 관상동맥과 체동맥이 수축되는 것으로 추정. 와 연관성이 있는 것으로 보인다. 이러한 관찰 소견들은. 된다. Nitric oxide 감소는 endothelin의 합성과 방출을. 감염이나 급성 체염증이 일시적으로 급성 심혈관계 사. 자극하여 혈관수축 장력을 높이고, growth factors 방. 건의 위험을 증가시킴을 암시한다. 이 증가된 위험은. 출 및 활성을 촉진하여 평활근 과증식과 intima내로의. 죽상종의 전체 양에 대한 급성 변화라기 보다는 이미 존. 41). 42). 1019.
(5) 재하는 죽상종에 혈전과 혈관경련이 발생하기 때문인 것. terleukin-1과 6, TNF-α들의 포괄적검사에서 azi-. 으로 여겨진다. 이러한 추정과 일치되게 안정형에서 불. thromycin 투여 6개월에 4가지 염증성 표식자가 향상. 안정형 협심증으로의 이행은 체 염증반응과 관련이 있. 된 결과를 관찰하였다. 그러나, 항체역가와 임상적 사건. 고,48) 급성 염증 표식자(cytokines, C-reactive pro-. 간에 유의한 차이는 관찰되지 않았다.. tein, and white cell count을 포함)는 심혈관계위험도 증가와 모두 연관되어 있음이 보고되었다.48-50) 흥미롭. 약물 스타틴(지질 저하제)의 생물학적 효과들(Biologi-. 게, 죽상종의 불안정성은 한 개의 경화반에 국한되지. cal effects of statins). 않고 다른 vascular beds 다수의 부위에서 나타날 수 있고, 이는 내재된 진행과정이 국소적이라기보다는 전. 스타틴의 혈관운동기능에 대한 효과(Effects of statins. 신적이라는 것을 암시한다.51). on vasomotor function). 어떻게 염증 혹은 감염이 atheroma와 관련된 위험. 고콜레스테롤혈증과 동맥경화증에서 endothelial-. 도를 변형시키는가? 박테리아 endotoxin, 혹은 어떤. mediated vasodilation이 손상되어져 있다.60)61) 동맥. proinflammatory cytokines(특히 TNFα)은 endo-. 경화증 환자에서 pravastatin과 lovastatin으로 콜레스. thelium 세포에서 nitric oxide와 혹은 어떤 vasodila-. 테롤을 낮추면 acetylcholine에 의한 혈관수축반응이. tor anti-aggregatory prostanoids 생성기능을 억제한. 억제 됨으로서 endothelium 기능이 개선 됨이 증명되. 52-54). 52)53). 었다.61)62)Simvastatin 치료는 말초의 산화질소를 매개. 를 대상으로 한 실험모델에서 관찰되었다. 건강한 자원. 로 한 혈관확장을 개선시킨다.63)64) Statin 치료에 의한. 자에서 endotoxin 또는 어떤 cytokines에 잠간의 노출. 관동맥 혈류와 혈관확장반응의 개선은 안정형 협심증. 에도 endothelium 의존성 이완기능이 많은 시일동안 손. 환자에서 일시적인 허혈을 감소시키고,65)66) 심근관류. 다.. 54). 이런 현상은 모든 동물 과 건강한 자원자. 52)53). 상되었으며,. 손상정도는 만성 위험인자에 의한 것. 보다 더 심하였다. 이런 현상을 endothelial “stunning” 53). 이라고 명명하였다.. 실험적 혹은 역학적 자료는 급성. 를 개선시킨다.67) Statin 치료는 endothelium의 기능 장애를 개선시키고 이로인해 임상증세 호전을 보이는 것으로 생각된다.. 감염이나 염증으로 인한 endothelium의 기능장애는 심근. Goode와 Heagerty68)는 18명의 고콜레스테롤혈증. 경색증과 불안정형 협심증에 대한 일시적 위험인자를. 환자에서 피하생검으로 소동맥을 분리하여 acetylcho-. 제공하며, 이는 비정상적 혈관반응을 자주 일으키지만. line과 이보다는 적은 정도인 nitroprusside에 대한 손. 약물치료에 나아질 수 있다고 보고하였다. 실제로 최근. 상된 확장 반응을 16명의 age, sex-matched 대조군. 몇 개의 연구에서 허혈성 심장질환자를 항생제로 치료. 의 소동맥과 비교 관찰하였다. 이들 환자중 10명에서. 한 후 고무적인 이득이 있음을 보고하였고, 불안정형. 지질저하치료를 받은 후 10개월에 생검을 다시 시행했. 협심증과 심근경색증의 발생이 유의하게 감소됨을 보. 으며, LDL 콜레스테롤 수치는 56%까지 감소하였다.. 55)56). 고하였다.. 하지만 이와는 대조적으로 Ridker등은. 이들 환자에서 치료 전과 치료 후를 비교했을 때 ace-. Chlamydia pneumoniae57) 또는 Herpes simplex 바. tylcholine과 nitroprusside에 대한 혈관확장기능이 유. 58). 이러스 또는 cytomegalovirus IgG seropo-sitivity. 의하게 개선됨을 관찰하였다. 최근에 Koh 등69)은 무작. 와 심근경색증 위험도의 연관성을 건강한 중년남성을. 위로 28명의 여성에게 매일 conjugated equine estro-. 대상으로 전향적 연구를 하였는데 연관성이 없는 것으. gen 0.625 mg, simvastatin 10 mg, 그리고 두가지 복. 로 보고하였다. 더욱이 seropositivity와 심근경색증을. 합요법으로 각각 6주간 치료하였다. Hyperemia와 nit-. 예측하는 염증 표식자인 C-reactive protein 농도와도. roglycerin에 대한 상완동맥의 확장반응은 고주파 초. 59). 역시 연관성이 없는 것으로 나타났다. Anderson 등. 음파로 측정되었다. 치료전과 비교하였을 때 simvastatin. 은 관상동맥질환이 있으면서 Chlamydia pneumoniae. 은 LDL-cholesterol을 25%까지 감소시켰다. 그리고. 항체에 혈청학적으로 양성인 환자를 대상으로 azithro-. simvastatin은 flow-mediated 확장을 4.3%에서 10%. mycin을 투여하여 무작위 이차적 예방연구를 시행하였. 까지 개선시켰다(Fig. 3). 고콜레스테롤혈증 환자에서. 다. 4가지 염증성 표식자인 C-reactive protein, in-. fluvastatin70) 혹은 LDL-apheresis71) 처치도 각각. 1020. Korean Circulation J 1999;29(9):1016-1031.
(6) nitric oxide의 방출을 반영하는 혈청 nitrate/nitrite77) 수치를 증가시킬 것이다”라는 가정하에 연구하였다. 그 러나, 이들 각각의 치료후 nitric oxide 방출의 증가를 반영하는 상완동맥의 flow-mediated dilation은 개선 되었지만, CEE 단독요법을 제외한 simvastatin 단독요 법 및 두가지 복합요법은 예상과 달리 혈청 nitrate/ nitrite 수치를 감소시키는 경향을 보였다. Statin치료 후의 nitric oxide의 혈관내강으로의 방출 감소는 endothelium과 염증세포들에서 산화된 지단백질과 free radical 분자들에 의한 nitic oxide의 분해가 감소됨으로 서 endothelium의 항상성을 유지하기 위하여 nitric oxide의 생성이 감소된 것으로 추정된다.78) Koh 등은 최 근의 다른 연구40)에서 위에 제시한 가설을 증명하였다 (Fig. 2). Fig. 3. Flow-mediated dilation before therapies (open bars) and following (hatched bars) CEE 0.625mg daily for 6 weeks (left), simvastatin 10mg daily for 6 weeks (center), and the combination of therapies daily for 6 weeks (right) in 28 hypercholesterolemic postmenopausal women. Standard error of the mean is identified by the error bars. Used with permission from Koh et al.69). Statin요법으로 지단백질 수치 및 LDL 산화방지에 대한 간접적인 효과 또는 nitric oxide의 합성 및 방출 에 대한 직접적인 효과로 개선된 nitric oxide의 생활성 도는 endothelium 의존성 혈관확장 뿐만아니라 혈소판 응집, 혈관벽의 endothelium 표면에 혈소판과 염증세 포의 부착, 혈관벽내의 평활근 세포들의 증식과 이동을. endothelium 의존성 혈관확장을 개선시켰다.. 촉진하는 인자들의 방출을 억제하는 많은 statin의 항. 에스트로젠 치료의 결과로 개선된 nitric oxide 생활. 동맥경화 효과를 설명해 준다.79) Statin의 지질을 낮추. 성도는 17β-estradiol로 에스트로젠 치료를 받은 폐경. 는 효과 뿐만 아니라 혈관운동기능을 개선시키는 효과. 기여성에서 혈관 nitric oxide 방출의(부분적인) 지표. 의 중요한 기전중의 하나는 free radical 분자로부터. 인 nitrogen oxides(nitrites, nitrates)의 혈장 수치가. nitric oxide의 분해를 방지하여 nitric oxide의 생활성. 치료전 혹은 대조군인 치료받지 않은 폐경기여성의 수. 도를 개선시키는 항산화 효과라고 할수 있다. 이점에 있. 치보다 높다는 관찰소견으로 알수있다.72) 어떤 연구들. 어서 Kleinveld 등80)은 23명의 고콜레스테롤혈증 환. 은 호르몬 대체요법이 chemiluminescence 혹은 ELISA. 자에서 18주동안 pravastatin 혹은 simvastatin을 복. 검사법으로 측정하였을 때 nitric oxide 수치가 증가됨. 용시켰을 때 LDL-콜레스테롤 수치는 36 %까지 감소. 을 관찰하였다.73)74) 그러나, 이들 연구는 nitrate-제한. 되었고, copper-catalyzed LDL oxidation의 비율과. 식이를 실시하지 않았다. 우리는 다른 연구에서 건강한. 범위도 역시 감소되었다. 또한 Statin 치료 후 LDL 입. 자원자 30명에서 nitrate-제한식이가 혈청 nitrogen. 자들은 단백질에 비해 상대적으로 지방이 적은 것으로. oxide 수치를 66.2±46.1에서 46.4±26.2 μmol/L(p. 바뀌어 산화가 비교적 안됨을 관찰하였다.81). 0.001)로 감소시킴을 관찰하였다. 최근 Koh 등69)75)은. LDL 수치의 감소와 LDL 입자구성의 변화보다 또. 혈청 nitrogen oxide 수치에 nitrate 식이(보통 하루에. 다른 HMG-CoA reductase inhibitor의 특성이 또한. 75 에서 100 mg 섭취함)가 영향을 미치는 것을 최소. 중요한 항산화기능을 일으킬 수 있다. 실제로 Giroux. 화하기 위해 치료전 연구와 치료후 연구를 실시하기 전. 등82)은 simvastatin이 조직배양에서 인간 대식세포에. 3일동안 nitrate-제한식이(하루에 15 mg 이하 섭취). 의한 superoxide anion 형성과 LDL 산화를 감소시키. 를 실시하였다.76). 는 것을 보고하였고, Girona 등83)은 최근에 simvastatin. 이 연구에서 Koh 등은 conjugated equine estro-. 이 지단백질 산화에서 나오는 알데하이드 생성을 감소. gen 또는 simvastatin 치료가“혈관내강으로 부분적. 시킴을 관찰하였는데 이는 simvastatin이 지단백질 입 1021.
