대한외과학회지:제 71 권 제 1 호
□ Case Report □
Vol. 71, No. 1, July, 2006
69
INTRODUCTION
Adenosquamous carcinoma of the pancreas is a rare tumor and it constitutes approximately 2% of all the pancreatic cancers.(1) This rare tumor is histopathologically characterized by variable propor- tions of the glandular elements of adenocarcinoma and components of squamous cell carcinoma. There are a variety of hypotheses about the histogenesis of adenosquamous carcinoma and these include the theory of a primitive cell capable of differentiating into either squamous or adenocarcinoma, the theory of squamous metaplasia, and the theory of collision that suggests histologically different tumors arise independently and then they join or coalesce.(2,3) The clinical outcome of this tumor is similar to that of conventional ductal adenocarcinoma. Here, we de- scribe a rare case of adenosquamous carcinoma of the pancreas.
CASE REPORT
In April 2005, a 47-year-old woman was admitted to our hospital with a 3-week history of epigastric discomfort and left upper quadrant pain. She was previously healthy and she denied the use of any medications. There was no history of abdominal surgery or diabetes mellitus. The family history was unremarkable. The patient reported a weight loss of 7 kg during the previous 6 months, and she was thin on the physical examination. She complained of mild tenderness over the left upper quadrant area, but there was no palpable mass. The laboratory data was within the normal range, except for the high preop- erative serum CA 19-9 (4019.08 U/ml) and CEA level
췌장의 선편평 암종
정준철․최성호․장기택
1․조성호․허진석․최동
욱․김용일
Adenosquamous carcinoma of the pancreas is a rare tumor;
its clinical features and radiologic findings are not well known, so the definite preoperative diagnosis of this tumor is quite difficult. We report a case of adenosquamous carci- noma of the pancreas. A 47-year-old woman was admitted on April 2005 to our hospital with a complaint of left upper quadrant pain. The serum CA 19-9 and CEA level were increased up to 4019.08 U/ml and 13.13 ng/ml, respectively.
An abdominal computed tomographic (CT) revealed a 10×9 cm sized well-defined homogenous lobulated mass in the pancreas tail. Under the impression of solid-pseudopapillary neoplasm (SPN) or nonfunctioning islet cell tumor, distal pan- createctomy and splenectomy with wedge resection of stom- ach were performed. The specimen consisted of a huge pancreatic mass that was attached to the posterior wall of stomach. The cut surface of pancreatic mass revealed a huge whitish infiltrative mass. Microscopically, glandular elements of ductal adenocarcinoma were admixed with solid squamoid complexes or squamous cell carcinoma compo- nents. Although the origin of the adenosquamous carcinoma has not been well proven, the histopathological findings of our case support the theory of squamous metaplasia. (J Korean Surg Soc 2006;71:69-72)
Key Words: Pancreas, Adenosquamous, Carcinoma, Squa- mous, Metaplasia
중심 단어: 췌장, 선편평, 암종, 편평, 화생
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
성균관대학교 의과대학 삼성서울병원 외과,
1병리과
Adenosquamous Carcinoma of the Pancreas
Departments of Surgery and
1Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Jun Chul Chung, M.D., Seong Ho Choi, M.D., Kee-Taek Jang, M.D.
1, Sung Ho Jo, M.D., Jin Seok Heo, M.D., Dong Wook Choi, M.D. and Yong Il Kim, M.D.
책임저자:최성호, 서울시 강남구 일원동 50 ꂕ 135-710, 삼성서울병원 외과 Tel: 02-3410-3469, Fax: 02-3410-0040 E-mail: [email protected]
접수일:2005년 11월 24일, 게재승인일:2006년 2월 6일 본 논문은 2005년 10월 대한외과학회 추계학술대회에서 발표되었음.
70
대한외과학회지:제 71 권 제 1 호 2006ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
(13.13 ng/ml). An abdominal CT scan revealed a 10
×9 cm sized well-defined homogenous mass in the pancreas tail (Fig. 1). Exploratory laparotomy was performed under the impression of SPN or nonfunc- tioning islet cell tumor. At laparotomy, the mass was identified in the pancreas tail. It was adhered to the splenic hilum and the posterior wall of the stomach.