(7) 자내에서 항산화제로서 역할을 함을 보여주는 연구결 84). 1 표현과 NF-kB 활성도를 하향조절함을 관찰하였다.. 과이다. 그러나, Palomaki 는 lovastatin이 metal ion-. 이 연구에서 atorvastatin이 신생내막 염증을 감소시키. independent oxidation에서 환원된 α-toco-pherol. 고, 동맥경화반을 안정화시킬 수 있다고 결론지었다.. 의 depletion time을 44%까지 감소시키고, metal ion-. 최근에 Pasterkamp 등92)은 파열되지 않은 동맥경화. dependent oxidation에서는 conjugated-diene 형성. 반 안에 염증세포의 유병율과 분포(local vs general). 의 lag time을 7%까지 단축함을 관찰하고 각각의 statin. 를 연구하였다. 대퇴 동맥과 관상동맥에서 대식세포에. 은 항산화작용에서 다르게 작용하리라 추정하였다. LDL. 대한 염색이 모든 횡절편의 45%와 41%에서 각각 관. 산화방지는 nitric oxide의 생활성도를 증가시키고, end-. 찰되었다. 섬유성 모자(fibrous cap)의 파열은 2개의 대. othelium 의존성 혈관운동 향상, 항염증성, 그리고 end-. 퇴동맥과 3개의 관상동맥 절편에서 관찰되었고, 항상. othelium의 항응고 특성을 개선시킨다.. 염증세포가 함께 존재하였다. CD68 혹은 acid phosphatase에 적어도 한개의 횡절편에서 양성으로 염색되. 스타틴의 염증에 대한 효과(Effects of statins on in-. 는 것은 대퇴동맥과 관상동맥에서 각각 84%와 71%. flammation). 관찰되었다. 이 연구 결과는 동맥경화성 대퇴동맥과 관상. 죽상종 형성 초기 단계에 단핵세포는 endothelium에 부착하고, subendothelial 공간으로 침투한다. Oxidized. 동맥에서 경화반의 cap 이나 shoulder에 염증이 가장 흔히 관찰되는 소견임을 보여준다.. LDL은 단핵세포에서 유도된 대식세포 표면의 대식세. 임상적 연구에 의하면 Abe 등93)은 고중성지방혈증. 포 수용체과 결합하여 foam cell을 생성한다. 대식세포. 과 낮은 HDL-cholesterol을 가진 환자에서 가용성 IC-. 와 T 임파구에 의해 분비되는 염증성 cytokine은 end-. AM-1과 VCAM-1의 수치가 증가됨을 관찰하였다.. othelium의 기능을 변형하고, 평활근세포 증식, collagen. Rohde 등94)은 92명의 외래 환자에서 동맥 경화증의 지. 85-87). 분해, 그리고 혈전증을 야기시킨다.. 88). Scalia 등 은. 표인 경동맥 intima-media 두께와 cell adhesion mo-. 토끼모델에서 고콜레스테롤혈증의 초기단계에 백혈구. lecule 사이에 상관관계가 있음을 관찰하였다. 이 연구. 와 endothelium의 상호작용에서 P-selectin, ICAM-. 에서 총경동맥 intimamedia의 두께를 3등분하여 나이. 1, 그리고 VCAM-1의 역할을 명확히 규명하였다. 그. 를 적용한 가용성 ICAM-1 수치를 계산하였을 때 단. 들은 고콜레스테롤 식이를 한 토끼의 intestinal micro-. 계별로 증가됨을 관찰하였다. 가용성 VCAM-1 역시 동. vascular endothelium안에서 면역조직화학적으로 end-. 일한 경향을 보였다. 이 연구는 혈청 cell adhesion mo-. othelial adhesion molecules가 상향조절 됨을 관찰하. lecule 들과 경동맥 intima-media 두께사이에 연관성. 였다. 실험모델에서 콜레스테롤 수치를 낮추면 동맥경화. 이 있음을 증명하였고, 체염증이 동맥경화 병변 발달에. 반 내에서 염증세포도 감소가 되었음을 관찰하였다.89)90). 중요한 역할을 할 것이라는 가정을 입증한 연구로 평가. 또한 고콜레스테롤혈증 환자의 in vitro 실험에서 고. 된다. 심장이식을 받은 환자에서 pravastatin 투여는. 정된 endothelium 세포에 고립된 단핵세포의 흡착이 증. cyclosporin으로 치료받은 환자에서 염증반응과 natural. 가되었으며, 이 반응은 lovastatin 및 simvastatin에 의. killer cell 활성도를 억제하는 것으로 보고되었다.95). 해서 감소되었음을 관찰하였다.90) Fluvastatin으로 치료. 최근에 Ridker 등96)은 Womens Health Study에 참. 받은 고콜레스테롤혈증 쥐에서 platelet activation fa-. 여한 건강한 여성 중에서 3년의 추적기간동안에 처음. ctor와 leukotrien B4에 의한 백혈구의 흡착 반응은 유의. 심혈관계 사건을 경험한 122명의 환자에서 미래의 심. 90). 하게 감소되었다.. 91). 최근에 Bustos 등 은 흥미로운. 혈관계 위험도에 대한 C-reactive protein의 기대치를. 실험 연구를 했다. 토끼 동맥경화증 모델에서 atorva-. 보고하였다. 심혈관계사건을 경험한 여성들에서 대조군. statin은 신생내막과 중막안에 동맥 대식세포의 침윤과. 에 비해 기저치의 C-reactive protein 수치가 아주 높. monocyte chemoattractant protein-1을 차단하는. 음을 관찰하였다. 기저치 C-reactive protein 수치가 가. 효과가 있었다. 동시에 atorvastatin은 배양된 혈관 평. 장 높았던 여성들에서 어떤 혈관사건의 위험도는 거의. 활근 세포안에 tumor necrosis factor alpha (TNF-. 5배 높았고, 심근경색증이나 뇌졸중의 위험도는 7배 높. α)로 유도되는 monocyte chemoattractant protein-. 았다. Strandberg 등97)은 simvastatin 혹은 atorvasta-. 1022. Korean Circulation J 1999;29(9):1016-1031.
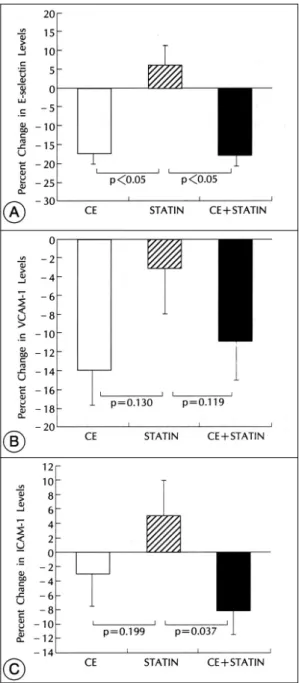
(8) tin이 고지혈증 관상동맥질환자에서 C-reactive protein. ester가 고체의 cholesterol crystal로 가수분해되는. 을 저하시킴을 관찰하였다.. 것은 더욱 단단한 경화반을 생성할 수 있을 것으로 추. 69). 최근 Koh 등 은 무작위로 28명의 여성에서 매일. 정된다. 이런 관점에서 Aikawa 등 103은 지질을 낮추. conjugated equine estrogen 0.625 mg, simvastatin 10 mg, 두가지 복합요법을 각각 6주간 투여하였다. 치료전과 비교하였을 때 simvastatin은 가용성 E-selectin, ICAM-1, 그리고 VCAM-1을 유의하게 변화 시키지 않았다.(Fig. 4) 흥미로운 것은 simvastatin은 28명의 폐경기 여성중에서 interleukin-6 level을 2.20 ±1.30에서 1.88±0.97 ng/ml로 유의하게 감소 시켰으며, 이는 Rosenson 등98)의 결과와 일치하였다. 그 럼에도 불구하고 simvastatin 치료는 nitric oxide 생 활성도의 지표로 간주되는 고주파 초음파에 의해 측정 된 상완동맥의 endothelium-의존성 확장을 유의하게 개선시켰다. 스타틴의 경화반 안정화에 대한 효과(Effect of statins on plaque stability) 죽상종내의 지질은 기계적 불안정화를 야기할 뿐만 아 니라 생리학적으로 활동적인 지질들은 산화 stress의 촉진과 단핵세포의 이동 같은 염증반응에도 관여한다. 그러므로 지질을 낮추는 것은 죽상종의 백혈구가 풍부 한 부위내에서 가장 활동적으로 나타나는 기질 분해 폭 포상반응(matrix degradation cascade)에 영향을 미 칠 수 있고, 또한 경화반내의 기계적 안정화를 가져올 수 있다. Statin은 phospholipid-containing pools안에 free cholesterol을 trapping 시켜 효소 acyl-coenzyme A cholesterol acyltransferase로 진행하는 free cholesterol의 활성도를 감소시키거나, cholesterol 에스트로 화에 요구되는 mevalonate와 mevalonate 부산물의 합성감소와 연관된 LDL 세포내이입(endocytosis)을 억제하여 단핵세포에서 유도된 대식세포에 cholesterol ester의 축적을 억제한다.99) Kempen 등100)은 pravastatin 보다 lovastatin과 simvastatin이 대식세포내 cholesterol의 축적에 용량 의존적 억제효과가 큰 것으 로 보고하였다. 따라서 혈중 LDL-cholesterol 수치를 낮추는 것이 경화반 크기를 감소101)시키거나 지질핵(lipid core)의 물리화학적 특성을 변형시킴102)으로서 경화반의 안정 성을 용이하게 할 것으로 생각된다. 액체의 cholesterol. Fig. 4. Percent change in the E-selectin (A), vascular cell adhesion molecule (VCAM-1)(B), and intercellular adhesion molecule (ICAM-1) levels (C) following CEE 0.6 25mg daily for 6 weeks (left), simvastatin 10mg daily for 6 weeks (center), and the combination of therapies daily for 6 weeks (right) in 28 hypercholesterolemic postmenopausal women. Standard error of the mean is identified by the error bars. Used with permission from Koh et al.69). 1023.
(9) 는 것이 platelet-derived growth factor-B 표현의. 집, 섬유소원, 혈장 점도, 그리고 섬유소용해 인자들이다.. 감소와 연관된 동맥경화 내막내 성숙된 평활근세포의 축적을 용이하게 하는 것을 관찰하였다.. 1. 응고체계(Coagulation system). 그리고 낮은 지혈증군(콜레스테롤 수치가 낮은 군)에 서 대조군 및 높은 지혈증군(콜레스테롤 수치가 높은. 1-1) Tissue factor. 군)과 비교하였을 때 matrix metalloproteinase-3와. Tissue factor와 이에 상응하는 messenger RNA는. -9의 표현이 감소됨을 관찰하였다. 다른 연구에서 Ai-. 사람 동맥경화반 대식세포에 위치하고 있다.108) Tiss-. kawa 등104)은 33마리의 토끼를 대상으로 풍선술을 이. ue factor는 plasma factor VII의 cofactor 및 factor. 용하여 혈관을 손상시킨 후 4개월동안 죽종형성식이를. Ⅶa에 대한 세포성 수용체로서 작용하고, 외인성 응고. 한후 지질에 의한 실험적 죽상종을 만들 수 있었다. 그. 경로(extrinsic coagulation pathway)의 시작에 중요. 들은 낮은 지혈증군에서 시간 경과에 따라 대식세포의. 한 역할을 한다.109) Brand등110)은 oxidized LDL이 사. 양과 matrix metalloproteinase-1 면역반응도가 점차. 람 점착 단핵세포내 lipopolysaccharide-induced tis-. 감소됨을 관찰하였다. Sirus red염색에 의해 측정되는. sue factor의 표현을 항진시킴을 관찰하였다. 지방친화. 대동맥의 간질성 교원질(interstitial collagen) 양은 낮. 성 statin인 fluvastatin과 simvastatin은 tissue factor. 은 지혈증군에서 기저군 혹은 계속적인 고지혈증군과 비. 생합성에 관여하는 geranylgeranylated protein를 억. 교하였을 때 증가되었는데, 이는 죽상종의 섬유화 골격. 제하여 배양된 대식세포에 대한 tissue factor 표현을. 강화를 의미하는 것이다. 실제로 Xu 등105)은 산화된. 억제시킨다.111) Tissue factor에 대한 이같은 효과는. LDL이 matrix metalloproteinase-9 표현을 상향 조. pravastatin에서는 관찰되지 않았다. Ferro등112)은 si-. 정하고, 단핵세포로 유도된 대식세포내 matrix me-. mvastatin이 Ⅱa 고콜레스테롤혈증 환자 24명에서 mo-. talloproteinase-1에 대한 조직억제물질은 감소시킴을. nocyte-tissue factor 표현을 감소시킴을 관찰하였다.. 106). 관찰하였다. Bellosta 등. 은 동맥경화반 균열을 가져. 외인성 응고 경로는 TFPI(tissue factor pathway. 오고 동맥 경화반의 섬유성 모자(fibrous cap)을 약화시. inhibitor)로 알려진 serine protease inhibitor에 의해. 키는 matrix metalloproteinase-9의 활성도에 대한. 견제되어진다. TFPI의 활성은 이형성 가족성 고콜레스. fluvastatin과 simvastatin의 효과를 쥐와 사람 대식 세포. 테롤혈증113)과 Ⅱa 및 Ⅱb 고지단백혈증114)환자에서 증. 를 배양하여 평가하였다. Fluvastatin은 대조군과 비교. 가되었다. Simvastatin은 factor Ⅶc의 유의한 변화없. 하여 용량 의존적으로 matrix metalloproteinase-9을. 이 LDL과 TFPI을 감소시켰다.115). 유의하게 감소시켰다. 뿐만 아니라 사람 단핵세포로 유 도된 대식세포내 matrix metalloproteinase-9 도 억 제시켰다. Simvastatin에서도 같은 결과를 관찰하였다.. 1-2) 혈소판 응집(Platelet aggregation) 높은 LDL 수치를 가진 환자의 혈소판이 정상인의 혈소판에 비해 응집인자에 더욱 민감하였다.116) Simva-. 지혈 표식자에 대한 스타틴의 효과(Effects of statins. statin은 치료 2주에 지질감소를 보였지만, 혈소판 응. on vascular hemostasis markers). 집과 thromboxane 생산의 감소는 치료 4주에서 24. 경화반 파열이 급성허혈 사건을 일으키는 지의 여부. 주 후에 관찰되었다.117) Lovastatin과 pravastatin도. 는 부분적으로 손상된 혈관벽에서 형성된 혈전의 성향. cytosolic 칼슘과 혈소판 응집을 감소시켰다.118) Statin. 에 의존한다. 혈전형성반응은 혈관벽 구성성분의 혈전. 은 아마도 혈소판막의 콜레스테롤 함량변화로 혈소판. 형성정도, 지방 pool이나 평활근 세포 그리고 proteog-. 막의 유동성을 변형시켜 혈소판 응집을 감소시킬 것으. lycans 복합체와 혈액구성성분과의 상호작용, 국부적인. 로 추정되고 있다.118). 혈류의 특성, 그리고 순환하는 지혈인자에 의해 영향받 는 것으로 추정된다. 최근에 Koh 등107)은 이 논쟁점들을. 1-3) 섬유소원과 점도(Fibrinogen and viscosity). 재조명하였다. 이 논문에서 statin 치료로 평가될 proth-. 섬유소원 수치와 혈장점도는 이미 관상동맥질환이 있. rombotic 인자들로는 tissue factor의 표현, 혈소판 응. 거나 없는 고지혈증 환자에서 심혈관계 위험도를 계층. 1024. Korean Circulation J 1999;29(9):1016-1031.