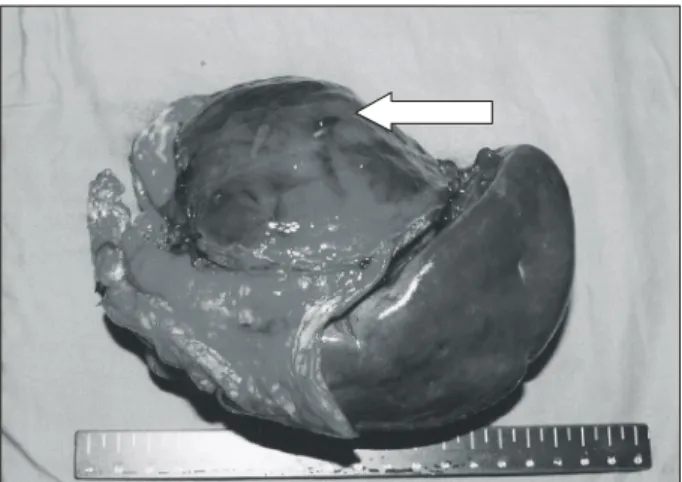
Distal pancreatectomy, splenectomy and wedge re- section of the stomach were performed by the com- plete, en bloc resection of the mass. The specimen consisted of a huge pancreatic mass measuring 9×8
×8 cm that was attached to the splenic hilum and posterior wall of stomach (Fig. 2). On serial section, the tumor showed invasion to the splenic hilum, extension to the submucosal layer of the stomach and
peripancreatic soft tissue, and adhesion to the adre- nal gland. Microscopically, glandular elements of ductal adenocarcinoma were admixed with solid squamoid complexes or squamous cell carcinoma components (Fig. 3). The glandular component gen- erally exhibited moderately to poorly differentiated ductal adenocarcinoma. The glandular components of ductal adenocarcinoma were surrounded by squamous cell carcinoma components. The invasion to stomach, spleen and peripancrancreatic soft tissue was by the squamous cell carcinoma component. The lymph node metastasis was also squamous cell carci- noma (Fig. 4). The final pathological diagnosis was adenosquamous carcinoma of the pancreas.
Fig. 1. Computed tomography revealed a huge pancreatic tail mass that measured about 10 cm, and it was attached to the splenic hilum and the posterior wall of the stomach (marked with an arrow).
Fig. 2. The upper surface of the tumor is covered with the mucosa of the stomach (marked with an arrow).
Fig. 3. Histology of the adenosquamous carcinoma demonstrated ductal adenocarcinoma with squamous metaplasia (H&E,
×200).
Fig. 4. The tumor cell type of the lymph node metastasis was
squamous cell carcinoma (H&E, ×200).
Jun Chul Chung, et al:Adenosquamous Carcinoma of the Pancreas
71
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
DISCUSSION
Adenosquamous carcinoma of the pancreas is a rare aggressive subtype of pancreatic cancer with an extremely poor survival rate, and it is often called mucoepidermoid carcinoma or adenoacanthoma. (4-6) The incidence of this unusual tumor is really not known, but the estimates from a review of the literature have been demonstrated its incidence to be 1% to 4% of all pancreatic malignancies,(7-9) even though higher rates of 9% to 11% have been reported in Japan.(4,6,10) Since the pancreas is entirely devoid of squamous cell components, several theories for the origin of this tumor have been proposed. These in- clude the theory of a pleuripotent primitive cell that is capable of differentiating into squamous cell carci- noma or adenocarcinoma, the theory of squamous metaplasia as a result of ductal inflammation or chronic pancreatitis, and the theory of collision that suggests histologically different tumors arise inde- pendently and then join or coalesce.(2,3) Although the origin of the adenosquamous carcinoma has not been well proven, the most favored origin is the squamous metaplasia theory.(11) Yamaguchi and Enjoji (10) reported that there was a close relation- ship between the glandular elements and the squa- mous components in all eight of the tumors in their study. Adenocarcinoma was generally situated at the center of the tumor and the squamous cell carcinoma was located at the periphery of the neoplasm, so they suggested that the squamous components were the result of metaplastic change of the pre-existing ductal adenocarcinoma. Onoda et al.(12) reported that the adenocarcinoma cells were located at the center of tumors and these were surrounded by layers of epidermoid cells, so they suggested that the epider- moid cells seemed to be derived from the adenocar- cinoma cells. In our current case, the focal glandular components of the ductal adenocarcinoma were sur- rounded by squamous cell carcinoma components with metaplastic change of the ductal adenocarci- noma. The histopathological findings of our case support the theory of squamous metaplasia.