(10) 화하는데 이용되어져 왔다. 사실 Eriksson등119)은 스. inogen-regulating cytokine에 대한 작용차이, fibr-. 톡홀름에 사는 65세 이하의 여성을 대상으로 commu-. inogen gene locus에 유전자 변동을 가진 연구 모집. nity-based, casecontrol study에서 혈장 섬유소원이. 단,134) 그리고 측정법의 다양성에 기인하는 것으로 추. 관상동맥질환을 예측하는 능력을 평가하였다. 이 연구. 정되고 있다.135) 또 다른 고려될 요인은 장기 연구인 경. 에서 환자의 혈장 섬유소원 평균값이 대조군에 비해 통. 우 섬유소원 수치가 나이의 영향을 받는다는 것이다.136). 계적으로 유의하게 높았다. 혈장 섬유소원의 가장 낮은 4분위값에 대한 가장 높은 4분위값에 관상동맥심장질. 2. 섬유소용해 체계(Fibrinolytic system). 환에 대한 나이를 적용한 odds ratio는 6.0이었고, 지. Statin과 관련된 섬유소 용해기전에는 lipoprotein(a). 단백 콜레스테롤, 중성지방, 그리고 교육수준을 적용시. 와 섬유소용해체계에 주요 억제인자인 plasminogen. 켰을 때 odds ratio는 3.0 이었다. 증가된 혈장점도는. activator inhibitor(PAI)-1이 포함된다.. 미세순환 혈류의 손상, 혈액과 endothelium의 경계면 에 대한 shear stress 손상, 협착후 재순환지대내 end-. 2-1) Plasminogen activator inhibitor-1. othelium과 혈장 단백질 반응의 촉진, 그리고 혈전증 성. PAI-1의 상승에 의해 측정되는 손상된 섬유소용해. 120). 능력은 허혈성 심장질환자137)나 심근경색 생존자137-139). 고지혈증 환자를 대상으로 섬유소원 수치에 대한 st-. 에서 허혈성 심장질환의 예측인자이다. Koh 등140)은 여. atin의 효과를 평가한 몇개의 연구에서 혼합된 결과를. 성호르몬 에스트로젠 치료후에 PAI-1 항원 수치의 감. 보여준다. Lovastatin은 26명121)과 49명122)의 환자를. 소 정도가 D-dimer 수치의 증가 정도와 통계적으로. 대상으로 한 6개월 연구에서 섬유소원 수치가 각각 19 %. 유의한 상관관계를 가짐을 보고하였는데 이 결과는 에. 향의 증가로 동맥혈전증에 기여하는 것으로 여겨진다.. 123). 에서 24%까지 증가하였고, 260명. 의 환자를 대상으. 스트로젠이 섬유소용해를 향상시킴을 보여준 연구로 평 가된다.. 로 한 12개월 연구에서는 5%의 증가를 보였다. 그러나 15명과 35명의 환자를 대상으로 한 두 개의. 여러종류의 지질을 낮추는 약제들은 혈장의 지단백. 다른 단기간 연구에서는 섬유소원 농도의 변화는 관찰. 변화와는 독립적으로 섬유소용해를 강화시키는 것으로. 되지 않았다.124)125) 이와는 대조적으로 Mayer등126)은. 추정된다. Brown등141)은 간암세포배양에서 gemfibr-. 16 주간 lovastatin으로 치료한 20명의 고지혈증 환자. ozil과 niacin이 기초상태이거나 transforming grow-. 에서 섬유소원 수치가 10% 유의하게 감소됨을 관찰하. th factor-β1 같은 mitogen으로 세포를 자극한 후에. 였고, 12개월간 치료시에는 더욱 감소하였다. Lovastatin. 배양된 간암세포에서 PAI-1의 합성이 감소됨을 관찰. 127). 혈장점도는 감소. 하였다. 비록 인간에서 혈장 PAI-1 항원 수치에 대한. 시키거나124) 변화를 일으키지 않았다.125)127) Pravast-. 은 전혈 혈액점도를 증가시키지만,. niacin의 효과는 보고되지 않았지만, gemfibrozil과. atin은 16명에서 24명의 환자를 대상으로 10주에서. HMG-CoA reductase inhibitor인 pravastatin은 고. 24 주까지 치료하였던 3가지 연구에서 섬유소원 수치를. 지혈증 환자에서 PAI-1 혈장 수치를 감소시켰다.142)143). 7%에서 9%까지 감소시켰다.129)130) Simvastatin은 12. 약리학적으로 서로 다른 약제에 의한 PAI-1 억제의 세. 명에서 111명을 대상으로 10주에서 2년간 추적한 4가지. 포내 기전과 PAI-1의 endothelium에 의한 합성이 이러. 연구에서 섬유소원 수치는 변화되지 않았다.128)130)131). 한 약제들에 의해 영향을 받는 지는 알려져 있지 않다.. 더불어 simvastatin치료는 혈액, 혈장, 및 혈청의 점 131). Pravastatin은 PAI-1 항원 수치를 26%에서 56%. Atorvastatin(80 mg)은. 까지 감소시켜129) 섬유소용해를 촉진하는 것으로 나타. 22명의 이형성 가족성 고지혈증 환자를 대상으로 6주. 났다. Lovastatin은 PAI-1 항원을 22% 감소시켰으. 132). 간 치료하였을 때 섬유소원 수치가 46% 증가하였다.. 나,122) 260명의 환자를 대상으로 한 연구에서는 34%. 다른 연구에서 95명의 환자를 대상으로 하루에 10 mg. 증가시키는 상반된 결과가 관찰되었다.123) Atorvastatin. 에서 80 mg까지의 여러 용량을 투여하였을 때 섬유소. 은 12개월 후 PAI-1 항원을 36% 증가시켰다.123) Si-. 원 수치가 19%에서 24%까지 증가하였다.133). mvastatin은 111명의 환자를 대상으로 2년간 치료한. 도를 변화시키지 않았다.. 섬유소원 수치에 대한 statin의 상반된 효과는 fibr-. 경우 PAI-1 항원을 18% 증가시켰다.144) Fluvastatin 1025.
(11) Fig. 5. Percent change in the plasminogen activator inhibitor type-1 (PAI-1) following conjugated estrogen (CE) alone, simvastatin (statin) alone, and combination therapies. Standard error of the mean is identified by the bars. Used with permission from Koh et al.69). Fig. 6. Percent change in lipoprotein (a) from respective pr-etreatment values after CEE alone, simvastatin alone, and the combination of therapies daily for 6 weeks in 28 hyper-cholesterolemic postmenopausal women (p<0.001 by AN-OVA). SEM is identified by the bars. Used with permission from Koh et al.69). 은 PAI-1 항원에 중성효과를 보였다.145) 최근 Koh. tein(a) 증가의 임상적 의미는 아직 불분명하다. 아마. 69). 등 은 무작위로 28명의 여성을 대상으로 매일 con-. 도, 섬유소용해의 다른 매개체에 대한 statin의 상반된. jugated equine estrogen 0.625 mg, simvastatin 10. 효과가 서로 상쇄될 것으로 생각된다.. mg, 2가지 복합요법을 각각 6주간 투여하였다. 기초값. 결. 과 비교시 simvastatin 단독투여경우 PAI-1 항원 수. 론. 치는 19.2 ng/ml에서 18.6 ng/ml로 통계적으로 유의 하게 변화되지는 않았다(Fig. 5). 또한 simvastatin 단. Endothelium의 기능장애는 최근 실험적 혹은 임상. 독투여경우 섬유소의 교차결합 분해 산물인 혈청 D-. 적 연구에서 정상으로 회복될 수 있다는 고무적인 연구. dimer 수치도 유의하게 변하지 않았다.. 결과들이 보고되기 시작했다. Statin은 역학 및 임상시 험에서 endothelium의 기능을 개선시킴으로써, 치명적. 2-2) Lipoprotein(a). 이거나 치명적이지 않은 심근경색증의 발생을 유의하게. Lipoprotein(a)는 plasminogen 수용체, 섬유소원, 섬. 감소시키는 것으로 이미 잘 알려져있다. 따라서 내피세. 유소에 plasminogen이 결합하는데 plasminogen과 경. 포 기능장애의 치료에 대해 앞으로 더 많은 연구가 필. 쟁하여 섬유소용해를 방해한다.146) Lipoprotein(a)의. 요하며, 초기 동맥경화증과 더 나아가 관상동맥질환의. 147)148). 수치는 statin 치료로 34%까지 증가될 수 있고,. 치료에 내피세포기능장애의 치료는 앞으로 좋은 새로운. 따라서 강력하게 섬유소용해를 손상시킬 수있다. 최근. 치료법이 될 것이다. 이점에서 동맥경화증 예방 또는. 에 Koh 등69)은 무작위로 28명의 여성을 대상으로 매. 치료와 관련된 염증과 혈전형성반응에 대한 statin의. 일 conjugated equine estrogen 0.625 mg, simva-. 효과는 좀 더 많이 연구되어져야만 한다. 이는 건강 및. statin 10 mg, 그리고 2가지 복합요법을 각각 6주간. 질환에 대한 endothelium의 역할에 대하여 기초적・생. 투여한 연구에서 기초값과 비교하였을 때 simvastatin. 리학적・임상적 이해에 대한 병행된 노력이 있어야만. 단독투여경우 lipoprotein(a) 수치는 28.8 mg/ml에서. 이루어질 수 있다.. 31.8 mg/ml로 통게적으로 유의하게 변화되지는 않았. Statin의 항동맥경화증 특성의 범주에는 endothelium. 다(Fig. 6). 전반적인 심혈관 위험도에 대한 lipopro-. 기능의 유지, 항염증기능, 회복반응에 수반된 extra-. 1026. Korean Circulation J 1999;29(9):1016-1031.
(12) cellular matrix protein의 합성을 가능케하는 경화반. 11) The Expert Panel on Detection, Evaluation, and Treatment. 안정화가 포함된다. Statin은 경화반 파열후에 혈소판 침 착(deposition)과 응집(aggregation), 응고인자, 유동 학(reology), 그리고 섬유소용해에 대한 다양한 기능으 로 혈전형성에 영향을 준다. statin간의 질적 차이 또한. 12). 역시 심혈관계사건들의예방과 동맥경화성 질환의 악화 에 대한 효율성에 영향을 줄 수 있을 것으로 생각된다.. 13). 중심 단어 :동맥경화증・내피세포 기능・HMG-CoA 환원효소 억제제.. 14). REFERENCES 1) Ross R. Atherosclerosis-an inflammatory disease. N Engl 2). 3). 4). 5). 6). 7). 8). 9). 10). J Med 1999;340:115-26. Scandinavian Simvastatin Survival Study Group. Randomized trial of cholesterol lowering in 4444 participants with coronary heart disease: the Scandinavian Simvastatin Survival Study. Lancet 1994;344:1383-9. Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N Engl J Med 1996;335:1001-9. Shepherd J, Cobbe SM, Ford I, et al, for the West of Scotland Coronary Prevention Study Group. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. N Engl J Med 1995;333:1301-7. Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, et al. for the AFCAPS/TexCAPS Research Group. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 1998; 279:1615-22. Thompson GR, Hollyer J, Waters DD. Percentage change rather than plasma level of LDL-cholesterol determines therapeutic response in coronary heart disease. Curr Opin Lipidol 1995;6:386-8. Sacks FM, Gibson CM, Rosner B, Pasternak RC, Stone PH, and the Harvard Atherosclerosis Reversibility Project Research Group. The influence of pretreatment low density lipoprotein cholesterol concentrations on the effect of hypercholesterolemic therapy on coronary atherosclerosis in angiogr-aphic trials. Am J Cardiol 1995;76:78C-85C. Jukema JW, Bruschke AVG, van Boven AJ, et al. Effects of lipid lowering by pravastatin on progression and regression of coronary artery disease in symptomatic men with normal to moderately elevated serum cholesterol levels: The Regression Growth Ev-aluation Statin Study (REGRESS). Circulation 1995;91:2528-40. Williams JK, Sukhova GK, Herrignton DM, Libby P. Pravastatin has cholesterol lowering independent effects on the artery wall of atherosclerosis monkeys. J Am Coll Cardiol 1998;31:684-91 The Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Expert panel report of the national cholesterol education program arch intern med 1986;148:36-69.. 15). 16). 17) 18). 19) 20). 21). 22). 23) 24). 25). of High Blood Cholesterol in Adults. Summary of the second report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). JAMA 1993;269:3015-23. Pekkannen J, Linn S, Heiss G, et al. Tenyear mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N Engl J Med 1990;322:1700-7. Pekkannen J, Tervahuata M, Nissinen A, Karvonen MJ. Does the predictive value of baseline coronary risk factors change over a 30-year follow-up? Cardiology 1993;82: 181-90. Grover SA, Coupal L, Hu XP. Identifying adults at increased risk of coronary disease: How well do the current cholesterol guidelines work? JAMA 1995;274:801-6. Castelli WP, Garrison RJ, Wilson PWF, Abbott RD, Kalowsdian kS, Kannel WB. Incidence of coronary heart disease and lipoprotein cholesterol levels: The Framingham Study. JAMA 1986;256:2835-8. Thompson SG, Kienast J, Pyke SDM, Haverkate F, van de Loo JCW, for the European Concerted Action on Thrombosis and Disabilities Angina Pectoris Study Group. Hemostatic factors an HF, Yarnell JWG, Beswick AD, Ba-ker IA, Elwood d the risk of myocardial infarction or sudden death in patients with agnina pectoris. N Engl J Med 1995;332:635-41. Sweetnam PM, Thomas PC. Fibrinogen, viscosity, and the 10-year inci-dence of ischaemic heart disease. Eur Heart J 1996;17:1814-20. Ridker PM, Glynn RJ, Hennekens CH. C-reactive protein adds to the predictive value of total and HDL cholesterol in deter-mining risk of first myocardial infarction. Circulation 1998;97:2007-11. Vaughan CJ, Murphy MB, Buckley BM. Statins do more than lower cholesterol. Lancet 1996;348:1079-82. Kinlay S, Selwyn AP, Delagrange D, Creager MA, Libby P, Ganz P. Biological mechanisms for the clinical success of lipid-lowering in coronary artery disease and the use of surrogate end points. Curr Opin Lipidol 1996;7:389-97. The Pravastatin Multinational Study Group for Cardiac Risk Patients. Effects of pravastatin in patients with serum total cholesterol levels from 5.2 to 7.8 mmol/Liter (200 to 300 mg/dl) pl-us two additional atherosclerotic risk factors. Am J Cardiol 1993;72:1031-7. Byington RP, jukema JW, Salonen JT, et al. Reduction in cardiovascualr events during pravastatin therapy: Pooled analysis of clinical events of the Pravastatin Atherosclerosis Intervention Program. Circulation 1995; 92: 2419-25. Furchgott RF, Zawadzki JV. The obligatory role of the endo-thelial cells in the relaxation of arterial smooth muscle by acetyl-choline. Nature 1980;288:373-6. Ambrose JA, Tannenbaum MA, Alexopoulos D, et al. Angio-graphic progression of coronary artery disease and the development of myocardial infarction. J Am Coll Cardiol 1988;12:56-62. Little WC, Constantinescu M, Applegate RJ, et al. Can coronary angiography predict the site of subsequent myocardial infarction in patients with mild-to-moderate coro-. 1027.