Although there have recently been an increasing number of case reports of adenosquamous carcinoma of the pancreas, the accurate preoperative diagnosis
of this lesion is difficult. Madura et al.(11) reported that most patients were in the sixth decade of life with a slight male predominance (1.5 : 1), and the tumors were slightly predominant in the head of the pancreas. However, the clinical features were similar to conventional ductal adenocarcinoma of the pan- creas, and there were no radiologic characteristics to differentiate it from the common exocrine tumors of the pancreas.(13) In our case, we performed explora- tory laparotomy under the impression of SPN or nonfunctioning islet cell tumor. On gross examina- tion, SPN is generally a well-encapsulated, spherical mass that usually measures around 8 to 10 cm. The cut surface shows characteristic hemorrhage and cystic degeneration.(14,15) Nonfunctioning islet cell tumor is most likely when the blood supply becomes insufficient as the tumor grows larger and there is consequent necrosis or cyst formation.(16) A few re- ports for the differential diagnosis of this tumor have recently been published. A report by Nabae et al.(17) described that the presence of central necrosis in a huge infiltrative pancreatic tumor seemed to be sug- gestive of the diagnosis of adenosquamous carcino- ma of the pancreas. Yet our case did not reveal any cystic change, even though the tumor was of a large size. A report by Kuji et al.(18) suggested that these lesions may selectively take up gallium-67 citrate on scintigraphy. Other authors have described the use- fulness of preoperative percutaneous examinations and intraoperative frozen examinations, but these procedures have the high risk of peritoneal seeding of the malignant cells and have little influence on the decision-making and the patients' survival. So, these procedures usually do not be recommended.(19) There have been some reports concerning the mo- lecular alterations. Campman et al.(20) and Ohtsubo et al.(21) reported on cases of adenosquamous carci- noma of the pancreas with K-ras point mutation and p53 overexpression. Kardon et al.(22) reported that K-ras oncogene mutations were identified in seven of 13 cases.
The prognosis of adenosquamous carcinoma of the
pancreas is usually very poor. Baylor and Berg (9)
reported that only 1 of 47 patients (2.1%) lived more
than 10 months. Cihak et al.(2) reported that the time
of survival from the onset of symptoms to death
ranged from 4 to 13 months, with a mean survival
72
대한외과학회지:제 71 권 제 1 호 2006ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ period of 9 months. Yamaue et al.(23) reported on a
63-year old female patient with adenosquamous car- cinoma of the pancreas who underwent extended ra- dical surgery, intraoperative radiation therapy, post- operative intra-arterial chemotherapy and external beam radiation therapy, and she had survived for 40 months after surgery. They emphasized the beneficial effects of such multidisciplinary treatment on patient survival.
REFERENCES
1) Adsay V, Hasteh F, Sarkar F, Vaitkevicius V, Cheng J, Klimstra D. Squamous cell and adenosquamous carcinoma of the pancreas: a clinicopathologic analysis of 11 cases.
Mod Pathol 2000;13:179A.
2) Cihak RW, Kawashima T, Steer A. Adenoacanthoma (ad- enosquamous carcinoma) of the pancreas. Cancer 1972;29:
1133-40.
3) Itani KMF, Karni A, Green L. Squamous cell carcinoma of the pancreas. J Gastrointest Surg 1999;3:512-5.
4) Ishikawa O, Matsui Y, Aoki I, Iwanaga T, Terasawa T, Wada A. Adenosquamous carcinoma of the pancreas: a clinico- pathologic study and report of three cases. Cancer 1980;
46:1182-6.
5) Makiyama K, Takuma K, Zea-Iriarte WL, Ikunn N, Kawatomi M, Mori N, et al. Adenosquamous carcinoma of the pancreas. J Gastroenterol 1995;30:798-802.