(13) nary artery disease? Circulation 1988;78:1157-66.. 26) Nakagomi A, Celermajer DS, Lumley T, Freedman SB.. 27). 28). 29). 30). 31). 32). 33). 34). 35) 36). 37). 38). 39). 40). Angiographic severity of coronary narrowing is a surrogate marker of the extent of coronary atherosclerosis. Am J Cardiol 1996;78:516-9. Casino PR, Kilcoyne CM, Quyyumi AA, Hoeg JM, Panza JA. Role of nitric oxide in the endothelium-dependent vasodilation in hypercholesterolemic patients. Circulation 1993;88:2541-7. Panza JA, Garcia CE, Kilcoyne CM, Quyyumi AA, Cannon RO III. Impaired endothelium-dependent vasodilation in patients with essential hypertension: Evidence that nitric oxide abnormality is not localized to a single signal transduction pathway. Circulation 1995;91:1732-8. Gilligan DM, Guetta V, Panza JA, Garcia CE, Quyyumi AA, Cannon RO III. Selective loss of microvascular endothelial function in human hypercholesterolemia. Circualtion 1994;90:35-41. Ludmer PL, Selwyn AA, Shook TL, Wayne RR, Mudge GH, Alexander RW, Ganz P. Paradoxical vasoconstriction induced by acetylcholine in atherosclerotic coronary arteries. N Engl J Med 1986;315:1046-51. Zeiher AM, Drexler H, Wollschlager H, Just H. Modulation of coronary vasomotor tone in humans. Progressive endothelial dysfunction with different early stages of coronary atherosclerosis. Circulation 1991;83:391-401. Egashira K, Inou T, Hirooka Y, Yamada A, Maruoka Y, Kai H, et al. Impaired coronary blood flow response to acetylcholine in patients with coronary risk factors and proximal atherosclerotic lesions. J Clin Invest 1993;91: 29-37. Vita JA, Treasure CB, Navel EG, McLeanchan JM, Fish RD, Yeung AC, et al. Coronary vasomotor response to acetylcholine relates to risk factors for coronary artery disease. Circulation 1990;81:491-7. Quyyumi AA, Dakak N, Mulcahy D, Andrews NP, Husain S, Panza JA, Cannon RO III. Nitric oxide activity in the atherosclerotic human coronary circualtion. J Am Coll Cardiol 1997;29:308-17. Ohara Y, Peterson TE, Harrison DG. Hypercholesterolemia increases superoxide anion production. J Clin Invest 1993;91:2546-51. Minor RL, Myers PR, Guerra R, Bates JN, Harrison DG. Diet-induced atherosclerosis increases the release of nitrogen oxides from rabbit aorta. J Clin Invest 1990;86: 2109-16. Pritchard KA Jr, Groszek L, Smalley DM, Sessa WC, Wu M, Villalon P, et al. Native low-density lipoprotein increases endothelial cell nitric oxide synthase generation of superoxide anion. Circ Res 1995;77:510-8. Hirata K, Miki N, Kuroda Y, Sakoda T, Kawashima S, Yokoyama M. Low concentration of oxidized low-density lipoprotein and lysophosphatidylcholine upregulate constitutive nitric oxide synthase mRNA expression in bovine aortic endothelial cells. Ci-rc Res 1995;76:958-62. Buttery LD, Springall DR, Chester AH, Evans TJ, Standfield EN, Parums DV, et al. Inducible nitric oxide synthase is present within human atherosclerotic lesions and promotes to formation and activity of peroxynitrite. Lab Invest 1996;75:77-85. Koh KK, Bui MN, Hathaway L, Csako G, Waclawiw MA,. 1028. 41). 42). 43). 44). 45) 46) 47) 48). 49) 50) 51). 52) 53). 54) 55). 56). Panza JA, Cannon RO III. Mechanism by which quinapril improves vascular function in coronary artery disease. Am J Cardiol 1999;83:327-31. Gordon JB, Ganz P, Nabel EG, Fish RD, Zebede J, Mudge GH, Alexander RW, Selwyn AP. Atherosclerosis influences the vasomotor response of epicardial coronary arteries to exercise. J Clin Invest 1989;83:1946-52. Cardillo C, Kilcoyne CM, Quyyumi AA, Cannon RO III, Panza JA. Role of nitric oxide in the vasodilator response to mental stress in normal subjects. Am J Cardiol 1997; 80:1070-4. Cayette AJ, Palacino JJ, Horten K, Cohen RA. Chronic inhibition of nitric oxide production accelerates neointimal formation and impairs endothelial function in hypercholesterolemic rabbits. Athroscler Thromb 1994;14: 753-9. Hamon M, Vallet B, Bauters C, Wernert N, McFadden EP, Lablanche J-M, et al. Long term oral administration of L-arginine reduces intimal thickening and enhances neoendothelium-dependent acetylcholine-induced relaxation after arterial injury. Circulation 1994;90:1357-62. Ross R. The pathogenesis of atherosclerosis: A perspective for the 1900s. Nature 1993;362:801-9. Fuster V, Badimon L, et al. The pathogenesis of coronary artery disease and acute coronary syndromes. N Engl J Med 1992;326:242-50, 310-8. Tillet HE, Smith JW, Gooch CD. Excess deaths attributable to influenza in England and Wales: Age at death and certified cause. Int J Epidemiol 1983;12:44-52. Liuzzo G, Biasucci LM, Gallimore JR, et al. The prognostic value of C-reactive protein and serum amyloid A protein in severe unstable angina. N Engl J Med 1994; 331:417-24. Brody JI, Pickering NJ, Capuzzi DM, et al. Interleukin1 alpha as a factor in occlusive vascular dissease. Am J Clin Pathol 1992;97:8-13. Kanda T, Hirao Y, Oshima S, et al. Interleukin-8 as a sensitve marker of unstable coronary artery disease. Am J Cardiol 1996;77:304-7. Gates P, Marwood S, Jelinek M, Scott M. Unreported symptomatic and asymptomatic ischaemic heart disease in patients presenting with TIA or minor stroke detected by the London School of Hygiene Cardiovascular Questionnaire and Minnesota coding of a routine ECG. Clin Exp Neurol 1987;24:21-5. Bhagat K, Vallance P. Inflammatory cytokines impair endothelium-dependent dilatation in humans, in vivo. Circulation 1997;96:3042-7. Bhagat K, Moss R, Collier J, Vallance P. Endothelial stunning following a brief exposure to endotoxin-a mechanism to link infection and infarction. Cardiovasc Res 1996;32:822-9. Wang P, Ba ZF, Chaudry IH. Administration of tumor necrosis factoralpha in vivo depresses endothelium-dependent relaxa-tion. Am J Physiol 1994;266:H2535-H2541. Gupta S, Leatham EW, Carrington D, et al. Elevated chlamydia pneumoniae antibodies, cardiovascular events, and azithromycin in male survivors of myocardial infarction. Circulation 1997;96:404-7. Gurfinkel E, Bozovich G, Caroca A, Beck E, Mautner B. Randomized trial of roxithromycin in non-Q-wave coron-. Korean Circulation J 1999;29(9):1016-1031.
(14) 57). 58). 59). 60). 61). 62). 63). 64) 65). 66) 67). 68) 69). 70). ary syndromes:ROXIS Pilot Study. ROXIS Study Group. Lancet 1997;350:404-7. Ridker PM, Kundsin RB, Stampfer MJ, Poulin S, Hennekens CH. Prospective study of chlamydia pneumoniae IgG seropositive and risks of future myocardial infarction. Circualtion 1999;99:1161-4. Ridker PM, Hennekens CH, Stampfer MJ, Wang F. Prospective study of herpes simplex virus, cytomegalovirus, and risks of future myocardial infarction and stroke. Circualtion 1998;98:2796-9. Anderson JL, Muhlestein JB, Carlquist J, Allen A, Trehan S, Nielson C, et al. Randomized secondary preventional trial of azithromycin in patients with coronary artery disease and serological evidence for infection. The azithromycin in coronary artery disease: Elimination of myocardial infarction with Chlamydia (AC-ADEMIC) Study. Circualtion 1999;99:1540-7. Leung W-H, Lau C-P, Wong C-K. Beneficial effect of cholesterol-lowering therapy on coronary endothelium-dependent relaxation in hypercholesterolemic patients. Lancet 1993;341:1496-5020. Anderson TJ, Meredith IT, Yeung AC, Frei B, Selwyn AP, Ganz P. The effect of cholesterol-lowering and antioxidant therapy on endothelium-dependent vasomotion. N Engl J Med 1995;332:488-93. Treasure CB, Klein JL, Weintraub WS, Talley JD, Stillablower ME, Kosinski AS, et al. Beneficial effects of cholesterollowering therapy on the coronary endothelium in patients with coronary artery disease. N Engl J Med 1995;332:481-7. Stroes ESG, Koomans HA, deBruin TWA, Rabelink TJ. Vascular function in the forearm of hypercholestreolaemic patients off and on lipid-lowering medication. Lancet 1995;346:467-71. ODriscoll G, Green D, Taylor RR. Simvastatin, an HMGCoA reductase inhibitor, improves endothelial function within 1 month. Circulation 1997;95:1126-31. van Boven AJ, Jukema JW, Zwinderman AH, Crijns HJ, Lie KI, Bruschke AVG. Reduction of transient myocardial ischemia with pravastatin in addition to the conventional treatment in pati-ents with angina pectoris. Circulation 1996;94:1503-5. Andrews TC, Raby K, Barry J, et al. Effect of cholesterol reduction on myocardial ischemia in patients with coronary disease. Circulation 1997;95:324-8. Aengevaeren WRM, Uijen GJH, Jukema JW, Bruschke AVG, Werf T. Functional evaluation of lipid-lowering therapy by pravastatin in the Regression Growth Evaluation Statin Study. Circu-lation 1997;96:429-35. Goode GK, Heagerty AM. In vitro responses of human peripheral small arteries in hypercholesterolemia and effets of therapy. Circulation 1995;91:2898-903. Koh KK, Cardillo C, Bui MN, Hathaway L, Csako G, Wacl-awiw MA, et al. Vascular effects of estrogen and chlesterol-lowering therapies in hypercholesterolemic postmnopausal women. Circulation 1999;99:354-60. John S, Schlaich MS, Langenfeld M, Weihprecht H, Schmitz G, Weidinger G, et al. Increased bioavailability of nitric oxide after lipid-lowering therapy in hypercholeterolemic patients: A randomized, placebo-controlled, doule-blind study. Circulation 1998;98:211-6.. 71) Tamai O, Matsuoka H, Itabe H, Wada Y, Kohno K, Tsuto-. 72). 73). 74). 75). 76) 77) 78) 79) 80). 81). 82). 83) 84). 85). 86) 87). mu I. Single LDL apheresis improves endothelium-dependent vasodilatation in hypercholesterolemic humans. Circulation 1997;95:76-82. Rosselli M, Imthurn B, Keller PJ, Jackson EK, Dubey RK. Circulating nitric oxide (nitrite/nitrate) levels in postmenopausal women substituted with 17β-estradiol and norethisterone. Hyperten-sion 1995;25(part 2) :848-53. Best PJM, Begher PB, Miller VM, Lerman A. The effect of estrogen replacement therapy on plasma nitric oxide and endothe-lin-1 levels in postmenopausal women. Ann Intern Med 1998;128:285-8. Kim YD, Chen B, Beauregard J, Kouretas P, Thomas G, Farhat MY, et al. 17β-Estradiol prevents dysfuncton of canine coronary endothelium and myocardium and reperfusion arrhythmias after brief ischemia/reperfusion. Circulation 1996;94:2901-8. Koh KK, Blum A, Hathaway L, Csako G, Waclawiw M, Panza JA, et al. Effects of estrogen and vitamin E therapies on vascular function in postmenopausal women. Circulation 1999(in press). White JW Jr. Relative significance of dietary sources of nitrate and nitrite. J Agric Food Chem 1975;23:886-91. Wennmalm A, Benthin G, Edlund A, et al. Metabolism and excretion of nitric oxide in humans. An Experimental and clinical study. Circ Res 1993;73:1121-7. Buga GM, Griscavage JM, Rogers NE, Ignarro LJ. Negative feedback regulation of endothelial cell function by nitric oxide. Circ Res 1993;73:808-12. Cooke JP, Tsao PS. Cytoprotective effects of nitric oxide. Circu-lation 1993;88:2451-5. Kleinveld HA, Demacker PNM, De Haan AFJ, Stalenhoff AFH. Decreased in vitro oxidizability of low-density lipoprotein in hypercholesterolemic patients treated with 3hydroxy-3-methylglu-taryl-CoA reductase inhibitors. Eur J Clin Invest 1993;23:289-95. Lavy A, Brook GJ, Canker G, Amotz AB, Aviram M. Enhanced in vitro oxidation of plasma lipoproteins derived from hyper-cholesterolemic patients. Metabolism 1991; 40:794-9. Giroux LM, Davignon J, Naruszewicz M. Simvastatin inhibits the oxidation of low-density lipoproteins by activated human mo-nocyte-derived macrophages. Biochim Biophys Acta 1993;1165:335-8. Girona J, La Ville AE, Sola R, Plana N, Masana L. Simvastatin decreases aldehyde production derived from lipoprotein oxidation. Am J Cardiol 1999;83:846-51. Palomaki A, Malminiemi K, Malminiemi O, Solakivi T. Effects of lovastatin therapy on susceptibility of LDL to oxidation during α-tocopherol supplementation. Arterioascler Thromb Vasc Biol 1999;19:1541-8. Warner SJC, Friedman GB, Libby P. Immune interferon inhibits proliferation and induces 2-5-oligoadenylate synthetase gene expression in human vascular smooth muscle cells. J Clin Invest 1989;83:1174-82. Vallance P, Collier J, Bhagat K. Infection, inflammation, and infarction: Does acute endothelial dysfunction provide a link? Lancet 1997;349:1391-2. Neumann FJ, Marx N, Gawaz M, et al. Induction of cytokine expression in leukocytes by binding of thrombinstimulated platelets. Circulation 1997;95:2387-94.. 1029.
(15) 88) Scalia R, Appel JZ III, Lefer AM. Leukocyte-endothelium. 89). 90). 91). 92). 93). 94). 95) 96). 97) 98) 99). 100). 101) 102). interaction during the early stages of hypercholesterolemia in the rabbit. Arterioscler Thromb Vasc Biol 1998; 18:1093-100. Weber C, Erl W, Weber KSC, Weber PC. HMG-CoA reductase inhibitors decrease CD11b expression and CD11bdependent ad-hesion of monocytes to endothelium and reduce increased adhesiveness of monocytes isolated from patients with hypercholesterolemia. J Am Coll Cardiol 1997;30:1212-17. Kimura M, Kurose I, Russell J, Granger DN. Effects of fluvastatin on leukocyte-endothelial cell adhesion in hypercholesterolemic rats. Arterioscler Thromb Vasc Biol 1997; 17:1521-6. Bustos C, Hernandez-Presa MA, Ortego M, Tunon J, Ortega L, Perez F, et al. HMG-CoA reductase inhibition by atorva-statin reduces neointimal inflammation in a rabbit model of atherosclerosis. J Am Coll Cardiol 1998; 32:2057-64. Pasterkamp G, Schoneveld AH, van der Wal AC, Hijnen D-J, van Wolveren WJA, Plomp S, et al. Inflammation of the atherosclerotic cap and shoulder of the plaque is a common and locally observed feature in unruptured plaques of femoral and coronary arteries. Arterioscler Thromb Vasc Biol 1999;19:54-8. Abe Y, El-Masri B, Kimball KT, Pownall H, Reilly CF, Osmundsen K, et al. Soluble cell adhesion molecules in hypertriglyceridemia and potential significance on monocyte adhesion. Arterioscler Thromb Vasc Biol 1998;18: 723-31. Rohde LE, Lee RT, Rivero J, Jamacochian M, Arroyo LH, Briggs W, et al. Circulating cell adhesion molecules are correlated with ultrasound-based assessment of carotid atherosclerosis. Arterioscler Thromb Vasc Biol 1998; 18:1765-70. Kobashigawa JA, Katznelson S, Laks H, et al. Effect of pravastatin on outcomes after cardiac transplantation. N Engl J Med 1995;333:621-7. Ridker PM, Buring JE, Shiha J, Matias M, Hennekens CH. Prospective study of C-reactive protein and the risk of the future cardiovascular events among apparently healthy women. Circulation 1998;98:731-3. Strandberg TE, Vanhanen H, Tikkanen MJ. Effect of statins on C-reactive protein in patients with coronary artery disease. Lancet 1999;353:118-9. Rosenson RS, Tangney CC, Casey LC. Inhibition of proinflammatory cytokine production by pravastatin. Lancet 1999;353:983-4. Bernini F, Didoni G, Bonfadini G, Bellosta S, Fumagalli R. Requirement for mevalonate in acetylated LDL induction of cholesterol esterification in macrophages. Atherosclerosis 1993;104:19-26. Kempen HJM, Vermeer M, de Wit E, Havekes LM. Vastatins inhibit cholesterol ester accumulation in human monocyte-derived macrophages. Arterioscler Thromb 1991; 11:146-53. Armstrong ML, Warner E, Connor W. Regression of coronary atheromatosis in rhesus monkeys. Circ Res 1970; 27:59-67. Small DM. Progression and regression of atherosclerotic lesi-ons: Insights from lipid physical biochemistry. Arterio-. 1030. sclerosis 1988;8:103-29.. 103) Aikawa M, Rabkin E, Voglic SJ, Shing H, Nagai R,. 104). 105). 106). 107) 108). 109) 110). 111) 112). 113). 114). 115). 116) 117). Schoen F, et al. Lipid lowering promotes accumulation of mature smooth muscle cells expressing smooth muscle myosin heavy cha-in isoforms in rabbit atheroma. Circ Res 1998;83:1015-26. Aikawa M, Rabkin E, Okada Y, Voglic SJ, Clinton SK, Brinckerhoff CE, et al. Lipid lowering by diet reduces matrix metalloproteinase activity and increases collagen content of rabbit atheroma:A potential mechanism of lesion stabilization. Circulation 1998;97:2433-44. Xu X-P, Meisel SR, Ong JM, Kaul S, Cercek B, Rajavashisth TB, et al. Oxidized low-density lipoprotein regulates matrix metalloproteinase-9 and its tissue inhibitor in human monocyte-derived macrophages. Circulation 1999; 99:993-8. Bellosta S, Canavesi VM, Pfister P, Fumagalli R, Paoletti R, Bernini F. HMG-CoA reductase inhibitors reduce MMP-9 secretion by macrophages. Arterioscler Thromb Vasc Biol 1998;18:1671-8. Koh KK, Horne MK III, Cannon RO III. Effects of hormone replacement thrapy on coagulation and fibrinolysis in postmeno-pausal women. Thromb Haemst 1999(in press). Wilcox JN, Smith KM, Schwartz SM, Gordon D. Localization of tissue factor in the normal vessel wall and in the athero-sclerotic plaque. Proc Natl Acad Sci USA 1989;86: 2839-43. Nemerson Y. Tissue factor and haemostasis. Blood 1988; 71:1-8. Brand K, Banka CL, Mackman N, Terkeltaub RA, Fan S-T, Curtiss LK. Oxidized LDL enhances lipopolysaccharide-induced tissue factor expression in human adherent monocytes. Arte-rioscler Thromb 1994;14:790-7. Colli S, Eligini S, Lalli M, Camera M, Paoletti R, Tremoli E. Vastatins inhibit tissue factor in cultured human macrophages. Arterioscler Thromb Vasc Biol 1997;17:265-72. Ferro D, Basilli S, Alessandri C, Mantovani B, Cordova C, Violi F. Simvastatin reduces monocyte tissue-factor expression type IIa hypercholesterolaemia. Lancet 1997; 350:1222. Hansen JB, Huseby NE, Sandset PM, Svensson B, Lyngmo V, Nordoy A. Tissue factor pathway inhibitor and lipoproteins: Evidence for association with and regulation by LDL in human plasma. Arterioscler Thromb 1994; 14:223-9. Zitoun D, Bara L, Basdevant A, Samama MM. Levels of factor VIIc associated with decreased tissue factor pathway inhibi-tor and increased plasminogen activator inhibitor-1 in dyslipide-mias. Arterioscler Thromb Vasc Biol 1996;1:77-81. Sandset PM, Lund H, Norseth J, Abildgaard U, Ose L. Treatment with hydroxymethyl- glutaryl coenzyme A reductase inhibitors in hypercholesterolemia induces changes in the components of the extrinsic coagulation system. Arteriolscler Thromb 1992;11:138-45. Carvalho AC, Colman RW, Less RS. Platelet function in hyperlipoproteinemia. N Engl J Med 1974;290:434-8. Nortarbartolo A, Davi G, Averna M, et al. Inhibition of thromboxane biosynthesis and platelet function by simvastatin in type IIa hypercholesterolemia. Arterioscler Thromb Vasc Biol 1995;15:247-51.. Korean Circulation J 1999;29(9):1016-1031.