6) Myung SJ, Kim MH, Lee SK, Seo DW, Kim YS, Min YI.
Adenosquamous carcinoma of the pancreas: differentiation from pancreatic pseudocyst. Gastrointest Endosc 1998;47:
410-3.
7) Cubilia AL, Fitzgerald PJ. Morphological patterns of prima- ry nonendocrine human pancreas carcinoma. Cancer Res 1975;35:2234-48.
8) Chen J, Baitkun SI. Morphological study of 391 cases of exocrine pancreatic tumors with special reference to the classification of exocrine pancreatic carcinoma. J Pathol 1985;146:17-29.
9) Baylor SM, Berg JW. Cross-classification and survival characteristics of 5,000 cases of cancer of the pancreas. J Surg Oncol 1973;5:335-58.
10) Yamaguchi K, Enjoji M. Adenosquamous carcinoma of the pancreas: a clinicopathologic study. J Surg Oncol 1991;47:
109-16.
11) Madura JA, Jarman BT, Doherty MG, Yun MN, Howard TJ.
Adenosquamous carcinoma of the pancreas. Arch Surg
1999;134:599-603.
12) Onoda N, Kang SM, Sugano S, Yamashita Y, Chung YS, Sowa M. Mucoepidermoid carcinoma of the pancreas: re- port of a case. Surg Today 1995;25:843-7.
13) Murakami Y, Yokoyama T, Yokoyama Y, Kanehiro T, Uemura K, Sasaki M, et al. Adenosquamous carcinoma of the pancreas: preoperative diagnosis and molecular altera- tions. J Gastroenterol 2003;38:1171-5.
14) Mancini GJ, Dudrick PS, Grindstaff AD, Bell JL. Solid pseudopapillary tumor of the pancreas: two cases in male patients. Am Surg 2004;70:29-31.
15) Huang HL, Shih SC, Chang WH, Wang TE, Chen MJ, Chan YJ. Solid-pseudopapillary tumor of the pancreas: clinical experience and literature review. World J Gastroenterol 2005;11:1403-9.
16) Kato K, Kondo S, Ambo Y, Omi M, Hirano S, Morikawa T, et al. Nonfunctioning endocrine tumor of the pancreas with extrapancreatic growth and cyst formation: report a case. Surg Today 2003;30:651-4.
17) Nabae T, Yamaguchi K, Takahata S, Utsunomija N, Ma- tsunaga H, Sumiyoshi K, et al. Adenosquamous carcinoma of the pancreas: report of two cases. Am J Gastroenterol 1998;93:1167-70.
18) Kuji I, Sumiya H, Taki J, Nakajima K, Yokoyama K, Kinuya S, et al. Intense Ga-67 uptake in adenosquamous carcinoma of the pancreas. Ann Nucl Med 1997;11:41-3.
19) Lozano MD, Panizo A, Sola IJ, Pardo-Mindan FJ. FNAC guided by computed tomography in the diagnosis of primary pancreatic adenosquamous carcinoma. A report of three cases. Acta Cytol 1998;42:1451-4.
20) Campman SC, Fajardo MA, Rippon MB, Kraegel SA, Ruebner BH. Adenosquamous carcinoma arising in a mu- cinous cystadenoma of the pancreas. J Surg Oncol 1997;64:
159-62.
21) Ohtsubo K, Mouri H, Sakai J, Akasofu M, Yamaguchi Y, Watanabe H. Pancreatic cancer associated with granulocyte- colony stimulating factor production confirmed by immuno- histochemistry. J Clin Gastroenterol 1998;27:357-60.
22) Kardon DE, Thompson LD, Przygodzki RM, Heffess CS.
Adenosquamous carcinoma of the pancreas: a clinicopath- ologic series of 25 cases. Mod Pathol 2001;14:443-51.
23) Yamaue H, Tanimura H, Onishi H, Tani M, Kinoshita H, Kawai M, et al. Adenosquamous carcinoma of the pancreas:
successful treatment with extended radical surgery, intraop- erative radiation therapy, and locoregional chemotherapy.
Int J Pancreatol 2001;29:53-8.