(16) 118) Le Quan Sang KH, Levenson J, Megnien JL, Simon A,. 119). 120) 121) 122) 123). 124). 125) 126) 127). 128). 129) 130). 131) 132). 133) 134). De-vynck MA. Platelet cytosolic Ca2+ and membrane dynamics in patients with primary hypercholesterolemia: Effects of pravast-atin. Arterioscler Thromb Vasc Biol 1995;15:759-64. Eriksson M, Egberg N, Wamala S, Orth-Gomer K, Mittleman MA, Schenck-Gustafsson K. Relationship between plasma fibrinogen and coronary heart disease in women. Arterioscler Th-romb Vasc Biol 1999;19:67-72. Rosenson RS. Viscosity and ischemic heart disease. J Vasc Med Biol 1993;4:206-12. Rosenson RS, Tangney CC. Beneficial effects of statins. Lancet 1996;348:1583. Saacsohn J, Setaro JF, Nicholas C, et al. Effects of lovastatin therapy on plasminogen activator inhibitor-1 antigen levels. Am J Cardiol 1994;74:735-7. Davidson M, McKenney J, Stein E, et al. Comparison of one-year efficacy and safety of atorvastatin versus lovastatin in primary hypercholesterolemia. Am J Cardiol 1997; 79:1475-81. Koenig W, Hehr R, Ditschuneit HH, et al. Lovastatin alters blood rheology in primary hyperlipoproteinemia: Dependence on lipoprotein(a)? J Clin Pharmacol 1992; 32:539-45. Koppensteiner R, Minar E, Ehringer H. Effect of lovastatin on hemorheology in type II hyperlipoproteinemia. Atherosclerosis 1990;83:53-8. Mayer J, Eller T, Brauer P, et al. Effects of long-term treatment with lovastatin on the clotting system and blood platelets. Ann Hematol 1992;64:196-201. Beigel Y, Fuchs J, Snir M, Green P, Lurie Y, Djaldetti M. Lovastatin therapy in hypercholesterolemia: Effect on fibrinogen, hemorheologic parameters, platelet activity, and red blood cell morphology. J Clin Pharmacol 1991; 31:512-7. Tsuda Y, Satoh K, Kitadai M, et al. Effects of pravastatin sodium and simvastatin on plasma fibrinogen level and blood rheology in type Ⅱ hyperlipoproteinemia. Atheroclerosis 1996;122:225-33. Wada H, Mori Y, Kaneko T, et al. Hypercoagulable state in patients with hypercholesterolemia:effects of pravastatin. Clin Ther 1992;14:829-34. Branchi A, Rovellini A, Sommariva D, Gugliandolo AG, Fasoli A. Effect of three fibrate derivatives and of two HMG-CoA reductase inhibitors on plasma fibrinogen level in patients with primary hypercholesterolemia. Throb Haemostasis 1993;70:241-3. Bo M, Bonino F, Neirotti M, et al. Hemorheologic and coagulative pattern in hypercholesterolemic subjects treated with lip-id-lowering drugs. Angiology 1991;42:106-13. Marais AD, Firth JC, Bateman ME, Byrnes P, Martens C, Mountney J. Atorvastatin:An effective lipid-modifying agent in familial hypercholesterolemia. Arterioscler Thro-b Vasc Biol 1997;17:1527-31. Wierzbicki AS, Lumb PJ, Semra YK, Crook MA. Effect of atorvastatin on plasma fibrinogen. Lancet 1998;51: 69-70. Behague I, Poirier O, Nicaud V, et al. Fibrinogen gene polymorphisms are associated with plasma fibrinogen. 135) 136). 137). 138). 139). 140). 141). 142). 143). 144). 145) 146) 147). 148). and coronary artery disease in patients with myocardial infarction: The ECTIM Study. Circulation 1996;93:440-9. Rosenson RS, Tangney CC, Hafner JM. Intraindividual variability of fibrinogen levels and cardiovascular risk profile. Arterioscler Thromb 1994;14:1928-32. The Writing Group for the PEPI Trial. Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in post-menopausal women: The Postmenopausal Estrogen/ Progestin Interventions (PEPI) Trial. JAMA 1995;273:199-208. Meade TW, Ruddock V, Stirling Y, Chakrabarti R, Miller GH. Fibrinolytic activity, clotting factors, and long-term incidence of ischaemic heart disease in the Northwick Park Heart Study. Lancet 1993;342:1076-9. Hamsten A, Wiman B, De Faire U, Blomback M. Increased plasma levels of a rapid inhibitor of tissue plasminogen activator in young survivors of myocardial infarction. N Engl J Med 1985;313:1557-63. Juhan-Vague I, Pyke SDM, Alessi MC, Jespersen J, Haverkate F, Thompson SG, for the ECAT Study Group. Fibrin-olytic factors and the risk of myocardial infarction or sudden death in patients with angina pectoris. Circulation 1996;94:2057-63. Koh KK, Mincemoyer R, Bui MN, Csako G, Pucino F, Guetta V, et al. Effects of hormone-replacement therapy on fibri-nolysis in postmenopausal women. N Engl J Med 1997;336:683-90. Brown SL, Sobel BE, Fujii S. Attenuation of the synthesis of plasminogen activator inhibitor type I by niacin: A potential link between lipid-lowering and fibrinolysis. Circulation 1995;92:767-72. Zambrana JL, Velasco F, Castro P, Concha M, Valles F, Montilla P, et al. Comparison of bezafibrate versus lovastatin for lowering plasma insulin, fibrinogen, and plasminogen activator inhibi-tor-1 concentrations in hyperlipemic heart transplant patients. Am J Cardiol 1997;80: 836-40. Wada H, Mori Y, Kaneko T, Wakita Y, Nakase T, Minamikawa K, et al. Elevated plasma levels of vascular endothelial cell markers in patients with hypercholesterolemia. Am J Hematol 1993;44:112-6. Mitropoulos KA, Armitage JM, Collins R, et al. Randomized placebocontrolled study of the effects of simvastatin on haemo-static variables, lipoproteins and free fatty acids. Eur Heart J 1997;18:235-41. Bevilacqua M, Bettica P, Milani M, et al. Effect of fluvastatin on lipids and fibrinolysis in coronary artery disease. Am J Cardiol 1997;79:84-7. Stein JH, Rosenson RS. Lipoprotein (a) and coronary heart disease. Arch Intern Med 1997;157:1170-6. Kostner GM, Gavish D, Leopold B, Bolzano K, Weintrauvb MS, Breslow JL. HMG CoA reductase inhibitors lower LDL cholesterol without reducing Lp (a) levels. Circulation 1989;80:1313-9. Hunninghake CB, Stein EA, Mellies MJ. Effects of one year of treatment with pravastatin, an HMG-CoA reductase inhibitor, on lipoprotein (a). J Clin Pharmacol 1993; 33:574-80.. 1031.
(17)
수치

관련 문서
Conclusions: Lipid lowering therapy with statins protected against the development of diabetic macular edema and progression of diabetic retinopathy in patients with type
Effects of PCB-77 on total serum cholesterol and VLDL cholesterol concentrations, lipid deposition within the liver and abdominal cavity, and atherosclerosis in ApoE –/–
elevated CRP, and pyuria are the risk factors of coronary artery abnormalities. Bayers et al. 17) reported that an elevated neutrophil count, an elevated ESR, low albumin, and
in young men with familial hypercholesterolemia. Improvement of impaired myocardial vasodilatation due to diffuse coronary atherosclerosis in hypercholesterolemics
Effect of naringin and lovastatin on serum lipid profiles, serum GOT, GPT and fatty streak in rabbits with 1.0% cholesterol diet all values mean±standard deviation 1% cholesterol
of diabetic patients with coronary heart disease. Statin; effecive antiatherosclerotic therapy.. Beyound lipid lowering: the role of statins in vascular
The presence of coronary artery calcification was correlated to risk factors of cardiovascular disease (age, blood pressure, triglyceride, HDL cholesterol, LDL cholesterol,
Albumin content of serum was significantly increased in GP groups, while total lipid, cholesterol and triglyceride of serum were significantly decreased in GP
